
Abstract
Introduction
Left ventricular (LV) hypertrophy and high filling pressure in severe aortic stenosis (AS) cause impairment in coronary flow reserve. This results in LV myocardial ischemia, resulting in impairment in longitudinal shortening.
Aim
To study the role of LV global longitudinal systolic strain (LVGLS) imaging in identifying subclinical LV dysfunction and to determine the correlation between LVGLS and N-terminal pro-B-type natriuretic peptide (NT pro-BNP) in asymptomatic patients having severe AS and preserved left ventricle ejection fraction.
Methodology
This study included 33 asymptomatic patients with severe AS and 30 age- and sex-matched control groups. The ejection fraction was measured using the modified Simpson technique. LVGLS was measured with a two-dimensional speckle tracking analysis on apical 2, 3, and 4 chamber views.
Results
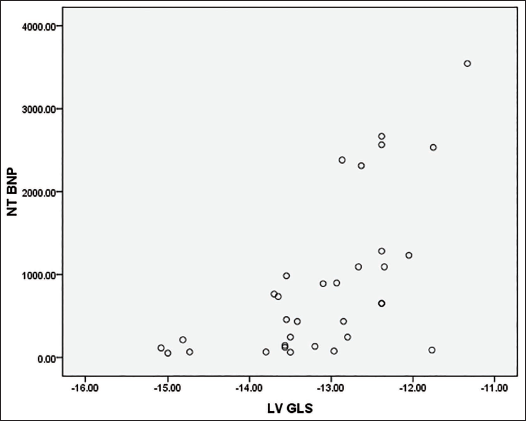
LVGLS was significantly reduced in asymptomatic severe aortic stenosis with normal ejection fraction compared to the normal control group without aortic stenosis (P < .001). There is a positive correlation between impairment of LVGLS and left ventricular mass index (LVMI), the pressure gradient across the aortic valve, and the valve area. There is a linear correlation between NT pro-brain natriuretic peptide (BNP) and LVGLS (r value 0.447); as the LVGLS decreases, NT pro-BNP increases.
Conclusion
LVGLS can be used as a reliable indicator for the detection of subclinical LV dysfunction in asymptomatic severe aortic stenosis patients with preserved ejection fraction.
Introduction
Usually, the systolic function of the left ventricle is assessed in terms of ejection fraction (left ventricle ejection fraction [LVEF]). However, the LVEF is usually preserved in AS, particularly if there is no coronary artery disease (CAD), and the concomitant presence of severe aortic stenosis (AS) and reduced LVEF is uncommon 1 in asymptomatic individuals. According to the latest guidelines, systolic dysfunction is a class I indication for aortic valve replacement (AVR) in severe AS, even in asymptomatic patients.2, 3 In most patients, symptoms begin long before LVEF decreases. However, symptoms in patients with AS may be difficult to detect, as these are often attributed to old age, and patients modify their lifestyle to a lesser functional capacity. Valvular intervention is currently recommended in cases of very severe AS (mean gradient above 60 mmHg or Vmax >5 m s−1), evidence of heavy calcification of the aortic valve as per cardiovascular computed tomography (CCT) assessment, features of rapid disease progression, and markedly increased brain natriuretic peptide. Exercise testing is often considered useful in determining whether the patient is truly asymptomatic. However, in those who are unable to perform this test, additional investigations are needed to decide the timing of the intervention. Concentric left ventricular hypertrophy and increased LV mass are predictors of poor outcomes, and even residual increase of LV mass after intervention leads to reduced postoperative survival. 4 Even though conventional echocardiography is useful in detecting significant LV dysfunction, it is not good for identifying subclinical dysfunction. Furthermore, many studies concluded that impairment of left ventricular global longitudinal systolic strain (LVGLS) is an independent predictor of mortality irrespective of AS severity (Figure 1). 5
Thus, with this study, our goal is to identify subclinical LV dysfunction in patients with asymptomatic severe AS but normal ejection fraction, according to GLS imaging, and its correlation with N-terminal pro-B-type natriuretic peptide (NT pro-BNP).
The objectives of the study are given below:
Material and Methods
Inclusion Criteria
In total, 33 patients with asymptomatic severe aortic stenosis with LVEF >50% and 30 healthy individuals were included in the study.
Exclusion Criteria
Exclusion criteria included patients with moderate to severe valvular regurgitation, subvalvular AS, mitral stenosis, known cases of CAD, and patients with atrial fibrillation or artificial pacing.
