
Abstract
Transvenous endocardial pacing of the right ventricle normally produces a QRS complex of left bundle branch block pattern (LBBB) on electrocardiogram. Although a paced right bundle branch block (RBBB) pattern can draw suspicion to lead perforation or displacement, it can also be a benign change. We present a case of a 56-year-old man who presented with dyspnea and was found to have a paced rhythm of RBBB morphology.
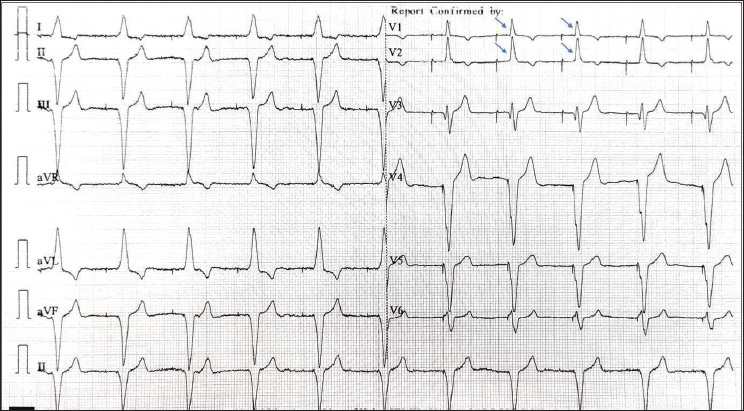
A 56-year-old man visited the outpatient department with complaints of dyspnea for 1 week. He had a history of dual chamber pacemaker (DDDR) implantation in 2005 for complete atrioventricular block and had undergone two pulse generator replacements in 2010 and 2023. An electrocardiogram (ECG) was performed, which revealed atrial-paced, ventricular-paced rhythm, and a right bundle branch block (RBBB) morphology in leads V1 and V2 (Figure 1). A previous ECG taken a few days earlier had shown a ventricular-paced rhythm with left bundle branch block (LBBB) morphology. This change raised concerns about possible lead perforation or displacement, although perforation at this late stage (19 years after implantation) is very rare.
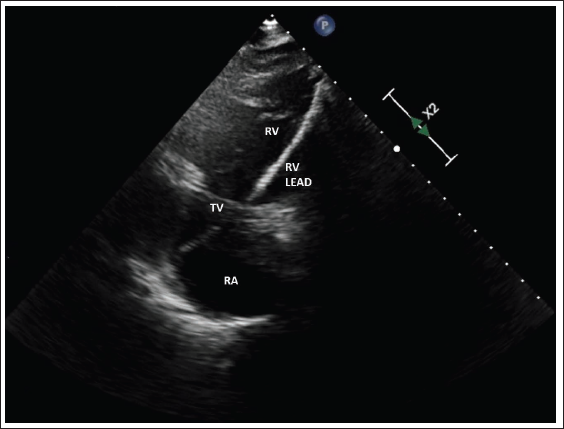
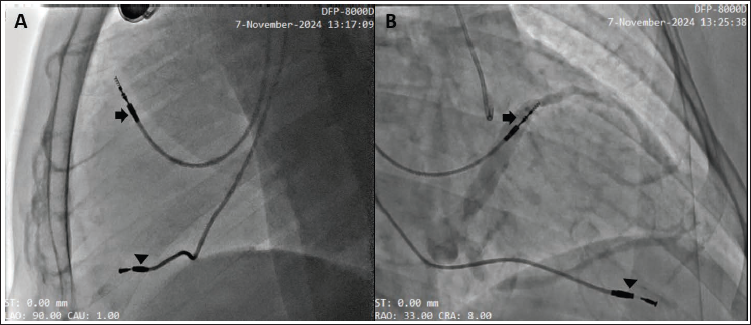
Chest X-ray showed the normal position of both atrial and ventricular leads. Echocardiogram (ECHO) showed the ventricular lead passing through the tricuspid valve toward the right ventricle (RV) apex near the interventricular septum (Figure 2), with no signs of pericardial effusion. Fluoroscopy in left anterior oblique (LAO) 90° and right anterior oblique (RAO) 30° views confirmed the normal position of the atrial and ventricular leads (Figure 3), and pacemaker interrogation showed normal parameters.
