
Abstract
Despite advanced drug therapy, percutaneous intervention, and surgery, atherosclerotic cardiovascular disease remains a major cause of morbidity and mortality worldwide. Atherosclerosis has a long subclinical stage before it manifests clinically, which can be detected early, leading to more appropriate use of primary prevention measures. Several noninvasive methods to detect subclinical atherosclerosis have been explored to predict future cardiovascular events. Carotid imaging and coronary artery calcium score have shown their ability to predict beyond conventional risk factor-based assessment. Other common methods are femoral plaque assessment, the diameter of the aorta, calcification of the descending aorta, ankle–brachial index, and endothelial function test. Current guidelines recommend coronary calcium score for better risk stratification of the intermediate-risk group and statin therapy with a higher score. The clinical utility of other methods needs to be explored further. Lifestyle change and statin therapy may be reinforced to improve outcomes with the detection of atherosclerosis during the subclinical stage.
Introduction
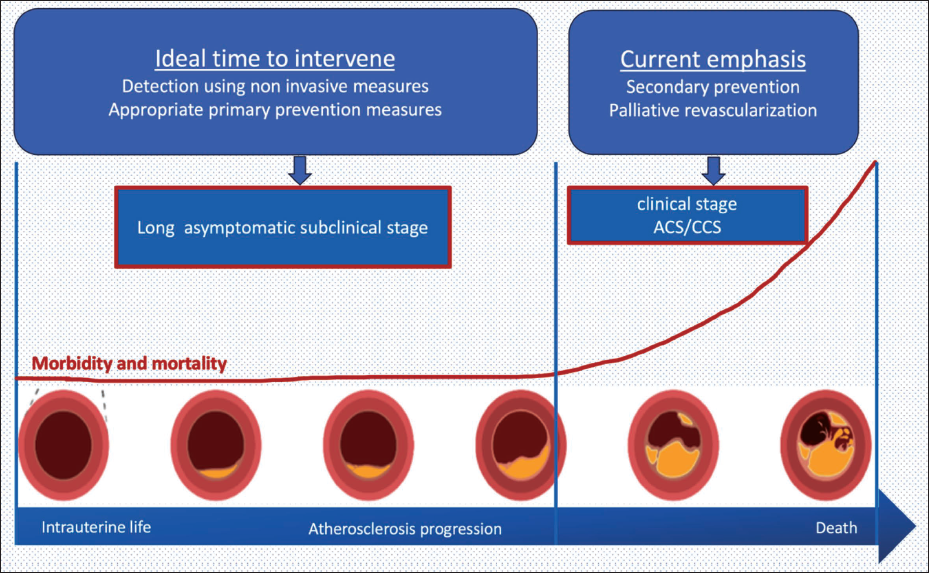
Atherosclerotic cardiovascular diseases (ASCVDs), mainly coronary artery disease (CAD) and stroke, are the leading cause of morbidity and mortality worldwide. 1 Subclinical atherosclerosis can be defined as atherosclerosis involving any arterial territory without clinical manifestation or cardiovascular (CV) event. Clinical manifestations of atherosclerosis include CAD, cerebrovascular event, limb ischemia, aortic aneurysm, and sudden cardiac death. Even with the advancement of drug therapy and intervention, CV events are responsible for the majority of morbidity and mortality globally. With a growing understanding of atherosclerosis, it is now obvious that it has a prolonged incubation period before it manifests clinically. Almost half of the events happen in individuals with no apparent prior symptoms and are classified as low risk according to the Framingham score. 2 Similarly, the majority of acute coronary events happen with plaque disruption of nonobstructive coronary stenosis. 3 Atherosclerosis process may be initiated during the intrauterine stage and continuous throughout life till death (Figures 1). Its management should also be a continuous effort from womb to death involving diet, exercise, management of comorbidity, and drug therapy. Current revascularization methods mainly focus on relieving significant coronary obstruction, locally and focally, which may not be sufficient to prevent subsequent acute coronary syndrome. Therefore, emphasis should shift towards early detection of subclinical atherosclerosis and appropriate primary prevention measures to reverse/halt the progression of atherosclerosis to prevent subsequent fatal CV events.
