
Abstract
Hypertension, the most common modifiable risk factor for “cardiovascular disease” burden, with mortality risk doubling for each 20/10 mmHg blood pressure increase above 115/75 mmHg. While brachial cuff blood pressure is commonly used, it often fails to accurately reflect central aortic pressures, which have a direct impact on target organs. It also tends to underestimate systolic blood pressure and overestimate diastolic blood pressure. Therefore, accurate blood pressure measurement is crucial for diagnosis and risk assessment.
Materials and Methods
This cross-sectional observational study was performed at Kilpauk Medical College. Intra-arterial aortic, brachial, and noninvasive cuff brachial pressures were measured in 100 patients undergoing elective coronary angiography. Systolic blood pressure, diastolic blood pressure, and pulse pressure were assessed to determine the relationship between invasive and noninvasive measurements.
Results
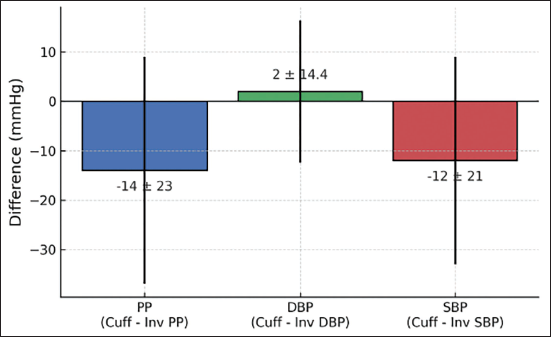
Cuff systolic blood pressure (132 ± 16 mmHg) was significantly lower than invasive brachial systolic blood pressure (144 ± 14 mmHg; P < .001). Relative to invasive brachial measurements, cuff systolic blood pressure was 12 mmHg lower (95% confidence interval: –16.1 to –7.9; P < .001), diastolic blood pressure was 2 mmHg higher (95% confidence interval: –0.8 to 4.8; P = .04), and PP was 14 mmHg lower (95% confidence interval: –18.5 to –9.5; P < .001).
Conclusion
Significant discrepancies exist between invasive and cuff-based systolic blood pressure measurements. Cuff-based blood pressure consistently underestimates true systolic blood pressure and pulse pressure, which may lead to hypertension underdiagnosis, particularly in patients with increased arterial stiffness. Invasive blood pressure measurements are thus more appropriate for precise assessment in high-risk populations.
Keywords
Introduction
The most prevalent modifiable risk factor for lowering cardiovascular morbidity and mortality is controlling elevated blood pressure (BP). 1 It is well established that the site of BP measurement alters the systolic blood pressure (SBP) values. 2 Even while brachial artery cuff BP is the most often used method for measuring BP and monitoring its treatment, it may not always accurately represent intra-arterial BPs in the brachial or aortic arteries. 3 Wave reflection raises pulse pressure (PP), frequently leading to a higher brachial SBP than aortic SBP. However, PP amplification decreases with age due to artery stiffening, which can lead to isolated systolic hypertension.4–6 Waveform reflection from peripheral impedance mismatch points and variations in arterial tree stiffness are the primary factors influencing the difference between central as well as peripheral BP. 7 Additionally, central aortic BP, pressure exerted directly on brain, heart, and kidneys, is more strongly linked to cardiovascular events and target organ damage as opposed to brachial BP.8–10 There is mounting evidence that this measurement differs from arm BP due to an amplification effect that increases central BP, implying that central aortic pressure is a more meaningful prognostic indicator than brachial BP. In fact, cuff diastolic blood pressure (DBP) consistently overestimates intra-arterial brachial DBP, whereas cuff SBP consistently underestimates intra-arterial brachial SBP by about 6 mmHg on average. 11 These findings underscore the need for accurate, method-specific BP assessment to ensure proper diagnosis, risk stratification, and treatment of systemic hypertension.
Aim
In the present research, we sought to investigate the relationship between aortic and brachial invasive BP, noninvasive cuff pressure, and augmentative pressure, as well as their significance. A better understanding of the mechanisms underlying cuff BP discrepancies could help refine accuracy and improve individual BP risk stratification.
