
Abstract
Introduction
Demographics, comorbidities, and pacemaker-related factors may affect survival in patients having permanent pacemakers. This study reports the mortality risk predictors in patients undergoing pacemaker implants.
Methods
This retrospective single-cohort observational study was conducted in permanent pacemaker implant patients from January 2015 to March 2021 in a tertiary care center in India. Survival was assessed during follow-up. Independent risk predictors for mortality were identified by multivariate Cox regression analysis. Using these, a risk score was derived to categorize patients into different risk groups.
Results
A total of 683 patients were included. 16.1% of patients died during a mean of 3 years follow-up. Independent mortality risk predictors were age >60 years at implant, diabetes mellitus, hemoglobin <11 g/dL, baseline left ventricular ejection fraction <50%, and presence of structural heart diseases. Sex, history of hypertension, atrial arrhythmias, indication for an implant, and higher serum creatinine value did not significantly affect survival. The preimplant mortality risk score showed patients with scores of 0-1 had 3.9% mortality, 2-3 had 18.6%, and scores of 4-6 had 35.4% mortality risk over 3 years of mean follow-up.
Conclusion
Poor survival in patients undergoing pacemaker implant was independently associated with older age at implant, history of diabetes mellitus, presence of anemia, baseline left ventricular systolic dysfunction, and presence of structural heart diseases. Our preimplant mortality risk score can help to categorize implant patients as low, intermediate, or high-risk groups.
Keywords
Introduction
Cardiac pacing plays a crucial role in enhancing both survival rates and quality of life for patients experiencing symptomatic bradycardia.1–4 However, overall survival rates following pacemaker implantation are lower than those expected for age- and gender-matched individuals in the general population.5–11 Numerous observational studies analyzed survival in pacemaker patients with relation to demographic factors such as age and gender, patient-related aspects like symptoms and urgency of the procedure, indication of implant, cardiac and non-cardiac comorbidities, length of hospital stay, and pacemaker-related factors like specific pacing mode, pacing percentage, and pacing location. These studies have yielded inconsistent and sometimes contradictory results; also, there is a paucity of Indian data related to survival in pacemaker patients.12–24
To address this gap, we designed this study to evaluate mortality rates in patients following permanent pacemaker implantation and to explore associations with their baseline characteristics. Finding these factors can help to identify patients at higher risk and facilitate the modification of such risk factors whenever feasible.
Methods
Study Design and Population
This retrospective single-cohort observational study was conducted in a single, tertiary care center. Institutional ethics committee approval was obtained beforehand. Patients older than 18 years who underwent pacemaker implantation between January 2015 and March 2021 were included. Patients with pulse generator change as index procedure, as well as those who received implantable cardioverter defibrillators or cardiac resynchronization therapy devices, were excluded from the study.
Data Collection
Patients who had undergone pacemaker implantation from January 2015 to March 2021 were identified from electronic clinical records. Those who satisfied the inclusion and exclusion criteria were included in the study. Electronic medical records at the time of implantation were reviewed to obtain demographic, clinical, and procedural data. Demographics like age at implant and sex were noted. Clinical history including the presence of systemic hypertension, diabetes mellitus, and history of coronary artery disease were reviewed for each patient in our records. Other baseline investigation values like serum creatinine and hemoglobin at the time of implant were noted. Each patient record was reviewed for indication of implant, presence or absence of structural heart disease, presence or absence of atrial fibrillation (AF), and left ventricular ejection fraction (LVEF) at the time of implant. Data on device mode and right ventricular lead position (apical or non-apical) in these patients were collected.
Patients who had not visited the hospital in the recent past were contacted telephonically. In cases of death, efforts were made to determine the cause by consulting close relatives, available medical records, death certificates, and autopsy reports. The causes of death were classified as either cardiac or non-cardiac and analyses were conducted separately for all-cause mortality and cardiac mortality.
Follow-up
Follow-up data was collected through outpatient department visits or telephone interviews, ensuring a minimum follow-up period of 1 year.
Endpoints
The primary endpoint of the study was all-cause mortality, while the secondary endpoint focused on cardiac mortality.
Outcome Variables
In our study, the primary outcome variable was death. The categorical independent variables were sex, diabetes mellitus, hypertension, AF, coronary artery disease, structural heart disease (such as congenital or valvular heart disease, or cardiomyopathies like hypertrophic, restrictive, or dilated), the indication for pacemaker implantation, the mode of the pacemaker, and the position of the right ventricular lead. The continuous independent variables comprised age at the time of implantation, LVEF, hemoglobin levels, and serum creatinine levels at implantation. For the analysis, we categorized the continuous variables into two groups: age (<60 years or ≥60 years), hemoglobin (<11 g% or ≥11 g%), serum creatinine (≤1 mg/dL or >1 mg/dL), and LVEF (<50% or ≥50%).
