
Abstract
Introduction
Recent years have highlighted a special emphasis on the association between Atherosclerosis and D-Dimer and Fibrinogen levels. The purpose of the study was to determine their function as supplementary diagnostic tools in patients of ACS (Acute Coronary Syndrome).
Materials and Methods
The study included 100 participants (50 controls and 50 cases), categorized into STEMI (ST Elevation Myocardial Infarction), NSTEMI (Non-ST Elevation Myocardial Infarction), and UA (Unstable Angina) based on ECG and Trop-T positivity. D-Dimer and Fibrinogen levels were measured for both controls and cases. Chi-square, Student t-test and ANNOVA test were used by SPSS-PC-25 version. The assessment of cut-off points was carried out using receiver operating characteristic (ROC) curve analysis.
Results
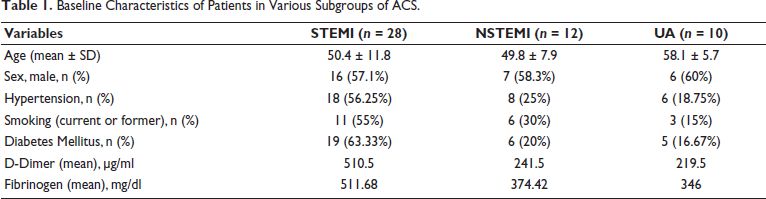
Mean D-Dimer was 510.5 µg/ml in STEMI, compared to 241.5 µg/ml in NSTEMI and 219.5 µg/ml in UA. Fibrinogen levels were higher in STEMI (511.68 mg/dl) than in NSTEMI (374.42 mg/dl) and UA (346.10 mg/dl). At a D-Dimer cut-off of 420.5 µg/ml, sensitivity and specificity for ACS prediction were 42% and 96%, respectively; for Fibrinogen at 368.5 mg/dl, they were 68% and 82%. For STEMI, at a D-Dimer cut-off of 354 µg/ml, sensitivity and specificity were 78.57% and 95.45%, while for Fibrinogen at 321 mg/dl, they were 85.71% and 50%.
Discussion
In our study, D-Dimer and Fibrinogen were measured in all the subjects of control group and ACS group and both the parameters were increased in the ACS group with an average of 340 (232-588.25) µg/ml and 453 mg/dl (standard deviation ±201.1) respectively. On the other hand, the control group showed an average D-Dimer of 210.5 µg/ml and Fibrinogen of 270.42 mg/dl (standard deviation ±104.33) which were both within the normal range. Both D-Dimer and Fibrinogen were also calculated for all the subgroups of ACS and the results showed the highest values in the subjects of STEMI.
Conclusion
D-Dimer and Fibrinogen levels were significantly higher in patients with Acute Coronary Syndrome, particularly in the STEMI subgroup, and can be used as supplementary diagnostic markers.