Methodology
Materials and Methods
Study Design
The present cross-sectional observational study was carried out in the Department of Cardiology at the Government Medical College and Hospital. The study population included 100 patients admitted for elective coronary angiography over 6 months. Institutional Ethics Committee approval was obtained before study initiation as well as written informed consent was secured from all participants. Inclusion criteria encompassed adult patients (>18 years) undergoing elective angiography for angina. Exclusion criteria included patients with interarm BP variation greater than 5 mmHg, a history of previous arrhythmias, chronic kidney disease, pregnant women, and age less than 18 years. Baseline demographic information, clinical profile, cuff brachial BP, invasive brachial BP, and invasive aortic BP measurements were recorded. Hypertension was defined as brachial SBP ≥130 mmHg or DBP ≥80 mmHg as per the 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines. 1
Invasive and Noninvasive Blood Pressure Measurements
All hemodynamic measurements had been obtained with the patient in the supine position, just before coronary angiography. A 5F Judkins catheter (Terumo, Cordis) was introduced through the right radial access to assess invasive aortic SBP and DBP. The catheter was positioned in the ascending aorta, 3-5 cm above the aortic valve, and central aortic pressures were recorded. Subsequently, the catheter was withdrawn to the mid-humerus level to obtain invasive brachial pressure waveforms. The peak of the ensembled waveform was recorded as the invasive SBP, while the lowest point was regarded as the invasive DBP. The transducer was positioned at heart level, and this system had been calibrated and flushed before each acquisition of the invasive central as well as brachial BP waveforms. Simultaneously, noninvasive brachial cuff BP was measured on the left arm using a validated automated oscillometric cuff BP device, “Omron HEM 7156.”
Blood Pressure Indices and Definitions
Invasive blood pressure amplification (BPA) had been defined as the difference between invasive brachial BP as well as invasive aortic BP. Specifically, subtracting invasive brachial pressure from invasive aortic BP provided the values for invasive systolic, diastolic, and PP amplification. Additionally, the noninvasive (cuff) SBP and DBP, along with PP difference, were calculated by subtracting the corresponding invasive brachial measurements from the cuff measurements.
Statistical Analysis
Descriptive statistics had been applied to all demographic and clinical variables. Continuous variables had been expressed as means ± standard deviations, and categorical variables as frequencies and percentages. Independent t-tests were performed to compare two distinct groups. For comparisons between more than two groups, one-way analysis of variance (ANOVA) was employed; when significant, post hoc pairwise comparisons were performed employing Tukey’s honest significant difference (HSD) test to identify specific group differences. The agreement between cuff and invasive brachial SBP readings was evaluated by calculating the mean difference and standard deviation of the two methods. The difference between cuff SBP and invasive brachial SBP was quantified as the “cuff SBP discrepancy” for each participant, with negative values indicating underestimation. Trend analysis was conducted to explore associations between physiological systolic blood pressure amplification (SBPA) (the invasive brachial SBP minus invasive aortic SBP) and these cuff SBP discrepancies.
Results
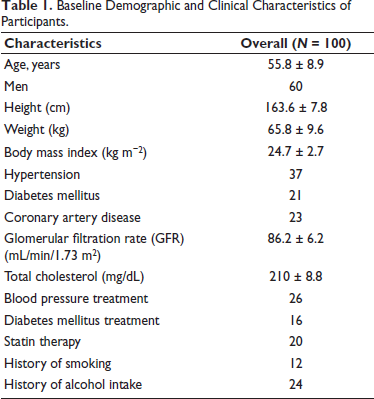
The study included 100 participants with a mean age of 55.8 ± 8.9 years; 60% were male. The average height and weight were 163.6 ± 7.8 cm and 65.8 ± 9.6 kg, respectively. The mean body mass index (BMI) was 24.7 ± 2.7 kg/m2, with the majority of individuals falling within the normal weight range. Approximately 37% of participants were known to be hypertensive, and 21% had diabetes mellitus. A history of coronary artery disease was reported in 23% of patients. The mean estimated glomerular filtration rate (GFR) was 86.2 ± 6.2 mL/min/1.73 m2, indicating that most participants had preserved renal function. Serum total cholesterol levels averaged 210 ± 8.8 mg/dL, slightly higher than standard guideline thresholds of <200 mg/dL.
Among hypertensives, 67% (n = 26) of participants were on hypertension medications. The most frequently prescribed medications for hypertension treatment were calcium-channel blockers (56%). Among diabetics, 16% were taking regular medications. About 20% of the population were on statin therapy. Regarding lifestyle factors, 12% of participants reported smoking, and 24% were alcoholics. Hypertension was less common in women (16%) than in men (22%) in our study. Approximately 48% of hypertensive patients were above 55 years of age (Table 1).
