
Abstract
Introduction
A crucial prognostic marker for patients with ST-elevation myocardial infarction is infarct size. The present study was done to study the relationship between infarct size and invasive hemodynamics in patients with ST-elevation myocardial infarction and its prognostic implications.
Methods
This prospective observational study enrolled 136 patients presenting with ST-elevation myocardial infarction and undergoing primary percutaneous coronary intervention.
Results
Hemodynamic parameters that correlated significantly with left ventricular ejection fraction were left ventricular end-diastolic pressure, cardiac output, systemic vascular resistance, systolic blood pressure/left ventricular end-diastolic pressure ratio, peak creatine kinase-myocardial band, and days of hospitalization. Left ventricular ejection fraction had the strongest correlation with systolic blood pressure/left ventricular end-diastolic pressure ratio (ρ = 0.97) and the second highest correlation with cardiac output (ρ = −0.36). Left ventricular ejection fraction also showed correlation with the number of days of hospitalization with left ventricular ejection fraction (ρ = −0.82) and wall motion score index (ρ = −0.69). Patients with reduced left ventricular ejection fraction, elevated creatine kinase-myocardial band, and wall motion score index experienced prolonged hospital stays, indicative of larger infarct sizes.
Conclusion
Left ventricular end-diastolic pressure and systolic blood pressure/left ventricular end-diastolic pressure ratio provide essential insights into cardiac performance during primary percutaneous coronary intervention. These parameters help clinicians tailor interventions to improve hemodynamics, reduce risks, and enhance patient outcomes. Incorporating these measures into routine practice ensures a more comprehensive approach to managing the hemodynamic complexities in systolic blood pressure/left ventricular end-diastolic pressure ratio patients.
Introduction
The degree of myocardial damage in acute myocardial infarction (AMI) is almost directly correlated with the prognosis. 1 Infarct size refers to the amount of heart muscle that is damaged or dies due to the lack of blood inflow during a heart attack. Infarct size is the strongest determinant of post-myocardial infarction (MI) left ventricular (LV) dysfunction and the compensatory and long-term adverse volumetric changes that occur in response to a low ejection fraction. 2 If evaluated early after an AMI, infarct size (IS) can be used to assess patients’ future risk and to optimize therapy efforts.
In ST-elevation myocardial infarction (STEMI), a large IS is associated with more significant hemodynamic changes, such as decreased cardiac output (CO), increased pulmonary artery pressure, and decreased blood pressure. These hemodynamic changes can lead to heart failure, cardiogenic shock, and other complications. 3
Hemodynamic parameters, such as left ventricular end-diastolic pressure (LVEDP) or systolic blood pressure/left ventricular end-diastolic pressure (SBP/LVEDP ratio), could potentially provide useful information in deciding when to use mechanical support in STEMI. Furthermore, hemodynamic evaluation, including right heart catheterization, has been shown to provide important prognostic information in patients with cardiogenic shock.
In the event of acute STEMI, the evidence of myocardial ischemic injury with abnormal cardiac biomarkers is required. High-sensitivity cardiac troponin T and creatine kinase-myocardial band have emerged as the biomarker of choice for assessing myocardial damage. 4 The peak value of high-sensitivity cardiac troponin T (Hs-cTnT) (above the 99th percentile upper reference limit) and creatine kinase-myocardial band (CK-MB) has proven to be a reliable indication of IS and is commonly utilized in clinical practice.5, 6 Previous research suggests that even early measures of such biomarkers can be relevant in terms of IS prediction.7, 8 There were some difficulties in incorporating biomarkers for STEMI risk stratification; variations in CK-MB and trop-I levels due to age, gender, renal function, and baseline health status may result in inconsistent predictive value across different patient populations. By combining biomarker trends with clinical parameters, we propose a study that evolves with the patient’s condition, offering real-time risk assessment rather than a static evaluation.