Data Collection and Methodology
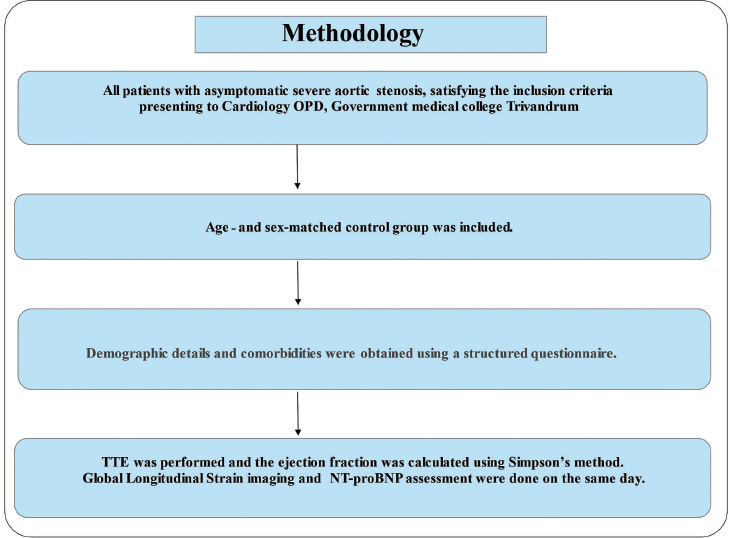
All patients with asymptomatic severe aortic stenosis who attended the cardiology department at Government Medical College, Thiruvananthapuram were included in the study. Demographic details and comorbid conditions were noted using a predefined pro forma after getting informed written consent from the patients; those who met the exclusion criteria were excluded from the study.
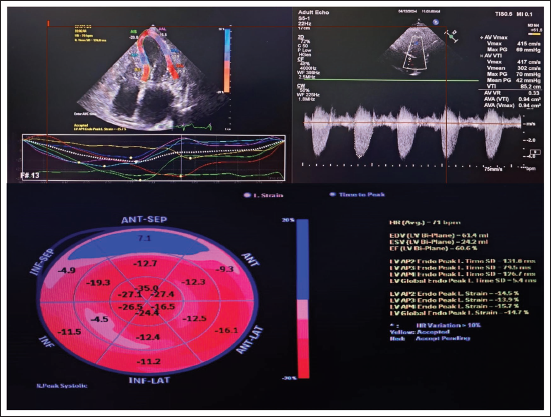
Age- and gender-matched control groups were enrolled, and data were collected. All patients were subjected to two-dimensional (2D) echocardiography to confirm the diagnosis and severity assessment of AS. All patients who satisfied the inclusion criteria of severe aortic stenosis as per the latest European Society of Cardiology (ESC) guidelines (severe AS was diagnosed when maximum velocity across aortic valve >4 m s−1, mean gradient >40 mmHg, or aortic valve area (AVA) <1.0 cm2) were enrolled in the study after getting informed written consent. The ejection fraction of these patients was calculated using the Simpsons method. The patients were further subjected to serum NT pro-BNP levels, and GLS and 2D strain imaging were obtained. 2D echocardiography images were obtained from LV apical 3C, 4C, and 2C views. LV endocardial borders were manually traced, and the speckle tracking width was adjusted to cover the entire left ventricular wall thickness to obtain curves for peak longitudinal strain. LVGLS was calculated from the average of the peak systolic values of the six LV walls (Figure 2).
For all patients included in the study, NT pro-BNP was obtained on the same day of the echocardiography assessment.
Ethical Considerations
Data collection was started only after getting ethical clearance.
Privacy of the patient and confidentiality of clinical data were maintained throughout the study.
Informed written consent was taken before inclusion in the study.
The study was done without any additional expense to the patient.
Echo details measured are given below:
Velocity across the aortic valve (Vmax). Maximum aortic valve pressure gradient (PG) and mean aortic valve pressure gradient. AVA calculated using the continuity equation. The LVEF%—calculated by Simpson’s biplane method of disks.
Global longitudinal strain values are collected as follows:
Basal: anterior, antero-septal, inferio-lateral, antero-lateral, inferio-septal, and inferior. Mid: anterior, inferior, antero-septal, inferolateral, antero-lateral, and inferoseptal. Apical: anterior, inferior, lateral, and septal. APEX.
Statistical Analysis
All obtained data were analyzed by Statistical Analysis for Social Sciences software version 16 as percentages and qualitative variables, means, standard deviations, and ranges were compared for quantitative variables. Student’s t-test was used to compare continuous distributions between patients with aortic stenosis and healthy controls. Categorical variables were compared with Fisher’s exact test and chi-square test.