Baseline Demographic and Clinical Characteristics of Participants.
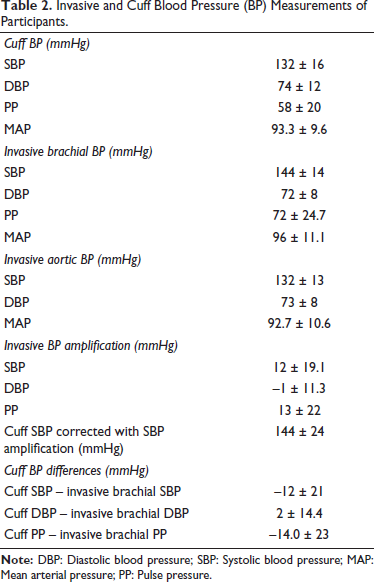
Cuff brachial SBP (132 ± 16 mmHg) was significantly lower than invasive brachial SBP (144 ± 14 mmHg; P < .001) (Figure 1). The invasive aortic SBP was 132 ± 13 mmHg, while the DBP was 73 ± 8 mmHg. The cuff measurements for SBP, DBP, PP, and mean arterial pressure (MAP) were 132 ± 16, 74 ± 12, 58 ± 20, and 93.3 ± 9.6 mmHg, respectively (Table 2). Compared with invasive brachial measurements, cuff SBP was lower by –12 mmHg (95% CI: –16.1 to –7.9; P < .001), DBP was higher by 2 mmHg (95% CI: –0.8 to 4.8; P = .01), and PP was lower by –14 mmHg (95% CI: –18.5 to –9.5; P < .001) (Figure 2).
Cuff Versus Invasive Brachial Blood Pressure (BP) Differences.
Invasive and Cuff Blood Pressure (BP) Measurements of Participants.
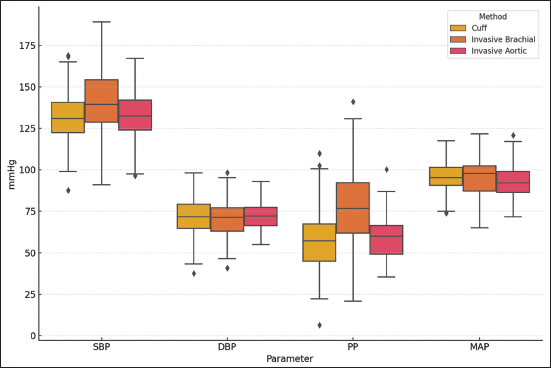
Boxplot of Blood Pressure (BP) Parameters by Measurement Method.
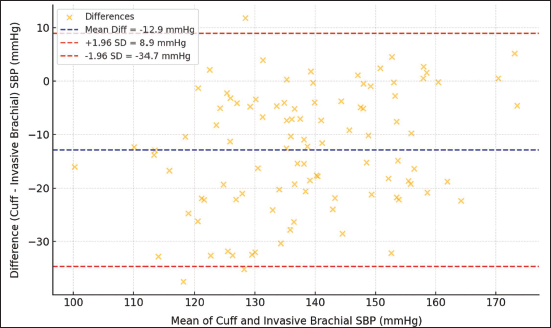
The agreement between cuff SBP and invasive brachial SBP was further assessed using Bland–Altman analysis (Figure 3), revealing a mean bias of –12.9 mmHg (indicating cuff underestimation) with 95% limits of agreement ranging from –34.7 to 8.9 mmHg. The average physiological SBPA (defined as invasive brachial SBP minus invasive aortic SBP) was 12 ± 19.1 mmHg. Interestingly, the mean difference between cuff SBP and invasive brachial SBP (representing cuff SBP underestimation) was –12 ± 21 mmHg, indicating that the cuff measurement often underestimated the true brachial SBP by a magnitude similar to the physiological amplification observed. However, this numerical similarity is coincidental and does not imply a direct causal link.
Bland–Altman Plot: Cuff Systolic Blood Pressure (SBP) Versus Invasive Brachial SBP.