Schematic Diagram Depicting Atherosclerosis as a Continuous Process from Intrauterine Period till Death with Long Subclinical Stage, Which Should Be the Ideal Time for Intervention.
Pathological Basis
Virtually histological changes of clinically manifested and subclinical atherosclerosis are similar. Pathologically atherosclerosis progresses from intimal hyperplasia to fibroatheroma, thin-capped fibroatheroma (TCFA) and plaque rupture or erosion with thrombosis. Based on underlying histopathology, subclinical atherosclerosis can be classified into three groups.
4
Stable unruptured plaque with less than 50% luminal stenosis Stable and unruptured plaque with 50%-90% stenosis or chronic total occlusion (CTO) without clinical symptom Plaque rupture or erosion leading to thrombosis with less than 50% stenosis without producing ischemic symptoms
Pathological intimal thickening (PIT) is considered as an initial stage of atherosclerosis consisting of focal intimal hyperplasia with microscopic calcification and without lipid pool. It progresses to fibroatheroma with the development of lipid pool, macrophage infiltration, and microcalcification. Inflammation and proteolytic enzymes produced from macrophages lead to necrotic core in more advanced atheroma. Subsequently, the fibrous cap of atheroma becomes thin (<65 microns) secondary to macrophage infiltration, apoptosis of smooth muscle, and lack of new collagen synthesis. This TCFA is considered a high-risk/vulnerable plaque for future acute coronary events.
Progression of atherosclerosis usually leads to critical luminal stenosis producing ischemic symptoms. However, positive remodeling of the artery with outward expansion without compromising the lumen is an established explanation for high atherosclerosis burden without ischemic symptoms. 5 The limit of this positive remodeling is usually <40% luminal narrowing, beyond which there is a rapid loss of lumen. Silent plaque rupture with thrombosis may be healed without any clinical manifestation. Such healed lesions are common in autopsy studies. 6 These healed ruptures lead to fibrocalcific plaques or sometimes CTO. Clinical studies involving CT coronary calcification correlate well with future CV events. 7
Although coronary atherosclerosis is the most often sought-after lesion, this is even more common in other vascular beds. According to imaging-based PESA (progression of early subclinical atherosclerosis) study, 8 atherosclerosis is more common in iliac arteries (44%), followed by carotids (31%), aorta (25%) and coronaries (18%). Autopsy studies from Japan also revealed aortofemoral bed being the most common site for atherosclerosis. 9 There are a few differences in atherosclerosis involving various beds. The aorta is the most common site of atherosclerosis and is mostly asymptomatic. Atheroembolism from the aorta to other organs manifests as stroke, acute kidney injury, limb, or mesenteric ischemia. Plaques with a thickness of more than 4 mm are usually associated with an increased risk of embolization. 4 There are some specific characteristics of atherosclerosis involving lower limb arteries. Plaques are mostly fibrocalcific with calcium content much higher than the carotid or coronary artery. The presence of Monckeberg-type medial calcification is a histological hallmark, which is very rare in carotid or coronaries. The lipid core usually has very little with a thick fibrous cap and more chance of chronic total occlusion. All these unique features suggest a higher frequency of subclinical atherosclerosis involving lower limb arteries. Characteristics of carotid atherosclerosis are usually similar to coronary involvement. Carotid calcification increases with severe luminal stenosis. Acute thrombosis at the plaque rupture site is less common contrary to coronaries. Coronary atherosclerosis often coexists with other vascular bed involvement. This makes the basis of screening of carotid atherosclerosis to predict coronary events.
Noninvasive Assessment of Subclinical Atherosclerosis
Invasive coronary angiogram and intravascular imaging remain the gold standard for the assessment of the burden of atherosclerosis. However, use of these invasive modalities may not be feasible for screening and primary prevention at the subclinical stage. Various noninvasive methods were explored to assess the underlying atherosclerosis burden and predict future CV events. Assessment of inflammatory markers, such as high-sensitivity C-reactive protein (hs-CRP), has been shown to predict future CV events and also shown to decline with statin therapy. These methods can be used for better risk stratification and primary prevention of CV events beyond conventional risk factor-based assessment. Table 1 summarizes the current methods of detecting subclinical atherosclerosis with their interobserver variability and predicting ability for future CV events.