Data Analysis
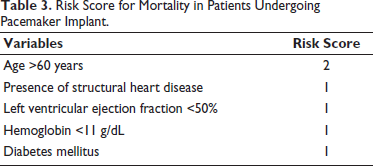
Statistical analysis was conducted using IBM SPSS (version 2019). Continuous variables were presented as mean ± standard deviation, while categorical variables were expressed as frequency and percentage. For survival analysis, the Kaplan–Meier survival curve was used, and statistical significance was assessed with the log-rank test. Significant variables were identified, and a multivariate Cox regression analysis was performed. Independent significant variables after multivariate analysis were used to calculate the mortality risk prediction score, which was calculated by summing the weighted values of each variable based on its hazard ratio (HR).25, 26 Points were assigned as follows: HR 1.1-2.0 = 1 point, HR 2.1-3.0 = 2 points, and HR 3.1-4.0 = 3 points. Individual risk score was calculated for each patient, and patients were divided into three groups: a low-risk group with scores of 0-1, an intermediate-risk group with scores of 2-3, and a high-risk group with scores of 4-6.
Results
Patients and Procedure
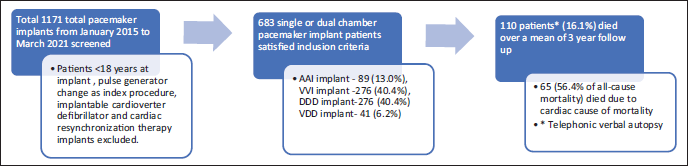
A total cohort of 683 patients who received single or dual-chamber pacemaker implants were identified from an initial pool of 1,171 procedures conducted between January 2015 and March 2021. The duration of follow-up for these patients varied from 1 to 7 years, with an average of 2.96 ± 1.85 years. Among these patients, 120 (17.5%) were implanted due to sinus node dysfunction (SND), while the remaining 563 (82.5%) had indications for atrioventricular block (AV block). In terms of the types of implants, 89 patients (13.0%) received single chamber atrial pacing (AAI) devices, 276 patients (40.4%) were fitted with single chamber ventricular pacing (VVI) implants, another 276 patients (40.4%) had dual chamber pacing mode (DDD) devices, and 41 patients (6.2%) received VDD implants (Figure 1).
Flowchart Indicating Methods and Follow-up of Pacemaker Patients.
Baseline Characteristics
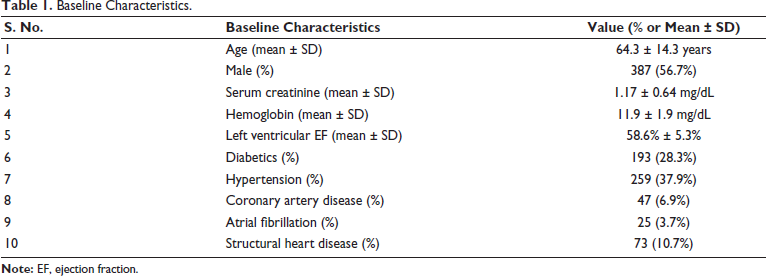
The study cohort had a slight male preponderance (56.7%), and the mean age at the implant was 64.3 ± 14.3 years. 28.3% of patients were diabetics, and 37.9% had a history of hypertension at the time of implant. A total of 25 (3.7%) patients had a history of AF, and 73 (10.7%) patients had structural heart disease (Table 1).
Baseline Characteristics.
Clinical Outcome and Survival Analysis
Out of 683 patients, 110 (16.1%) died over a mean 3-year follow-up.