ECHO Showing the Ventricular Lead Traversing the Tricuspid Valve Toward the RV Apex.
Fluoroscopy in LAO 90° (A) and RAO 30° (B) Views Demonstrating the Atrial Lead (Arrow) and Ventricular Lead (Arrowhead) in Normal Positions.
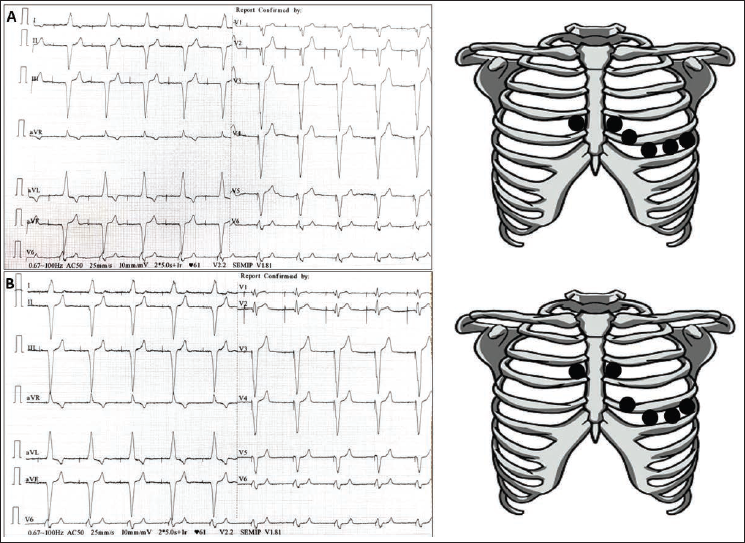
Based on these findings, we conducted a repeat ECG after confirming that all chest and limb leads were correctly placed. The new ECG indicated a paced rhythm consistent with an LBBB pattern (Figure 4A). To investigate the change in QRS morphology, we performed another ECG, this time positioning the V1 and V2 electrodes one intercostal space higher. This subsequent ECG displayed a paced RBBB rhythm in leads V1 and V2 (Figure 4B), which was similar to the original ECG. By adjusting the position of the ECG electrodes, we were able to replicate the initial-paced RBBB rhythm, suggesting that the alterations observed in the initial ECG were likely due to improper electrode placement.
Normally, transvenous endocardial pacing of the right ventricle leads to an LBBB pattern on ECG. A paced RBBB pattern can occur if there is inadvertent pacing of the left ventricle through a congenital septal defect such as patent foramen ovale (PFO), atrial septal defect (ASD) or ventricular septal defect (VSD), or in the coronary sinus, or rarely by retrograde transarterial pacing. It can be seen in lead perforation of the right ventricular free wall or interventricular septum. It can also be observed in deep lead screw fixation, causing earlier activation of the LBB area.
However, a paced RBBB rhythm can be seen in patients with correctly placed ventricular leads. This so-called pseudo-RBBB pattern can occur in up to 22% of patients. 1 Apical lead positioning is associated with a significantly higher likelihood of pseudo-RBBB pattern than mid-septal positioning. 2 It is crucial to be able to differentiate between the complicated RBBB pattern and the pseudo-RBBB pattern because the former requires intervention.
One simple way to do this is by repositioning the V1 and V2 ECG electrodes. This maneuver was first described by Klein et al., 3 who found that placing the V1 and V2 electrodes one intercostal space lower can remove the RBBB pattern, while positioning them one intercostal space higher can enhance the RBBB pattern, which is evident in our patient. However, this technique may not always be effective. Assessment of the frontal plane axis and precordial transition can be very reliable. A frontal plane axis between 0° and −90° and precordial transition by V3 is highly specific for RV apical or septal pacing. 4
A careful analysis of the 12-lead ECG provides a quick and inexpensive way to distinguish malposition and pseudo-RBBB pattern. This avoids the use of unnecessary anticoagulation, fluoroscopy, and lead replacement.
Footnotes
Data Availability
ECG/ECHO/fluoroscopy is available on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent for publication was provided by the participant.