Noninvasive Methods to Assess Subclinical Atherosclerosis.

Carotid Artery Imaging for Atherosclerosis
Superficial location and relative immobility of the carotid artery allow noninvasive assessment with ultrasound to detect atherosclerosis. This might act as a surrogate marker of atherosclerosis in other vascular beds.
CIMT (carotid intima media thickness) is a quantitative parameter to express intimal thickening secondary to atherosclerosis. CIMT is usually measured with a B-mode ultrasound probe over the common carotid artery. Several studies showed a positive correlation between CIMT and severity of coronary atherosclerosis in invasive angiography.10, 11 Similarly increased CIMT has been shown to predict future CAD and stroke, but recent metanalysis questioned its role beyond traditional risk factor-based assessment.12, 13 There may be compensatory intimal hyperplasia secondary to increased blood pressure, hemodynamic stress, and growth and may not represent true atherosclerosis. 14 Various limitations are proposed against the appropriateness of CIMT measurement. CIMT is routinely measured in the common carotid artery due to its superficial easily accessible location; however, early atherosclerosis usually starts at bulb/bifurcation. In addition, B-mode ultrasound measurements of CIMT are usually based on the assessment of opposite walls of the carotid artery perpendicular to the probe and not assessing the entire circumference of the wall. Plaque formation in the carotid bifurcation usually begins along the outer wall of the bulb because of predisposing hemodynamic factors and then progresses to involve the circumference of the bulb. This may not be imaged with routine CIMT of common carotids. Finally, CIMT is a relatively simplistic measure of the carotid wall and does not take into account the complexity of plaque features such as lipid-rich necrotic core, intraplaque hemorrhage, and thin fibrous cap, which are closely related to plaque vulnerability and CV risk. 15
More detailed carotid imaging to detect carotid plaque is a better predictor of future CV events. Meta-analysis comparing CIMT and carotid plaque found that the presence of carotid plaque had a significantly higher diagnostic accuracy for the prediction of future myocardial infarction compared to CIMT. 16 Ultrasound-based studies assessing carotid used various definitions for carotid plaque, such as protrusion inside lumen causing diametric stenosis, protrusion into the artery lumen of at least 0.5 mm or 50% of the surrounding intima-media thickness, intimal thickening of at least 1 mm, or >1.21 mm or 1.5 mm, or focal widening of the artery compared with adjacent sites and there is positive correlation between future CV events.17, 18 Pooled meta-analysis showed presence of carotid plaque associated with increased risk of stroke (hazard ratio [HR]: 1.89, 95% confidence interval [CI]: 1.04-3.44) and coronary events (HR: 1.77; 95% CI: 1.1-2.6). 19 Similarly, plaque area, calcification, heterogeneous plaque, and increased plaque score are associated with more CV events. A similar positive association was also shown in the MESA (multiethnic study of atherosclerosis) study including all ethnicities. 20 Although carotid imaging is mostly studied with B-mode ultrasound, there is expanding evidence with the use of computed tomography/magnetic resonance imaging (CT/MRI) for more accurate assessment and better prediction. 19 However, cost and radiation exposure prohibit its use in routine clinical practice. Imaging of the carotid artery using ultrasound for a comprehensive assessment of common, external, and internal carotid along the whole length with circumferential assessment should be done.