ST-elevation myocardial infarction is a severe manifestation of coronary artery involvement that is linked to a poor prognosis, including short- and long-term myocardial rupture, acute pump failure, fatal arrhythmias, and LV dysfunction. 9 Certain clinical factors, including electrocardiographic criteria, age, female gender, multivessel coronary artery disease, post-procedural flow grade, chronic kidney disease, anemia, recurrent ischemia, reduced left ventricular ejection fraction (LVEF), and elevated Killip classification, are associated with major adverse cardiovascular events (MACE) in patients with STEMI.9, 10 The main aim of the present study was to study the relationship between IS and invasive hemodynamics in patients with STEMI and its prognostic implications.
Materials and Methods
In this prospective observational study, we enrolled 136 patients presenting with STEMI and undergoing primary percutaneous coronary intervention (PPCI) between November 2019 and January 2023 at a tertiary cardiac care hospital. All STEMI patients underwent screening in accordance with the American Heart Association/American College of Cardiology guidelines. 11 Patients with a pre-existing left bundle branch block were evaluated using Sgarbossa’s criteria. 12
Patients with structural heart disease and terminal disease were excluded from the study. Written informed consent was taken from all the patients or their relatives. The study protocol was reviewed and approved by the Institutional Ethics Committee.
Echocardiography and Role of Wall Motion Score Index
The importance of IS in determining prognosis after STEMI is well established, as it correlates strongly with outcomes, including LV remodeling and survival. Among the tools available for assessing IS, echocardiography stands out as a non-invasive, widely accessible, and cost-effective modality. One of its key parameters, the wall motion score index (WMSI), provides valuable insights into regional and global myocardial function by evaluating wall motion abnormalities. Wall motion score index is calculated by assigning scores to myocardial segments based on their motion and thickening, with higher scores indicating greater dysfunction and larger IS. Although useful in a clinical setting, WMSI is frequently underused in STEMI risk assessment models.
Cardiac Catheterization
Both diagnostic and therapeutic cardiac catheterization were performed. Percutaneous access to radial or femoral arteries through the Seldinger or modified Seldinger technique was taken. Invasive hemodynamic parameters, including SBP, diastolic blood pressure (DBP), pulmonary pressure (PP), LVEDP, CO, and mean arterial pressure (MAP), were measured at the initial phase of the PPCI procedure.
Cardiac Output
The indirect Fick concept and thermodilution are typically used to calculate CO following right heart catheterization. Assumed maximal oxygen consumption is used in the indirect Fick method.

Cardiac Power Output
Cardiac power output measures the heart’s pumping capability and overall functionality. Normal cardiac power output (CPO) range: 0.6-1.0 W. CPO < 0.4 W indicates severe cardiac dysfunction, often seen in cardiogenic shock. CPO > 1.0 W: represents preserved or high cardiac performance.

Systemic Vascular Resistance
Systemic vascular resistance indicates afterload and vascular tone. Normal range: 800-1,200 dyn·s/cm5. Elevated SVR indicates cardiogenic shock, and a decreased SVR suggests vasodilation.

Heart rate was also recorded before the procedure. The normal mean arterial pressure (MAP) ranges from 70 to 100 mm Hg, while the normal LVEDP ranges from 4 to 12 mm Hg. Cardiogenic shock is characterized by a low cardiac index (lesser than 2.2 L/min/m2) with elevated LVEDP (greater than 18 mm Hg).
All STEMI patients’ demographic details, history of chest pain, breathlessness, syncope, and palpitation were recorded. General physical examination, cardiovascular and systemic examination, and laboratory investigations were recorded. Cardiac biomarkers like high sensitive troponin-I on admission, peak troponin-I, and CK-MB were also recorded. Electrocardiogram, echocardiography, and angiographic results were systematically recorded.
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) 26.0 software package (IBM SPSS Statistics for Windows, Version 26.0, Armonk, NY: IBM Corp). Continuous data were presented as mean ± standard deviation (SD), whereas categorical data were summarized as percentages. Group comparisons for continuous variables were performed using the Mann–Whitney U test. Correlation between continuous variables and LVEF, WMSI, peak trop-I, and peak CK-MB was tested using the Spearman correlation coefficient test. The linear regression analysis was performed to explore relationships between variables of interest. For all analyses, a P value less than .05 (two-tailed) was considered indicative of statistical significance.