Results
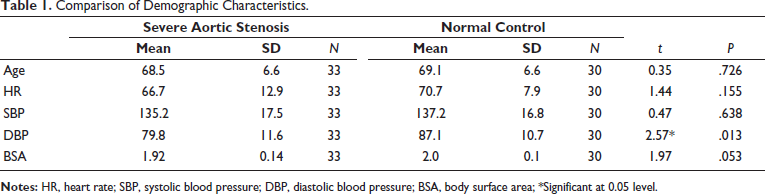
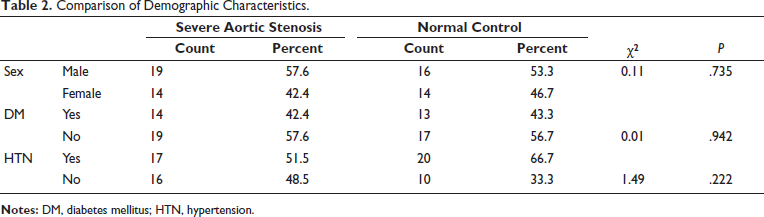
Baseline parameters like age, gender, heart rate, blood pressure, and ejection fraction (EF) were similar in both case and control groups (Table 1). Intravascular ultrasound (IVS) and posterior wall thickness were significantly higher in the case group (<0.01). Left ventricular mass index (LVMI) was significantly elevated in the case group (132.1 ± 23.7) when compared to the control group (83 ± 15.8) with a P value < .01. When LAVI was compared with the case versus control group, it showed a statistically significant elevation of LAVI in the case group (39.6 ± 4.4 and 33.8 ± 2.5) P value < .001. Diastolic dysfunction was significantly higher in the case group (normal: 21.2%; grade 1: 21.2%; grade 2: 36.4%; grade 3: 21.2%) when compared to the control group (normal: 67%; stage 1: 10%; stage 2: 23%) P value < .001 (Table 2).
Comparison of Demographic Characteristics.
Comparison of Demographic Characteristics.
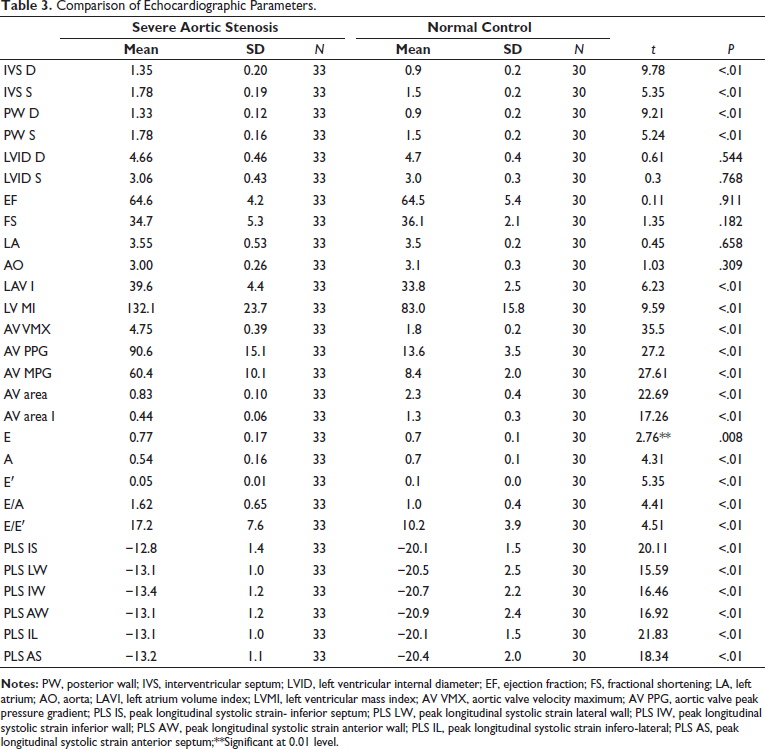
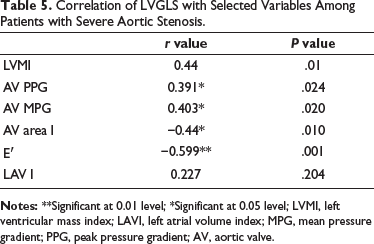
LVGLS was significantly reduced in the case group (−13.11 ± 0.9) when compared with the control group (−20 ± 1.3) P values < .01. The NT pro-BNP level was significantly elevated in the case (885.3 ± 123) than with control (85.03 ± 54) with a P value < .001 (Table 3). LVGLS was significantly reduced in patients with higher LVMI with a P value < .001. When mean and peak gradients across the aortic valve were compared with LVGLS, it was shown that as the gradient is increased, LVGLS is decreased, with a P value < .001. Similarly, when LVGLS was compared with the aortic valve index, it showed that as the valve area was decreased, LVGLS was also reduced, with a P value < .001. When GLS was compared with diastolic dysfunction, GLS was significantly decreased in patients with diastolic dysfunction. LAVI was statistically significant when compared with LVGLS, as LVGLS was reduced, LAVI was found to be elevated. NT pro-BNP was significantly elevated in patients with reduced GLS, with a P value < .00 and an r value of 0.447 (Table 4 and Figure 3).
Assessment of GLS in a Patient with Severe Aortic Stenosis.
Methodology.