Univariate Analysis
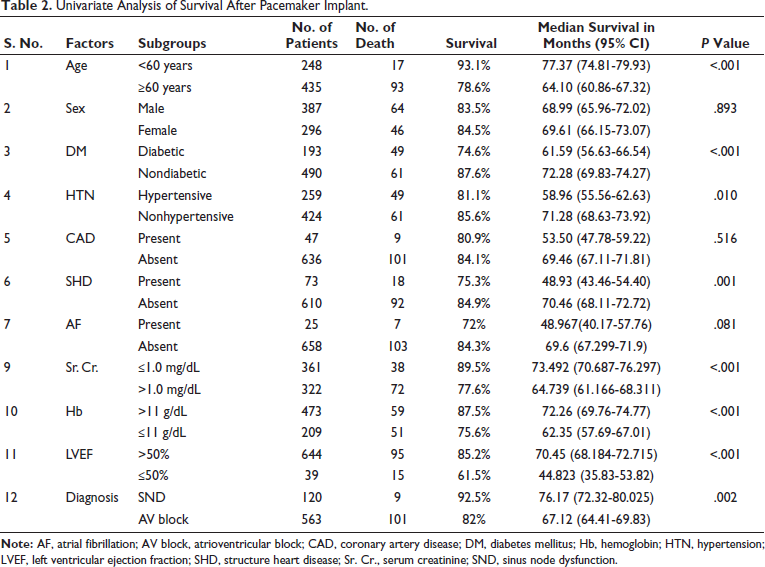
The survival curve was plotted for each variable using the Kaplan–Meier method, and statistical significance was determined by log-rank test. Univariate survival analysis showed that individuals over the age of 60 years, those with a history of diabetes mellitus, systemic hypertension, serum creatinine levels above 1 mg/dL, hemoglobin levels below 11 mg/dL, LVEF below 50% at the time of implant, those with structural heart disease and the presence of AV block as an indication for implantation were associated with notably lower survival rates (P value < .05). Conversely, factors such as the individual’s sex, the presence of coronary artery disease, and atrial flutter or fibrillation did not show a significant impact on survival (P value > .05) (Table 2).
Univariate Analysis of Survival After Pacemaker Implant.
Multivariate Analysis
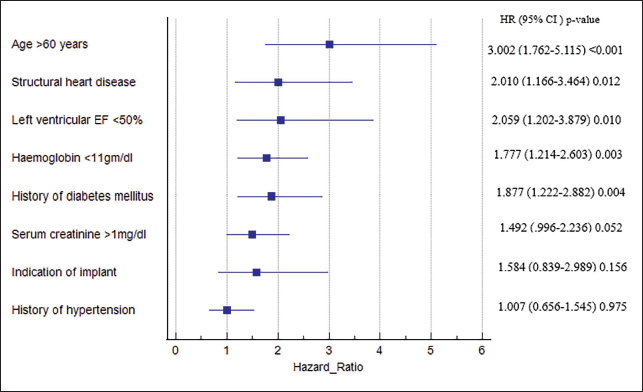
Outcome variables that were significant in univariate analysis were included in multivariate analysis. Cox regression hazard analysis was used to assess the effect of different variables on survival. The results indicated that factors such as being over 60 years old, having diabetes mellitus, a hemoglobin level below 11 g/dL, the presence of left ventricular dysfunction, and structural heart disease were independently linked to poorer survival outcomes. We found that indication for implant, history of hypertension, or serum creatinine >1 mg/dL did not affect medium-term survival in pacemaker patients (Figure 2).
Forest Plot for Multivariate Analysis.
Mortality Risk Prediction
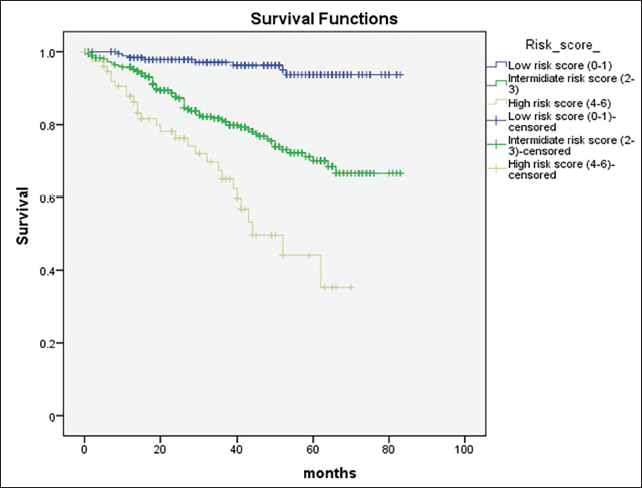
The individual risk score was calculated, which showed patients in the low-risk score group (scores of 0-1) had a mean survival of 79.91 months, those in the intermediate-risk score group (scores of 2-3) had 66.54 months, and those in the high-risk score group (scores of 4-6) had 45.83 months. During the follow-up of 2.96 years, patients in the low-risk group had 3.9% mortality, the intermediate-risk group had 18.6% mortality, and the high-risk group had 35.4% mortality (Figure 3 and Tables 3 and 4).