Coronary Artery Calcium
An increase in calcification of plaques suggests a high atherosclerosis burden. Noncontrast-gated cardiac CT scan can be used to assess this calcification noninvasively and serve as evidence of subclinical atherosclerosis. Calcium scoring (Agatston score) was calculated with summation of all calcified areas multiplied by respective density (1-4 based on peak attenuation, 1 for 130-199 Hounsfield unit [HU], 2 for 200 HU -299 HU, 3 for 300 HU -399 HU, 4 for ≥400 HU). Other methods for calcium scoring, such as the volumetric method, have been developed. This was shown to be more reproducible than the Agatston score. However, the majority of the clinical studies validated Agatston scoring, leading to its more frequent clinical use. A CAC score of zero denotes a very low risk of CV mortality, and the risk increases with an increase in score. 21 There is a defined cutoff according to age, sex, and ethnicity for risk stratification. There is good repeatability and interobserver variability. Although studies have shown its usefulness in predicting CV events, there are a few controversies around it. The calcium score is based on the density of calcium, but there is an inverse association of CV events with plaque density. 22 Trained athletes have been found to have high CAC scores despite low risk for events. Statin therapy, although it reduces CV risk, has also been shown to increase plaque density and CAC score. This makes it not suitable to monitor CAC scores in patients taking statin. Despite all these limitations, the CAC score has shown a linear correlation with the risk of CV events across studies. 23 Plaque burden, as assessed by CAC score, may be a better predictor of future CV events than the presence of obstructive CAD. Prediction is superior when compared to Framingham risk score and pooled cohort equation (PCE).24, 25 Radiation exposure is a known limitation for this method. However, because of more objective assessment with less interobserver variability makes it suitable for frequent clinical use. Recent American Heart Association (AHA) primary prevention guidelines recommended the use of CAC scoring for better risk stratification for intermediate-risk groups and initiation of statin therapy. 26 Recent evidence questioned the role of aspirin use for primary prevention. Few studies suggest that CAC may even help to identify high-risk individuals who are more likely to benefit from aspirin. 27 CAC assessed from noncontrast CT chests done for other medical reasons also carries prognostic significance and can be used as a tool for optimal risk factor management. 28
Femoral Plaque
Atherosclerosis of iliofemoral arteries is more common than carotid arteries. However, this has not been studied extensively as carotid atherosclerosis as a predictor of CV event or mortality. Femoral plaque as defined by Manheim consensus includes focal structure encroaching into the lumen of at least 0.5 mm, or 50% of the surrounding intima-media thickness, or a total thickness of >1.5 mm. The majority of available studies involving imaging of femoral arteries assessing the presence of plaque and high-risk morphology (plaque ulceration) is a strong predictor of major CV events. 29
Calcification and Diameter of Abdominal Aorta
Calcification abdominal and thoracic aorta has also been linked to predicting coronary events. Aortic calcification is more common than coronary calcification and mostly assessed by a CT scan. Absence of calcium is considered normal. A score from 0 to 300 is considered as low and >300 as high. 30 Atheroembolism or thromboembolism from the aorta is often considered as source of embolic stroke. However, the prognostic value of aortic calcification itself is debated. 31 Normally aorta tapers gradually from ascending aorta till iliofemoral bifurcation. Aneurysmal dilation usually happens secondary to atherosclerosis-mediated weakening of the aortic wall. Aortic diameter measured by imaging (ultrasound, CT, MRI) at certain landmarks may predict future CV events. However, current evidence is not so robust with regard to aortic diameter.
Ankle–Brachial Index
Systolic blood pressure at the ankle should be about 1.1 times the brachial systolic pressure with normal arterial circulation. Reduction in the ankle systolic pressure suggests proximal aortoiliac stenosis. Ankle–brachial index (ABI) is measured as the ratio of systolic blood pressure (measured using a handheld Doppler) between the ankle and arm. ABI normally ranges between 1.0 and 1.39. A value less than 0.9 indicates obstructive atherosclerosis involving the descending aorta or femoral artery. MRI studies of femoral arteries showed a linear increase in plaque burden with the reduction in ABI. In high-risk individuals with normal resting ABI, exercise-induced decline is also shown to be associated with increased CV events. 32 MRI studies assessing femoral artery have shown that plaque burden increases linearly with a decrease in ABI below 1, in patients with intermittent claudication and in asymptomatic people. Metanalysis done by Ankle Brachial Index Collaboration concluded a reverse J-shaped relationship between ABI and all-cause mortality. 33 . Lowest mortality was observed with those who had an ABI value between 1.1 and 1.4. There was a linear increase in mortality with decline in ABI value below 1.1. Sometimes, false-negative high ABI suggests artery walls are stiff, calcified, and may be incompressible. In such a situation, the toe/brachial index may be a more reliable test to detect peripheral atherosclerosis. Current evidence is good enough to consider low ABI as a surrogate marker of subclinical atherosclerosis and predict future CV events in middle-aged to elderly.