Introduction
Acute Coronary Syndrome (ACS) describes a pathological condition characterized by myocardial ischemia, resulting from a disparity between the oxygen demand of the heart and the available blood supply. This imbalance is primarily caused by the obstruction resulting from plaque formation within the coronary arteries. It is the most frequent reason for hospitalization globally and the leading cause of mortality in the industrialized world, accounting for one in every five fatalities 1 . Accurate and prompt diagnosis, coupled with economical care for ACS, holds paramount importance due to the substantial morbidity, mortality, and socioeconomic consequences linked to this illness. Over the years, the assessment of cardiac enzymes, including Troponin T and Troponin I, has been instrumental in evaluating chest pain, particularly in identifying whether it is linked to acute myocardial ischemia. Although both markers, particularly Troponin T, exhibit low sensitivity in the hyper acute phase, which is within a few hours after the initiation of ACS, these enzymes are notably precise and sensitive, serving as critical tools for the diagnosis of myocardial injury 2 . However, significant myocardial necrosis is typically preceded by local thrombus formation and inflammation. The goal of novel cardiac biomarkers is to identify these severe manifestations of inflammation. Hence, attempts continue to find a superior and faster way to diagnose ACS. Recent years have witnessed significant focus towards understanding the connection between the inflammatory elements of plaque and the development of atherosclerosis and studies have demonstrated a relationship between the prognosis of individuals suffering from ACS and several biochemical markers, including Homocysteine, Low-Density Lipoprotein (LDL), C-Reactive Protein (CRP), D-Dimer, Fibrinogen, Plasmin-α2 Antiplasmin, Prothrombin, Activated factor VII, etc. It is hypothesized that the levels of these biomarkers will alter as coronary vascular thrombosis occurs more frequently 2 . D-Dimer represents a distinct degradation product derived from the cross-linked fibrin that is generated after activation by the fibrinolytic system. Its presence signifies active formation and dissolution of thrombi. Increased levels of D-Dimer in plasma are indicative of a greater degree of fibrin synthesis and degradation occurring in the body. D-Dimer is usually absent in human blood unless the coagulation cascade is activated, for example by the presence of thrombosis or Disseminated Intravascular Coagulation. Since D-Dimer develops faster than other inflammatory indicators in the ACS pathophysiology, D-Dimer levels are expected to increase faster than other cardiac markers in acute ischemia 3 . Fibrinogen, on the other hand, is an important component of blood coagulation and a major component of thrombus, which is converted to fibrin by thrombin, which induces clot formation. Plasma Fibrinogen plays a major role in the inflammatory response, endothelial dysfunction and smooth muscle cell migration 4 . Additionally, a high level of plasma Fibrinogen causes increased blood viscosity, which impairs circulation, damages endothelial cells under shear stress, and raises the risk of thrombosis 5 . In healthy individuals, elevated Fibrinogen levels are a strong risk factor for cardiovascular disease. Additionally, it is a predictor of accelerated coronary atherosclerosis and a risk factor for myocardial ischemia recurrence in patients with prior coronary events. Thus, elevated plasma D-Dimer and Fibrinogen levels might cause a hyper-coagulative state that could affect the degree and duration of formation of thrombus at the time of coronary insult. Thus, the present study is being undertaken to establish their roles as additional diagnostic markers for the diagnosis of an Acute Coronary event.
Materials and Methods
Research Design and Setting
This cross sectional study was conducted in the Medical Emergency (Department of Medicine) and Department of Pathology from 1st January 2021 to 31st May 2022. The study included a total of 100 subjects divided into two equal groups of Cases and Controls. Patients eligible for inclusion in the study were those aged 18 years and older, experiencing their first occurrence of typical chest pain. This pain was defined as a substernal discomfort that arose during physical activity and was alleviated by either rest or nitroglycerin, conforming to the Universal criteria for myocardial infarction as specified in the latest European Society of Cardiology guidelines 6 . Exclusion criteria were any history of surgery, trauma or coronary revascularization within 6 months, known cases of CAD already on treatment and any co-existing confounding condition known to modify D-Dimer levels such as cerebrovascular disease, peripheral vascular disease, hepatic insufficiency, renal insufficiency, malignancy or sepsis. Age and sex matched people above the age of 18 years without any comorbidity or prior history of CAD were chosen as Controls.
Data Collection
The data collection process involved a thorough examination of the subjects’ medical histories, emphasizing the timing of chest pain onset, the characteristics of the pain, its response to rest, and the presence of associated symptoms such as excessive perspiration, vomiting, shortness of breath, and fatigue. Furthermore, the subjects were questioned about their smoking habits, alcohol consumption, history of hypertension, diabetes, and any pertinent family medical history. Complete general and systemic examination was done to assess BMI, hemodynamic stability, signs of congestive cardiac failure and/or cardiogenic shock. All patients were subjected to ECG (12-lead with Rhythm Strip) and Routine blood-based Investigations like CBC, KFT, LFT, Electrolytes, Fasting blood glucose, Lipid profile and Cardiac enzymes. Trop T was measured qualitatively by Trop T kits based on immunological test and 2D Echo was done. Serum D-Dimer and Fibrinogen levels were calculated by Automated Coagulometer Elite Pro at 37°C on presentation by collecting blood sample in Sodium Citrate vacutainer. Subsequently, based on the results of the ECG and positive Troponin-T test, the cases were classified as STEMI, NSTEMI or UA.