Correlation Between NT BNP and LVGLS in Patients with Asymptomatic Severe Aortic Stenosis.
Comparison of Echocardiographic Parameters.
LVGLS and NT Pro-BNP in Patients with Severe AS and Normal Controls.

Correlation of LVGLS with Selected Variables Among Patients with Severe Aortic Stenosis.
Discussion
Management of patients with severe AS, whether conservative or interventional, is still a matter of controversy, especially in asymptomatic patients. LV fractional shortening and LVEF are obtained by measuring endocardial displacement and tend to overemphasize systolic function in the presence of concentric LV hypertrophy (which is seen frequently in severe AS). LVEF represents the ratio between end-diastolic and end-systolic left ventricular volume but does not assess the intrinsic contractile function of the myocardium.
In our study, 33 symptomatic AS and 30 normal patients were enrolled. Although EF was similar in the two groups, LVGLS and NT pro-BNP were considerably deranged in the case group.
In this study, GLS was markedly reduced in the case group when compared to the control group. Thus, it showed that even if EF was normal, there was an ongoing LV dysfunction in patients with asymptomatic severe AS. This observation was identical to a study done by Younan et al., 6 in which 50 asymptomatic patients with severe AS and 30 matched healthy controls were compared and showed significantly reduced GLS (−12.7 ± 3.6) in the case compared to the control (−12.7 ± 3.6) versus −19.3 ± 2.7 with P < .001. Similarly, a study by Vollema et al. 7 showed similar results: LVGLS −17.9% in asymptomatic severe aortic stenosis versus −19.6% in age- and sex-matched healthy controls (P < .001). As the left ventricle contracts in systole, it shortens in the longitudinal and circumferential direction (negative strain) and thickens in the radial direction (positive strain). This change in dimensions is measured and indicated as a percentage of its diastolic length or thickness. This change in length or thickness is called the strain or deformation. Longitudinal shortening is accountable for 60% of the left ventricular ejection and is an essential component of systolic function. So, this dysfunction of LV global longitudinal strain may be due to increased LV afterload, subendocardial ischemia, and LV myocardial fibrosis, and these may anticipate a poor outcome even after AVR. In a study by Kusunose et al., 5 LVGLS was observed as an important predictor of mortality and was significant in the prognosis of patients with severe aortic stenosis.
Another observation in our study was a significant correlation between left ventricular mass index and LVGLS in which patients with higher LVMI had lower LVGLS. This came in agreement with another study by Wilfried et al., 8 in which it was observed that as LVMI increases, LVGLS decreases (r = 0.6, P < .001).
This study showed that as the AVA decreases, the impairment in GLS increases. This agrees with another study by Miyazaki et al. 9 (r = 0.211, P = .025). Another study by Jurin et al. 10 showed an inverse relation of GLS with AVA (R2 = 0.12, P = .026). Another finding of this study is a positive correlation between mean PG and impairment in global longitudinal strain. As the PG across the aortic valve increases, the impairment in GLS also increases. Recently, another trial by Sevilla et al. 11 demonstrated a lower incidence of mortality and cardiovascular or all-cause death in patients with very severe AS who had early AVR compared to patients who received conservative care (Table 5).
Brain natriuretic peptide is an endogenous hormone, secreted mainly from the left ventricle in response to increased wall stress. In patients with aortic stenosis, plasma brain natriuretic peptide (BNP) levels have been demonstrated to be highly correlated with left ventricular end-systolic wall stress and reflect the onset of symptoms. 12
This study demonstrates that as the impairment of global longitudinal strain increases, NT pro-BNP also increases. This observation was similar to another study by Goodman et al. 13 in which also a positive correlation was observed between impairment of global longitudinal strain and level of NT pro-BNP (r = −0.62, P = .0004). Similarly, Bottaro et al. 14 demonstrated a positive correlation (r = 0.43) between impairment in LVGLS and NT pro-BNP and hence prove that LVGLS can be used as a reliable marker in assessing myocardial damage.
Conclusion
This study concludes that left ventricular global longitudinal strain is significantly impaired in patients with asymptomatic severe aortic stenosis even though they had normal ejection fraction. NT pro-BNP was significantly higher in aortic stenosis patients even though they were asymptomatic when compared with normal controls. There was a positive correlation between impairment in LVGLS and elevation of NT pro-BNP. Hence, it can be concluded that LVGLS can be used as a reliable indicator in detecting subclinical impairments in left ventricular function and early interventions in those with severe aortic stenosis who are free of symptoms.
Limitations
The limitations of the study are given below:
The sample size of this study was low. It was a cross-sectional study, and there was no follow-up. In this study, patients were not taken for coronary angiograms to exclude those with CAD. The study period was also short.
Footnotes
Declaration of Conflicting Interests
The author declares no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethical Approval
The ethical committee reference number was 03/04/2021/MCT.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent was obtained from all study participants.