Kaplan–Meier Analysis of Survival in Different Risk Groups (P Value < .01).
Risk Score for Mortality in Patients Undergoing Pacemaker Implant.
Three Categories According to Cumulative Risk Score.

Secondary Outcome
During the follow-up period, of the 110 patients who passed away, 62 (56.4%) succumbed to cardiac-related issues. Our secondary outcomes especially look for cardiac mortality-related risk factors. The multivariate cox-regression analysis showed that age above 60 years, history of diabetes, patients having structural heart disease, AF, and LVEF <50% were independently associated with poor survival in pacemaker patients who died due to cardiac cause after implant (P < .05).
Discussion
In this single-center cohort study involving 683 patients who received pacemaker implants, the survival rate was 83.9% after an average follow-up of 3 years. Key predictors of mortality included being over 60 years old at the time of implantation, having diabetes mellitus, baseline left ventricular systolic dysfunction, hemoglobin levels below 11 g/dL at the time of the procedure, and the presence of structural heart disease. A scoring system was created using these factors to assess mortality risk in patients undergoing pacemaker implantation.
In our study, the average age at which patients received implantation was 64.3 years, with a 3-year survival rate of 83.9%. For instance, a large European study by Brunner et al. on 6,505 pacemaker patients, with a mean age of 72.1 years at implantation, reported a 5-year survival rate of 65.5%. 17 Similarly, another European study by Pyatt et al. in 833 pacemaker patients with a mean implantation age of 77.3 years had a survival rate of only 55%. 14 Comparing our results with global data indicated that Indian patients are nearly a decade younger than those in Western populations at the time of implant, which might explain better survival in these patients.27–29
We found that patients older than 60 years at implant had significantly lower survival rates (78.6% vs. 93.1%; P < .001). Similarly, Dębski et al. highlighted that each additional year of age at implantation increased mortality risk by 7% (P < .001), while being male was linked to a 30% higher mortality risk compared to females (P < .001). 18 Pyatt et al. reinforced these findings, identifying older age (RR 1.06; 95% CI 1.01-1.12) and male sex (RR 1.27; 95% CI 1.22-1.32) as significant mortality risk factors in pacemaker patients. 14
In our study, age was the strongest key predictor of prognosis in pacemaker patients (HR 3.00; 95% CI 1.76-5.11; P < .001); however, sex did not significantly influence survival (females: 84.5% vs. males: 83.5%; P = .893) after multivariate analysis. In studies of pacemakers in India, female patients have shown similar survival rates compared to males, potentially due to factors like the types of pacemakers used, the underlying heart condition, and the overall health of the patient.8, 27, 29 In the general population, in India, women typically have a life expectancy of 2.5 years longer than men, while globally, women’s life expectancy is around 5 years longer than men’s; these facts might confound our study results. 30
Patients with atrioventricular (AV) block exhibited lower survival rates than those with SND (82.4% vs. 91%; P = .002), though this difference was not significant after multivariate analysis (HR 1.58; P = .156) in our study. Similar trends have been observed in previous studies as Brunner et al. reported higher 5-year survival rates for patients with sick sinus syndrome than those with AV block (73.5% vs. 62.6%; P < .05), 17 likewise, Pyatt et al. found that AV block was associated with poorer survival outcomes compared to sinus node disease (P < .05). 14 The better survival seen in patients with SND could be influenced by factors such as younger age at implant and AAI pacing mode.27–29
Chronic comorbidities like diabetes mellitus and hypertension, which are prevalent with advancing age, may impact survival in pacemaker patients. Our study revealed that diabetic pacemaker patients had significantly lower survival rates (74.6% vs. 87.6%; HR 1.88; CI 1.22-2.88; P = .004), while hypertensives did not show a statistically significant difference (81.1% vs. 85.6%; HR 1.007; CI 0.656-1.545; P = .975).
Similarly, a study by Krystyna et al. reported that higher fasting glucose levels were linked to poorer survival (HR = 1.19; P < .01), while hypertension appeared to have a protective effect in older pacemaker patients (HR = 0.52; P < .05). 20 Our data analysis emphasizes awareness of higher mortality risk and control of blood sugar levels in the diabetic pacemaker population.