Ethical Consideration
This study was approved by the Institutional Ethics Committee. Every patient was adequately informed about the outlined plan, and written consent was obtained from all of them.
Data Entry and Statistical Analysis
The data collected was reformulated into variables, encoded, and recorded in Microsoft Excel. The analysis and statistical evaluation of this data were carried out using SPSS-PC-25 version. The Shapiro-Wilk normality test was employed to assess the normal distribution of various parameters.
Quantitative data were presented as mean ± standard deviation (SD) or median with interquartile range. The comparison of normality between two groups was conducted using the Student’s t-test or the Mann-Whitney U test. For comparisons involving more than two groups, the analysis was performed using either the ANOVA test or the Kruskal-Wallis H test. Qualitative data were expressed in frequency and percentage and difference between proportion were tested by chi square test. ROC curve was prepared using D-Dimer and Fibrinogen level to predict ACS and then STEMI in ACS subjects and based on that cut off value was calculated. Sensitivity, specificity, PPV and NPV of D-Dimer and Fibrinogen was calculated to predict ACS and then STEMI in ACS subjects. P’ value less than 0.05 was taken as statistically significant.
Results
Baseline Characteristics
The study group comprised of individuals whose ages varied from 28 years to 80 years, with the mean age being 51.84 years (SD ± 10.39) in the ACS group and 47.22 years (SD ± 13.43) in the control group. Majority of the subjects included in the study were between 56-65 years (24%) in the ACS group and 36-45 (28%) in the control group. The ACS group consisted of 3 subgroups: STEMI, NSTEMI and UA. Out of the total 50 subjects in the group, 28 (56%) belonged to the STEMI group, 12 (24%) belonged to the NSTEMI group and 10 (20%) belonged to the UA group (Table 1).
Baseline Characteristics of Patients in Various Subgroups of ACS.
D-Dimer and Fibrinogen Levels
D-Dimer and Fibrinogen were calculated in all the sub groups of ACS and control subjects. The normal ranges of D-Dimer and Fibrinogen according to the equipment used (Automated Coagulometer Elite Pro) during the study was <250 µg/ml and 200-400 mg/dl respectively. The ACS group exhibited increased levels of D-Dimer and Fibrinogen with an average of 340 (232-588.25) µg/ml and 453 mg/dl (SD ±201.1) respectively. The control group showed an average D-Dimer of 210.5 µg/ml and Fibrinogen of 270.42 mg/dl (SD ±104.33) which were both in the normal range.
Subgroup Analysis
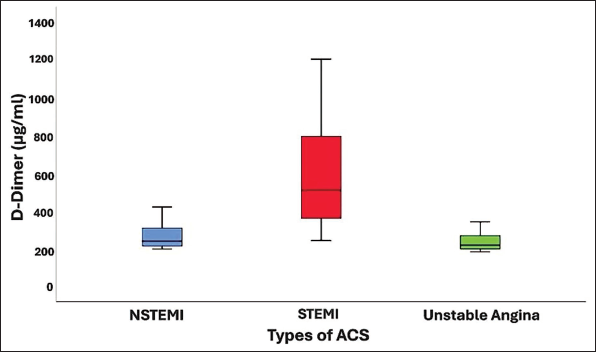
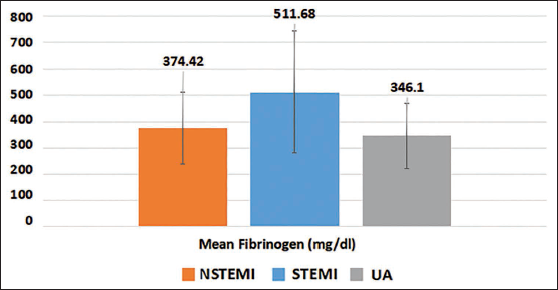
The levels of D-Dimer and Fibrinogen were markedly elevated in the STEMI cohort compared to other types of ACS (NSTEMI and UA). Mean D-Dimer was 510.5 µg/ml in the STEMI sub group whereas it was just 241.5 µg/ml in NSTEMI and 219.5 µg/ml in UA (Figure 1). Fibrinogen was also higher in STEMI (511.68±231.76 mg/dl) as compared to NSTEMI (374.42±137.37) and UA (346.10±123.71) subjects (Figure 2).