Results
In this prospective observational study, 136 patients were included. The mean age of the study population was 55.91 years, with 83.8% males and 16.2% females. Patients with anterior wall myocardial infarction (AWMI) are more common (67.6%) than those without (32.4%).
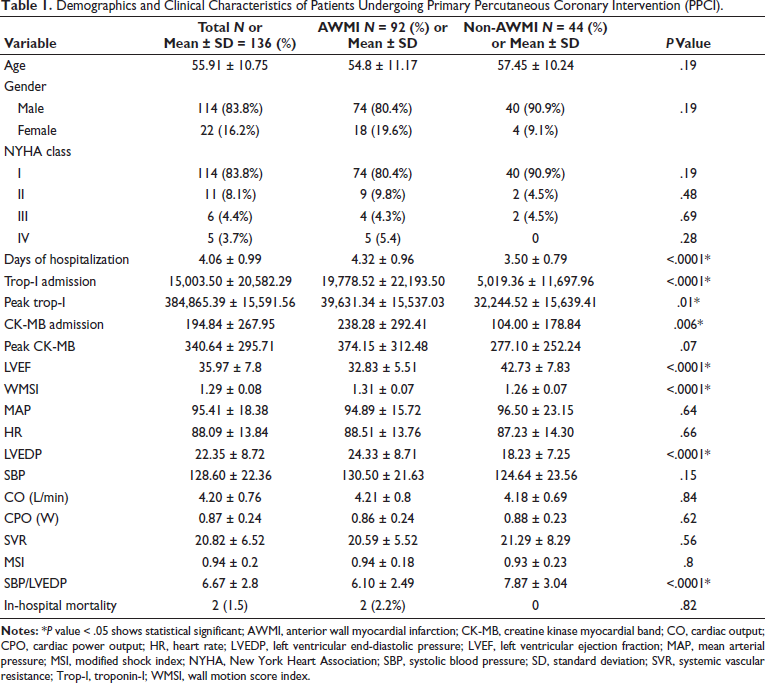
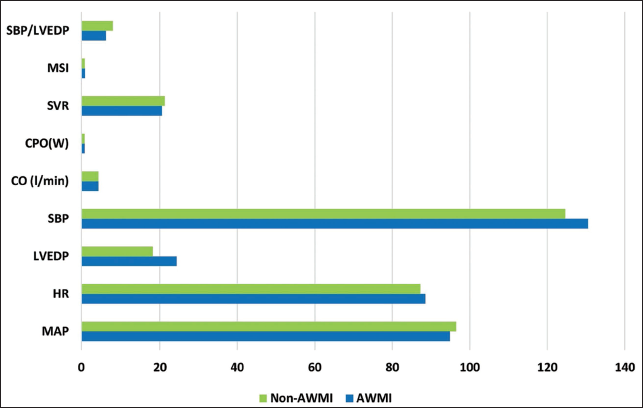
Patients undergoing PPCI were categorized based on the type of STEMI, and demographic and clinical characteristics are shown in Table 1. Most of the admitted patients had New York Heart Association (NYHA) class I (83.8%), followed by class II (8.1%) and class III (4.4%). Only five patients with AWMI had NYHA class IV. Patients with AWMI had higher values of WMSI (1.31 ± 0.07 vs. 1.26 ± 0.07; P < .0001), LVEDP (24.33 ± 8.71 vs. 18.23 ± 7.25; P < .0001), baseline trop-I (19,778.52 ± 22,193.50 vs. 5,019.36 ± 11,697.96; P < .0001), and days of hospitalization (4.32 ± 0.96 vs. 3.50 ± 0.79; P < .0001) compared to non-AWMI. Anterior wall myocardial infarction patients had lower LVEF (32.83 ± 5.29 and 42.73 ± 7.83; P < .0001) and lower SBP/LVEDP ratio (6.10 ± 2.49 vs. 7.87 ± 3.04; P < .0001) compared to non-AWMI patients, the difference was statistically significant. Hemodynamic changes in both groups were mentioned in Figure 1. Patients with AWMI showed higher values of hemodynamic measures such as SBP (130.50 ± 21.63 vs. 124.64 ± 23.56; P < 0.15) and CO (4.21 ± 0.8 vs. 4.18 ± 0.69; P < 0.64) and lower values of MAP (94.89 ± 15.72 vs. 96.50 ± 23.15; P < .64) and CPO (0.86 ± 0.24 vs. 0.88 ± 0.23; P < 0.62), although the difference was not statistically significant.