The cuff brachial, invasive brachial, and invasive aortic measurement groups showed a significant difference in SBP (F(2, 297) = 7.84, P < .001) according to a one-way ANOVA, but there was no significant difference in DBP across the groups (F(2, 297) = 1.06, P = .35) (Table 3). Although there was no significant difference between cuff and invasive aortic SBP, Tukey’s HSD post hoc analysis showed that cuff brachial SBP was considerably lower than invasive brachial SBP (mean difference = –12 mmHg, 95% CI: –16.1 to –7.9, P < .001). Additionally, the mean difference between invasive brachial and invasive aortic SBP was +12 mmHg, 95% CI: 7.9-16.1, P < .001 (Table 4).
Analysis of Variance (ANOVA) Test Results.

Tukey’s Honest Significant Difference (HSD) Post Hoc Test Results (Systolic Blood Pressure (BP)).

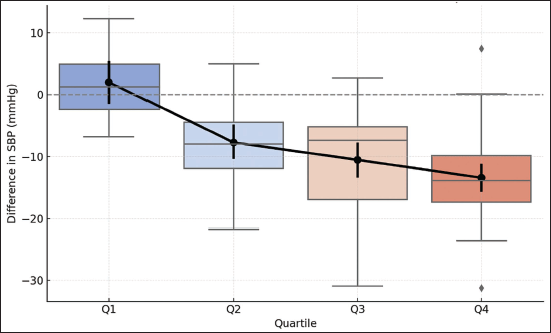
A trend analysis across quartiles of invasive SBPA demonstrated a progressively larger difference between cuff and invasive brachial SBP. In the lowest amplification quartile (Q1, n = 10), the mean difference was minimal, whereas in the highest quartile (Q4, n = 40), the cuff significantly underestimated invasive SBP by approximately 14 mmHg. This pattern showed a statistically significant linear trend (P for trend < .001), indicating that the underestimation by cuff measurements increased with greater SBPA (Figure 4).
Trend in Systolic Blood Pressure (SBP) Difference (Cuff – Invasive Brachial) Across SBP Amplification Quartiles.
Discussion
The most significant modifiable risk factor for cardiovascular disease (CVD) is still hypertension. 12 Hypertension is defined as a DBP of more than 80 mmHg or an SBP of greater than 130 mmHg, under the 2017 AHA/ACC recommendations. The risk of cardiovascular mortality doubles for every 20 mmHg rise in SBP and 10 mmHg increase in DBP over a baseline of 115/75 mmHg. 1
Accurate BP measurement is critical for the proper diagnosis and management of hypertension patients in both outpatient and critical care settings. 13 While the brachial cuff method of BP measurement remains the most common technique for noninvasive BP assessment, mounting evidence suggests that it may significantly underestimate SBP when compared with invasive intra-arterial measurements. 11 The pressure on the heart and brain is known as central (aortic) BP, and it might be different from the pressure measured in the arm. Cardiovascular risk surrogates, such as carotid intima-medial thickness and left ventricular mass, seem to correlate more strongly with central SBP than peripheral SBP. 14 In certain groups, central pressure could be a more accurate indicator of outcome, especially older age groups, and its response varies with different classes of antihypertensive medications.15, 16 The arterial pulse increases from the central to the peripheral arteries as SBP rises, while diastolic and mean BP remain relatively constant. 17
Direct intra-arterial BP assessment demonstrates a physiological increase in SBP from the central to peripheral arteries, known as peripheral BPA, and is a well-known phenomenon.4, 18 The primary mechanism for peripheral amplification of BP is differences in arterial tree stiffness and waveform reflection from peripheral impedance mismatch points. Likewise, the SBPA from the brachial to radial arteries has been described as the Popeye phenomenon.19, 20 According to certain studies, the average increase in invasive SBP from the brachial to radial artery is 4-12 mmHg, while the average noninvasive SBP increase is 6-15 mmHg. 21
In our study, a significant difference between invasive and noninvasive BP measurement was seen. Cuff brachial SBP measured (130 ± 20 mmHg) significantly underestimated invasive brachial SBP (139 ± 20 mmHg), with a mean difference of 12 ± 21 mmHg, P < .001, and cuff-based DBP was slightly overestimated by 2 ± 14.4 mmHg. These discrepancies reflect the limitations of the oscillometric method of BP measurements.