Our study found that patients with hemoglobin levels below 11 g/dL at the time of implantation had lower survival rates (75.6% vs. 87.5%; HR 1.77, P = .003). Additionally, those with serum creatinine levels above 1 mg/dL also had significantly lower survival (77.6% vs. 89.5%), though this difference was marginally statistically insignificant after multivariate analysis (HR 1.492; P = .052). Supporting this, Balla et al. found that an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m² or creatinine above 1.3 mg/dL was linked to poorer survival (HR = 1.63; P = .006) in octogenarians, while higher hemoglobin levels correlated with better survival (HR = 0.89; P = .008). 22 Similarly, Krystyna et al. also found that higher hemoglobin levels were associated with improved survival (HR = 0.846; P < .05) in older patients. 20
Higher serum creatinine, lower hemoglobin levels, and associated hypertension may indicate underlying chronic renal dysfunction, which is more or less associated with higher mortality in pacemaker patients and is one of the important aspects to emphasize regular follow-up and needful treatment.
Patients with left ventricular systolic dysfunction (LVEF <50%) demonstrated poorer survival rates (61.5% vs. 85.2%), making it a strong independent risk factor for mortality (HR = 2.059; p = 0.01). Similarly, those with structural heart disease including congenital, valvular, and various types of cardiomyopathies also exhibited significantly lower survival (75.3% vs. 84.9%; HR = 2.01; P = .012). While Krystyna et al. found that left ventricular systolic dysfunction (LVEF 40% cut-off) did not have a prognostic value (P > .05) in pacemaker patients, 20 Pyatt et al. identified valvular heart disease (RR 2.01; 95% CI 1.98 to 2.04) as an independent predictor of mortality. 14
Our study emphasizes the importance of a pre-procedural echocardiogram for structural abnormalities in every indexed pacemaker patient, which might affect prognosis after implant.
We observed that patients with AF had lower survival rates after 3 years of follow-up (72% vs. 84.3%), although this difference was not statistically significant (P = .081). Similarly, Brunner et al. 17 reported that pacemaker patients with a history of AF had lower 5-year survival rates (58.6% vs. 65.5%, P < .0001), a finding echoed by Bradshaw et al. 16 However, Dębski et al. found no significant impact of atrial flutter or fibrillation on survival (P = .548). 18 While many studies suggest that AF is linked to lower survival rates in pacemaker patients, this may be influenced by the pacing mode-VVI pacing, which is commonly used in these patients, has been associated with poorer outcomes.14, 17
Our study found that coronary artery disease did not significantly impact survival in pacemaker patients (P > .05). This aligns with findings from Cheng et al., who also reported no significant effect of coronary artery disease on survival (P = .43). 19 Our findings stress that routine coronary angiograms before implant might be avoided as there is no survival benefit and unnecessarily might pose a risk for dye-induced renal dysfunction.
Our mortality risk prediction score, developed using pre-implant clinical variables, provides a reliable way to assess prognosis after pacemaker implantation in the medium term. However, it still needs validation in an external cohort. Notably, previous studies have not established a comprehensive mortality risk score for pacemaker patients across all age groups.
Limitation
This observational study has a mean follow-up duration of 3 years. Longer follow-up could better indicate prognostic factors. Additionally, we lack data on some variables that could impact survival, such as body mass index (BMI), eGFR, and detailed medication history. Furthermore, the information regarding the causes of mortality was gathered using a verbal autopsy questionnaire, which may not accurately reflect the true causes of death.
Our research focuses exclusively on survival rates and does not address the quality of life of patients following their implants. Lastly, the findings and the effectiveness of the scoring system require validation through a prospective large-scale study.
Conclusion
This retrospective single-cohort study reports survival in a contemporary cohort of 683 patients undergoing pacemaker implants in a tertiary care center in India. After an average follow-up of 3 years, 83.9% of the patients were alive. Poor survival was independently associated with age over 60 years, diabetes mellitus, a hemoglobin level below 11 mg/dL, the presence of structural heart disease, and left ventricular systolic dysfunction. A risk score was constructed using these factors to categorize patients into different risk groups, which could assist in identifying patients at greater risk of mortality during medium-term follow-up following a pacemaker implant.
Footnotes
Abbreviations
AAI, single chamber atrial pacing; AF, atrial fibrillation; AV block, atrioventricular block; CRT, chronic resynchronization therapy; DDD, dual chamber pacing mode; ICD, implantable cardiac defibrillator; SND, sinus node dysfunction; VVI, single chamber ventricular pacing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional ethics committee approval was taken as per protocol.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Participant consent was taken either in person who attended clinics or telephonically for those who were not able to attend, or in case of death, close relative consent was taken.