Demographics and Clinical Characteristics of Patients Undergoing Primary Percutaneous Coronary Intervention (PPCI).
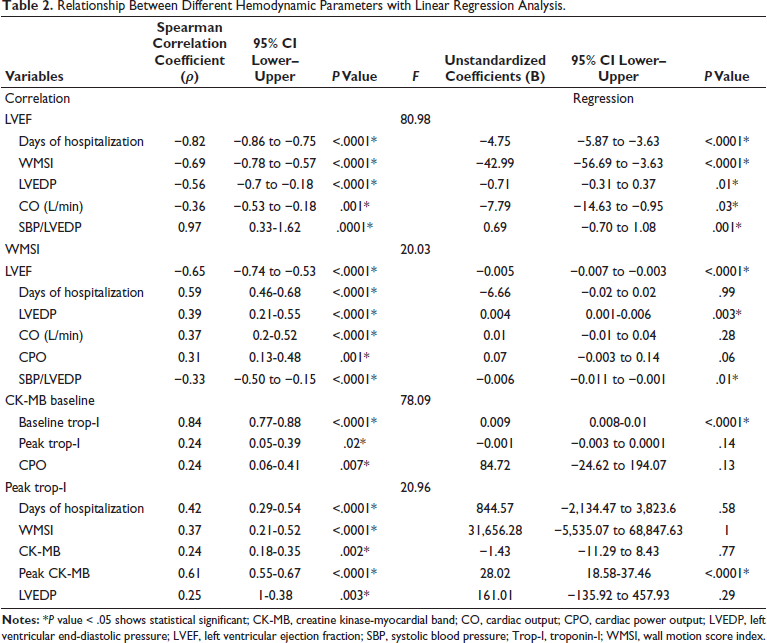
Relationship Between Different Hemodynamic Parameters with Linear Regression Analysis.
Hemodynamic Variation in Anterior Wall Myocardial Infarction (AWMI) and Non-AWMI Patients.
We did the correlation and regression analysis model to find out the association between study variables. The Spearman correlation coefficient for hemodynamic parameters with LVEF was strongly correlated with SBP/LVEDP ratio (ρ = 0.97) and WMSI (ρ = −0.69), LVEDP (ρ = −0.56), and days of hospitalization (ρ = −0.82) were inversely correlated with LVEF. Cardiac output (ρ = −0.36), SVR (ρ = 0.25), and peak trop-I (ρ = −0.39) were also inversely, moderate to weakly, correlated with LVEF. According to the linear regression model, LVEF was inversely associated with CO −7.79 (95% CI, −14.63 to −0.95; P < 0.03), WMSI −42.99 (95% CI, −56.69 to −3.63; P < .0001) and days of hospitalization −4.75 (95% CI, −5.87 to −3.63; P < 0.0001). Left ventricular ejection fraction was also associated with SBP/LVEDP ratio 0.69 (95% CI, −0.70 to 1.08; P < 0.001) mentioned in Table 2. Left ventricular ejection fraction was lower in patients with longer hospitalization. Patients with lower LVEF were found to have higher LVEDP and lower CO, SVR, and SBP/LVEDP ratio.
Hemodynamic parameter: Wall motion score index was significantly inversely associated with LVEF (ρ = −0.65) and SBP/LVEDP ratio (ρ = −0.33). Days of hospitalization (ρ = 0.59), LVEDP (ρ = 0.39), and CPO (ρ = 0.31) were also significantly associated with WMSI. According to the regression model, LVEF −0.005 (95% CI, −0.007 to −0.003; P < .0001) and SBP/LVEDP ratio −0.006 (95% CI, −0.011 to 0.001; P < .01) were inversely, and LVEDP 0.004 (95% CI, 0.001-0.006; P < .003) was positively associated with WMSI.