Boxplot Showing Comparison of D-Dimer Between Subgroups of ACS.
Comparison of Fibrinogen Between Subgroups of ACS.
Diagnostic significance of D-Dimer and Fibrinogen
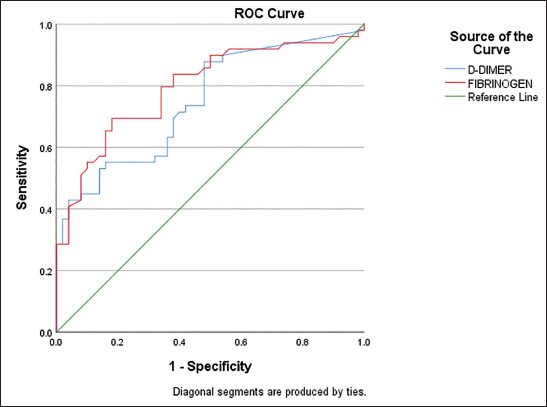
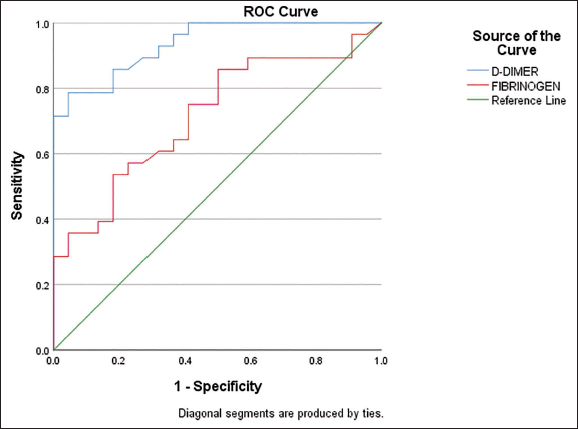
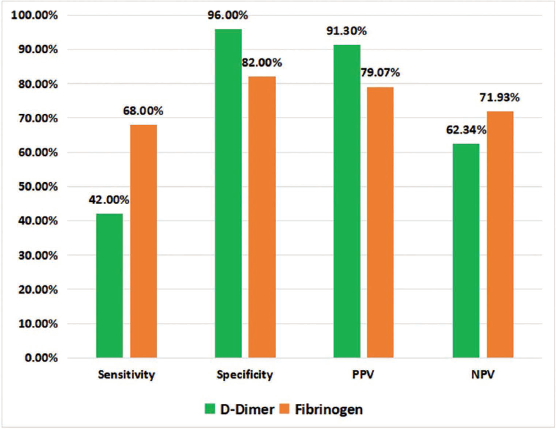
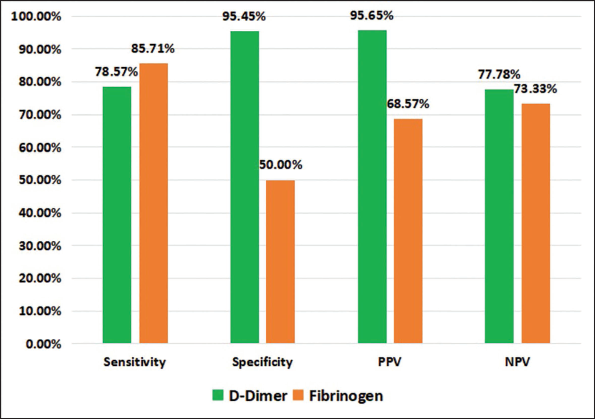
A Receiver Operating Characteristic (ROC) curve was used to determine the cut-off point with maximum sensitivity and specificity of D-Dimer levels in the diagnosis of ACS (Figure 3 & 4). At cut-off of 420.5 µg/ml, Sensitivity & Specificity of D-Dimer to predict ACS was 42% & 96% while the Sensitivity & Specificity of Fibrinogen was 68% & 82% at cut off of 368.5 mg/dl (Figure 5). At cut-off of 354 µg/ml, Sensitivity & Specificity of D-Dimer to predict STEMI was 78.57% & 95.45% while the Sensitivity & Specificity of Fibrinogen was 85.71% & 50% at cut off of 321 mg/dl (Figure 6).