Endothelial Function Test
Endothelial dysfunction has been established as part of the pathogenesis of atherosclerosis. This can be measured as flow-mediated dilation of brachial arteries. Impaired flow-mediated dilation is considered as endothelial dysfunction. However, there are mixed results in studies involving endothelial function tests predicting future CV events or mortality independent of CV risk factors. 34 Similarly, arterial stiffness measures (pulse wave velocity [PWV], augmentation index, wave reflection) have been suggested as markers of underlying atherosclerosis. Out of these, PWV has been shown as a predictor of future heart failure.
Current ASCVD Risk Assessment
Appropriate risk stratification remains the cornerstone for the primary prevention of future CV events. PCE, including traditional modifiable risk factors, assesses individuals’ 10-year ASCVD risk. Although it has been shown to underestimate and overestimate the risk in certain populations, PCE is now considered as the most effective method of risk assessment. 26 The role of the above-discussed noninvasive methods to detect subclinical atherosclerosis in further risk stratification is being explored. Out of all, CT assessment of coronary artery calcification (CAC) and carotid plaque has shown better predicting potential for future events. Risk factor management and lifestyle modification are suggested for all individuals, irrespective of risk stratification. However, drug therapy (statin) is recommended based on risk score. For those with borderline or intermediate risk scores, the role of preventive therapy is uncertain. Such individuals should be further risk stratified based on coronary calcium score (CAC). Those with higher scores may be considered candidates for preventive statin therapy. Although various noninvasive methods to detect subclinical atherosclerosis have shown their predicting potential, their routine clinical use still remains uncertain.
Therapeutic Implications
Diet, exercise, and control of modifiable risk factors remain cornerstones in the management and prevention of ASCVD. 26 Childhood and adult-onset obesity is a growing concern and needs to be addressed in time. Yoga and stress management have shown their role in the reduction of CV events. 35 Statin therapy has proven, beyond doubt, its role in the secondary prevention of CV events. However, their role in subclinical atherosclerosis is still being explored. The role of statin therapy after the detection of subclinical atherosclerosis in the prevention of future CV events has been assessed in various ways. CIMT-based studies showed plaque regression or delayed progression with statin therapy.36, 37 Coronary intravascular imaging-based studies showed a reduction in atherosclerosis burden with statin therapy. 38 This reversal effect is almost similar between high-intensity atorvastatin and rosuvastatin. 39 Stabilization of plaque was observed as early as one month and further reversal over time. 40 In patients with high CAC scores, statin therapy has been shown to reduce CV events, although CAC score increases with therapy. 41 Current recommendations for primary prevention of CV events include lifestyle measures, risk factor control, and statin therapy in intermediate to high-risk score. 26 In adults at intermediate risk, CAC measurement can be used for further reclassifying risk. Statin therapy is reasonable in those with CAC ≥100 AU or CAC ≥75th percentile. The role of aspirin is well-established in the management of established ASCVD. However, its added benefit over statin for primary prevention is controversial and may be considered in adults (40-70 years of age) with higher ASCVD scores and low bleeding risk. 26 Angiotensin-converting enzyme (ACE) inhibitors have shown their benefit in secondary prevention. However, its benefit in subclinical atherosclerosis needs further studies. Drugs targeting inflammation, such as colchicine and canakinumab, have shown benefits in secondary prevention. Their role in the subclinical stage needs further exploration. Various genetic focuses have been explored in the pathogenesis of atherosclerosis, and targeted gene therapy may be the way out to prevent subsequent CV events. With this growing body of evidence, drug therapy may be instituted more frequently with the detection of subclinical atherosclerosis to prevent subsequent events. Similarly, lifestyle modification and smoking cessation can be reinforced with more objective evidence of subclinical atherosclerosis.
Conclusion
Atherosclerotic CV disease has a long subclinical stage, which can be targeted to prevent future CV events. Various noninvasive methods explored to detect subclinical atherosclerosis and predict future CV events. Strict risk factor control and statin therapy can be used more judiciously targeting subclinical atherosclerosis to reduce future events.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.