Cardiac biomarker baseline CK-MB was strongly associated with baseline trop-I (r = 0.84), and weakly associated with peak trop-I (ρ = 0.24) and CPO (r = 0.24). Peak trop-I was significantly associated with days of hospitalization (ρ = 0.42), peak CK-MB (ρ = 0.61), WMSI (ρ = 0.37), and LVEDP (ρ = 0.25). Regression model showed peak CK-MB 28.02 (95% CI, 18.58-37.46; P < .0001) was associated with peak trop-I. Baseline and peak cardiac biomarkers were not associated with other hemodynamic parameters. In-hospital mortality was seen in 1.5% of patients.
Discussion
The echocardiographic and cardiac biomarkers associations between IS and invasive hemodynamics in patients with STEMI were as follows. Left ventricular end-diastolic pressure, systolic blood pressure/left ventricular end-diastolic pressure ratio, and wall motion score index were the hemodynamic parameters at the time of PCI that had the strongest relationship with IS. If initiating rapid hemodynamic assistance improves outcomes in patients with large infarctions, the ability to quickly and effectively identify patients with massive infarctions, and the ability to promptly and effectively identify patients at the time of PPCI who are likely to sustain shock or death due to pump failure following STEMI, may be crucial. 13 Many studies have demonstrated a link between SBP and mortality, and low SBP accompanied or unaccompanied by evidence of hypoperfusion is now used to diagnose cardiogenic shock.3, 14
However, parameters other than CO influence blood pressure regulation, and it is unclear if SBP is the most effective hemodynamic indicator for identifying individuals with a high risk of LV failure during PPCI. Systolic blood pressure is influenced by CO, but a preserved or elevated SBP may occur with significant compensatory vasoconstriction (increased SVR), which masks reduced stroke volume (SV) or CO. During PPCI, myocardial ischemia, reperfusion, and pharmacologic interventions alter heart rate (HR), SV, and SVR dynamically, leading to variations in SBP that may not consistently predict left ventricular failure (LVF) risk.
Cardiogenic shock is characterized by increased sympathetic activity and the stimulation of compensatory mechanisms, which increase HR, LV contractility, fluid retention, and vasoconstriction, all of which can raise SBP. There is emerging evidence that hemodynamic measurements carried out during PPCI, such as LVEDP, pulse pressure (PP), and SBP/LVEDP ratio, are more predictive of outcomes in STEMI patients than SBP and might be more closely related with the extent of the LV damage caused by a MI.15–19
In our study, we showed the correlation between the location of infarction and invasive hemodynamic variables. Recognizing the role of hemodynamic stability in limiting IS emphasizes the importance of pre-procedural stabilization. Patients having AWMI (67.6%) were more than patients having non-AWMI (32.4%). There was a statistically significant difference in the mean value of LVEF in the AMWI and non-AMWI groups (P < .0001). Patients with AWMI had higher peak CK-MB and trop-I compared to patients with non-AWMI, but the difference was not statistically significant (P < 0.07, 0.17).