ROC Curves Analysis Using D-Dimer and Fibrinogen for Predicting ACS.
ROC Curves Analysis Using D-Dimer and Fibrinogen for Predicting STEMI.
Sensitivity, Specificity, PPV, NPV of D-Dimer and Fibrinogen for Predicting ACS.
Sensitivity, Specificity, PPV, NPV of D-Dimer and Fibrinogen for Predicting STEMI.
Discussion
This study explored the potential of D-Dimer and Fibrinogen as supplementary diagnostic markers for patients with Acute Coronary Syndrome, yielding favorable results.
Currently, one of the most accurate indicators for identifying myocardial injury is the measurement of Troponin levels 7 . However, their primary disadvantage is an increase in serum level 3 to 4 hours after the onset of symptoms. Therefore, it is still believed that new biomarkers need to be evaluated for the faster diagnosis of coronary thrombosis as a hallmark of ACS.
Numerous studies have already demonstrated the involvement of D-Dimer and Fibrinogen in the development of atherosclerosis8, 9. As the principal degradation product of cross-linked fibrin, D-Dimer may act as a direct marker for the presence of ongoing fibrinolytic activity. Because plasma concentration of D-Dimer reflects the presence of active fibrin degradation, measurement of D-Dimer has proven clinically useful in the diagnosis of acute venous thrombosis, pulmonary embolism, and disseminated intravascular coagulation10, 11. In contrast, the effect of Fibrinogen levels on cardiovascular disease parallels that of key risk factors such as elevated blood pressure, smoking, and diabetes. A notable association has been established between Fibrinogen levels and the likelihood of coronary heart disease 12 .
In our study, D-Dimer and Fibrinogen were measured in all the subjects of control group and ACS group. The ACS group showed elevated levels of both D-Dimer and Fibrinogen, while their average levels remained within the normal range in the control group. This result was in accordance with the study done by Antoni Bayes-Genis et al 13 in which Individuals experiencing acute ischemic events, such as myocardial infarction and unstable angina, exhibited significantly higher D-Dimer and Fibrinogen levels compared to non-ischemic patients. This was also similar to the study results of Mohammad Shojaie et al 14 in which the mean plasma Fibrinogen in ACS patients (354.9 ± 60 mg/dl) was elevated markedly compared with the control group (329 ± 73 mg/dl). Both D-Dimer and Fibrinogen were also calculated for all the subgroups of ACS and the results showed the highest values in the subjects of STEMI. Mean values of D-Dimer in STEMI, NSTEMI and UA were 510.5 µg/ml, 241.5 µg/ml and 219.5 µg/ml respectively. Similarly, the mean values of Fibrinogen in STEMI, NSTEMI and UA were 511.68 mg/ml, 374.42 mg/ml and 346.10 mg/ml respectively. This finding was found to be statistically significant. Similar results were observed in studies done by Falgun Gosai et al 15 in which highest values of D-Dimer were found in the subgroup of STEMI. Using ROC curve analysis, the cut off values of D-Dimer and Fibrinogen for predicting ACS showed high specificity of 96% and 82.0% respectively. Since both the mean values D-Dimer and Fibrinogen were found to be highest in the STEMI subgroup, ROC curve was again applied to find out the best discriminate power and the cut off value of D-Dimer for predicting STEMI again showed high sensitivity and specificity.