The physiological basis for this underestimation stems from both technical and anatomical factors. Vascular stiffness and arterial compliance, patient positioning while taking BP readings, incorrect cuff size, and hemodynamic instability are all factors that contribute to discrepancies between cuff and invasive measurements. Cuff-based BP measurement methods rely on detecting oscillations in the arterial wall as the cuff deflates, but these oscillations may be difficult to detect in people with stiff arteries, such as those with atherosclerosis or those who are older, resulting in an underestimation of SBP. These devices calculate BP using algorithms that are typically calibrated on healthy subjects and may not perform accurately in patients with vascular stiffness, arrhythmias, or altered hemodynamics.
These findings are consistent with previous studies. For instance, a study by Picone et al. in 2017, which evaluated over 70 studies, concluded that cuff-based measurements underestimated invasive brachial SBP by an average of 5.7 mmHg, while overestimating DBP by approximately 5.5 mmHg. 11 Dankel et al. also reported that SBP was generally underestimated (4.55 mmHg), while DBP was overestimated by 6.20 mmHg using the cuff method, with significant random errors. 22
These discrepancies highlight potential difficulties in accurately estimating intra-arterial BP using the cuff method, which could affect hypertension diagnosis and management. These systematic biases raise concern regarding underdiagnosing hypertension, particularly in patients with borderline BPs for hypertension staging or requiring tight BP control, such as in pregnancy or critical illness. This underscores the critical need for proper arm positioning to obtain accurate BP readings.
Improper positioning of the arm during BP recording or the wrong cuff size can also lead to significantly higher readings. Ebinger et al. demonstrated that when the arm was unsupported, SBP and DBP increased by 6.5 and 4.4 mmHg, respectively, when compared to the arm kept supported at heart level. 23 Similarly, Bilo et al. demonstrated that the use of an inappropriately sized cuff can lead to falsely low SBP readings, particularly in obese patients. 24
In critically ill patients, especially in those with hypotension, BP measured by cuff devices may be more unreliable. Studies by Lakhal et al. and Dunser et al. have shown that in hypotension and septic shock, cuff BP may significantly underestimate invasive values, sometimes by more than 20 mmHg.25, 26 Sharman et al., in a study, found that oscillometric BP devices tend to underestimate actual intra-arterial SBP, particularly in patients with higher arterial stiffness and PP amplification, similar to our study. 27
Interestingly, our study found no significant difference between cuff brachial and invasive aortic SBP, indicating that cuff pressures are underestimated compared to invasive brachial pressures; they may still provide a reasonably accurate estimate of central aortic pressures. These findings are consistent with earlier research by Williams et al., suggesting that cuff SBP may better represent central pressures than peripheral values. 14
The large SBP gradient between invasive brachial and invasive aortic pressure supports the physiological phenomenon of PP amplification, in which pressure rises from peripheral to central arteries, which has been well documented in previous studies, including those by Nichols and O’Rourke. Our findings support the importance of measurement location and technique in interpreting BP, with implications for clinical practice and cardiovascular risk assessment. 28
Notably, the trend analysis revealed that the cuff SBP underestimation (difference between cuff and invasive brachial SBP) widened as physiological SBPA quartiles increased. This is consistent with findings by McEniery et al., which show that peripheral amplification varies greatly between individuals and accounts for the underestimation of SBP by brachial cuff devices. 29
The clinical significance is that patients with larger arterial amplification, typically younger or taller individuals, may be at a higher risk of having their SBP underestimated, potentially affecting diagnosis and treatment. 30
The study’s limitations include an observational design, which limits causal inference and restricts generalizability. Even when device calibration and operator skill are standardized, measurement variability may persist, and invasive measurements may be influenced by catheter placement and waveform processing.
Conclusion and Future Directions
The cuff-based BP measurement tends to underestimate SBP and may not accurately reflect invasive pressures, particularly in critically ill patients, pregnant women, and individuals with increased arterial stiffness. Although brachial cuff-based BP measures remain the most popular method of BP measurement due to their convenience, more accurate alternatives are required in clinical settings where precise BP recordings are critical for decision-making.
Emerging technologies such as ClearSight and Finapres technologies have proven to offer more precise and continuous BP measurements with good resemblance to invasive arterial BP. Similarly, devices using finger-cuff technologies, such as the Vasera and Finometer, have shown improved accuracy in various clinical scenarios compared to standard oscillometric cuffs. Future research should focus on developing more precise cuff-based devices, improving algorithmic methods for noninvasive BP measurement, and investigating the widespread use of continuous noninvasive BP monitoring technologies in diverse patient populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Ethics Committee approval was obtained on 1/6/2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all patients for participation and publication of data.