Patients with AWMI had higher WMSI (1.31 ± 0.07), LVEDP (24.44 ± 8.81 mm Hg), baseline trop-I (19,778.52 ± 22,193.50 ng/L), days of hospitalization (4.32 ± 0.96), and SBP/LVEDP ratio (6.10 ± 2.49) compared to patients with non-AWMI. There was a significant difference between the two groups (P < .0001). Patients with AWMI had a trend toward lower MAP and SBP compared to patients with non-AWMI, but they were also found to be statistically non-significant. Patients with hemodynamic disturbances were found to develop larger infarcts, regardless of the location of the culprit lesion, suggesting these disturbances may serve as an early predictor of poor outcomes. Conversely, patients without hemodynamic disturbances tended to have smaller infarcts and better outcomes. Hong et al. studied the prognostic significance of the location of infarction and found that AWMI was associated with adverse outcomes. 3
Biochemical markers (peak troponin-I and peak CK-MB levels) as well as LVEF and WMSI, by 2D echocardiography, were used to measure the infarction’s size. There was an inverse correlation between biochemical markers (peak trop-I, peak CK-MB) and LVEF, with LVEF reducing as biochemical markers increased. Whenever PPCI occurred, the mean HR was 88.09 ± 13.8/min, LVEDP 22.35 ± 8.72, SBP 128.60 ± 22.36 mm Hg, CO 4.20 ± 0.76 L/min, and SBP/LVEDP ratio was 6.67 ± 2.8. These findings were similar to Goins et al. Peak troponin levels and echocardiographic evaluation of LV systolic function at the time of PPCI showed that the hemodynamic parameters LVEDP, PP, and SBP/LVEDP ratio had the strongest connection with the IS. 20
The study adds to speculation that invasive hemodynamic parameters are assessed during PPCI to predict outcomes in STEMI patients. During PPCI, targeted adjunctive therapies (e.g., thrombectomy, vasodilators for microvascular dysfunction) can be employed based on hemodynamic assessments. Intra-procedural monitoring of hemodynamics can inform decisions, such as escalating to advanced support or prolonging reperfusion therapy. Tiller et al. showed in their study that, on admission, increased biomarkers indicated large IS, and that routine indicators such as HR, SBP, Killip class, and post-thrombolysis in myocardial infarction (TIMI) flow imparted large IS. 7
Planer et al. reported that LVEDP was found to be an independent predictor of unfavorable outcomes. Therefore, we compare patients with LVEDP 18 mm Hg and LVEDP >18 mm Hg had higher hazard ratios (95% confidence interval) for death at 30 days and 2 years. This study also reported that in STEMI patients undergoing PPCI, angiographically identifiable collaterals had a protective effect on the size of the enzymatic infarct. 16
A comprehensive hemodynamic evaluation, including right heart catheterization, offers significant predictive insights in individuals experiences cardiogenic shock. Certain factors like LVEDP and SBP/LVEDP ratio calculated during PPCI are linked to the extent of the heart function as measured by biochemical markers and echocardiographic assessment of LV function. Goins et al. revealed a similar finding, which endorses our findings. 20 Patients with low LVEF and high peak CK-MB had a higher duration of hospitalization. This signifies that a large IS increases the stay in hospitalization.
Hemodynamic measures and cardiac biomarkers combining approach creates new research and clinical options in cardiology. It indicates the significance of the approach to STEMI management, which involves not only culprit lesion intervention but also systemic circulatory optimization. Also, in our study, there was one in-hospital mortality. This patient had high trop-I, CK-MB, WMSI, and reduced LVEF. Considering all these parameters as surrogates of IS is related to outcomes.
Limitations of the Study
The main limitations include that it is a single-center study and a lack of follow-up data. Other limitations include a single time-point measurement of hemodynamic variables. Future research with larger, more diverse cohorts, standardized methods, and interventional trials is essential to validate and expand upon these findings.
Conclusion
Patients with elevated trop-I, CK-MB, WMSI, and reduced LVEF experienced prolonged hospital stays, indicative of larger ISs. The outcomes were predicted by hemodynamic markers. This suggests the LVEDP along with the ratio of SBP/LVEDP during PPCI to evaluate LV performance and hemodynamic condition. Clinically, an increase in LVEDP may indicate elevated filling pressures and diastolic dysfunction, which can influence the use of diuretics or vasodilators. In contrast, a low SBP/LVEDP ratio suggests inadequate CO and severe myocardial dysfunction, requiring the use of inotropic drugs or mechanical support. These measurements offer immediate insights into patient stability, enabling customized interventions. Continuous monitoring is required for evaluating treatment outcomes and making real-time modifications to therapy.
Footnotes
Data Availability Statement
Due to confidentiality of patient’s identity, we cannot share patient’s data.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
The study has been approved by the Institutional Ethics Committee (UNMICRC/CARDIO/2019/13).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by U. N. Mehta Institute of Cardiology and Research Centre and received no specific grant from any funding agency, commercial, or not for profit sectors.
Patient Consent
Informed consent for publication was provided by the participant(s) or a legally authorized representative.