The primary aim of our study was to assess the effectiveness of these two coagulation markers in the early diagnosis of ACS and to establish their potential as novel diagnostic tools. The remarkable potential of D-Dimer is its capacity to reveal persistent thrombus formation and dissolution in patients with myocardial injury, a phenomenon that is overlooked by traditional diagnostic methods. Apart from its role in diagnosing myocardial infarction, D-Dimer could serve as a valuable prognostic indicator as well. For patients with UA and lower basal D-Dimer levels, D-Dimer prognostic data may be especially helpful. Lee et al 16 showed that marked increases in circulating D-Dimer are indicative of thrombotic complications in patients with MI, suggesting that D-Dimer, besides being useful as a marker for early diagnosis, is also a risk factor for the development of MI complications. Our study is limited by a small sample size and the lack of follow up analysis of cardiovascular event and mortality. Nonetheless, our findings imply that the observed elevations in D-Dimer and Fibrinogen are probably a reflection of increased physiological fibrinolysis, resulting from ongoing thrombosis or a more intense fibrinolytic response to coronary thrombosis.
Conclusion
Our study findings suggest that assessing serum D-Dimer and Fibrinogen levels could serve as a promising biomarker with high sensitivity for diagnosing suspected Acute Coronary Syndrome. Given its significant sensitivity in identifying STEMI, D-Dimer serves as a valuable tool for the proper triage of patients, ensuring their timely referral to a cardiologist for early coronary interventions. However, it is recommended that additional cardiac biomarkers must be utilized alongside D-Dimer and Fibrinogen to enhance their diagnostic capabilities.
Strengths of the Study
The study employed reliable and validated measurement tools, enhancing the accuracy and credibility of serum D-Dimer and Fibrinogen levels in diagnosing patients suspected of having ACS, particularly ST-Elevation Myocardial Infarction (STEMI).
The study’s sample size and careful control of variables strengthen the reliability of its findings, ensuring that the results are both statistically significant and generalizable to broader patient populations. Additionally, the use of validated laboratory techniques for serum measurements allowed for the control of confounding variables, providing a clearer understanding of the relationships between key factors.
While the results underscore the diagnostic potential of D-Dimer and Fibrinogen, the study also recommends combining these biomarkers with other cardiac markers to enhance their diagnostic accuracy. This thoughtful approach to combining biomarkers addresses the complexity of ACS diagnosis and provides a pathway for future research.
The study’s comprehensive methodology, adherence to ethical standards, and innovative use of serum biomarkers for early ACS diagnosis make it a valuable contribution to cardiology research, with the potential to shape clinical practices and enhance patient outcomes in the future.
Limitations of the Study
The study had a small sample size of 50 cases only, therefore more studies with a large sample size need to be undertaken.
Coronary angiography to confirm the diagnosis was not performed in this study.
D-Dimer and Fibrinogen levels were only measured at the time of presentation, so no data is available whether revascularization alters the values of the same.
This study lacked the follow up analysis of cardiovascular event and mortality
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Study titled ‘D-Dimer and Fibrinogen Levels as Additional Diagnostic Markers in Patients with Acute Coronary Syndrome’ was approved by the Institutional Ethics Committee, Atal Bihari Vajpayee Institute of Medical Sciences and Dr Ram Manohar Lohia Hospital, New Delhi on 29 December 2020 through the Approval number TP (MD/MS) 6 of 7 (111/2020)/IEC/ABVIMS/RMLH/377.
Informed Consent
Informed written consent was taken from all the participants.
Data Availability Statement
All data generated or analyzed during this study are included in this published article [and its supplementary information files].