
Abstract
A diabetic sexagenarian presented with exertional dyspnea and was diagnosed to have moderate mitral regurgitation. We present an interesting sign that was picked up during echocardiographic evaluation, which gave a clue regarding the etiology of mitral regurgitation and aided in further management.
Case Description
A diabetic sexagenarian presented with exertional dyspnea for the last few weeks. Examination showed normal general physical examination, with a pulse rate of 88 bpm and blood pressure of 128/76 mmHg. Cardiovascular examination showed mild cardiomegaly, with an LVS3 and a grade 2/6 holosystolic murmur at the cardiac apex radiating to the axilla and inferior angle of the scapula. The echocardiogram showed fair left ventricular (LV) function with moderate mitral regurgitation (MR). A detailed echocardiographic evaluation was done to identify the etiology of MR. There was no valvar/sub-valvar apparatus thickening, commissural fusion or calcification indicative of rheumatic etiology or valve displacement above the annular plane, suggesting mitral valve prolapse (MVP). The chordal attachment to the valve was intact. The anterior mitral leaflet (AML) appeared tented, leading to non-coaptation, and regional wall motion abnormality (RWMA) was noted in the inferior wall (Figure 1A-1D, Video 1), suggesting an ischemic etiology.
(A) Apical Five-chamber View Showing Tethering of Anterior Mitral Leaflet (AML) Creating a Wing of Seagull Appearance—“Seagull Sign”. Note the Resultant Coaptation Defect. (C) Strut Chordae Attached to AML, Causing Tethering, Leading to Non-coaptation (B, D) Mitral Regurgitation (MR) Through the Coaptation Defect. (E, F) Pictorial Representation of the Mechanism of MR.
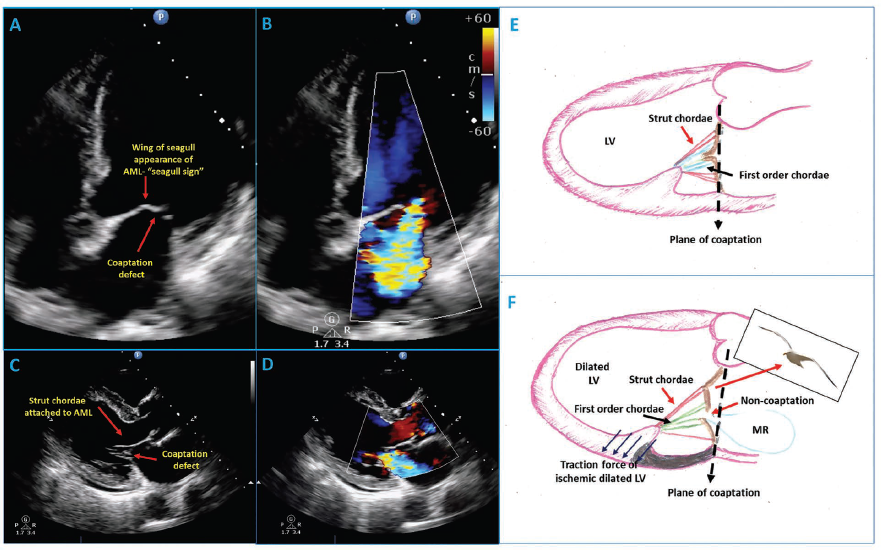
Ischemic MR develops by various mechanisms. LV enlargement and annular dilatation lead to Carpentier type I MR. Whereas, papillary muscle displacement secondary to LV remodeling leading to leaflet tethering and non-coaptation results in Carpentier type IIIb MR. 1 Lam et al. classified chordae tendineae (CT) attaching to the rough zone of AML into commissural, para-commissural, strut and paramedian chordae, of which strut chordae are the thickest and form the skeleton. Tandler and Quain classified CT into first, second, and third orders based on attachment to the edge, belly, and base of leaflets. The AML tethering by secondary strut chordae gives rise to the wing of the seagull appearance of AML—seagull sign, which leads to non-coaptation (Figure 1A-1F). This is seen in inferior wall myocardial infarction with RWMA in basal segments. The cutting of this strut chordae is studied to be an effective procedure to reduce MR in these patients. 1 The patient subsequently underwent a coronary angiogram, which showed triple vessel disease and is awaiting coronary artery bypass grafting along with mitral valve repair.
Learning Points
Echocardiographic evaluation to define the MR mechanism is critical and aids in choosing appropriate therapeutic intervention.
In inferior wall myocardial infarction, tethering of AML by secondary strut chordae leads to non-coaptation and secondary MR.
The surgical release of this strut chordae is an effective procedure to reduce MR in such patients.
Footnotes
Authors’ Contributions
SSK—Conceptualization: Equal; Formal analysis: Lead; Writing—original draft: Lead; Writing—review & editing: Lead); SM—Conceptualization: Equal; Investigation: Equal; Supervision: Equal; SKG—Investigation: Equal; Conceptualization: Equal; Formal analysis: Lead; Writing—review & editing: Lead.
Data Availability Statement
All data are incorporated into the article and its online supplementary material.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as it is an anonymous case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Obtained from the patient in line with COPE guidance.
Supplemental Material
Supplemental material for this article is available online.