
Abstract
Carotid sinus hypersensitivity is a rare cause of syncope. A 66 year old male patient, presented with an episode of syncope and after evaluation it was diagnosed as carotid sinus hypersensitivity and was treated with dual chamber pacemaker. In the presence of risk factors, carotid sinus hypersensitivity as a diagnosis is considered very rare.
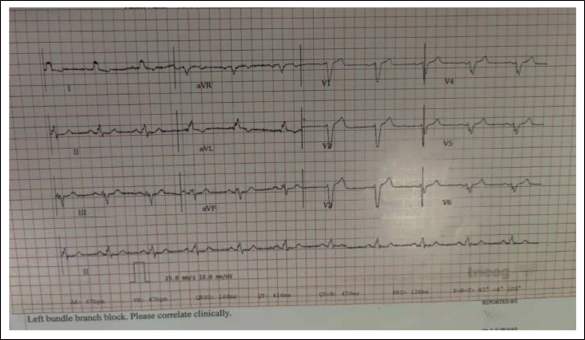
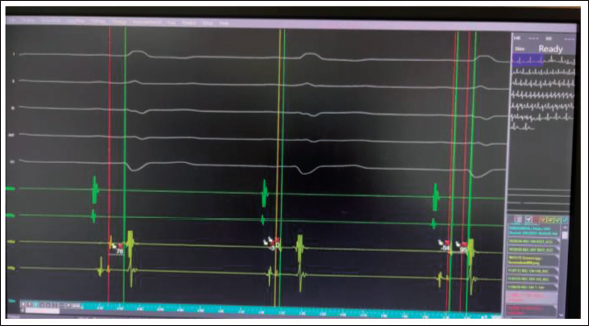
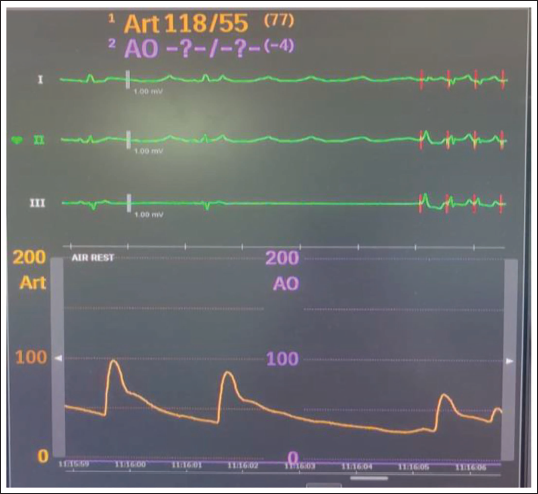
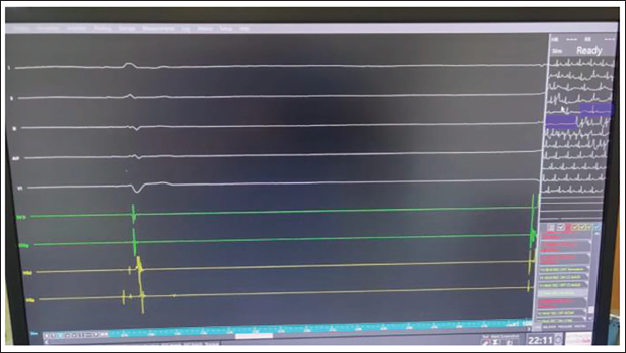
A 66-year-old male patient, presented with an episode of syncope. He experienced a brief episode of loss of consciousness while parking the car; he hit the wall. There was associated trauma on the forehead. He was non-hypertensive, non-diabetic, a non-smoker, and had no past medical illnesses. He lived an active lifestyle with regular exercise and no history of effort intolerance. The patient had experienced a similar episode of syncope 1 month ago while walking and reading a book. He suddenly fell down and regained consciousness within a minute. Both episodes were not associated with tonic-clonic movements, tongue bites, or urinary incontinence. His routine biochemistry was unremarkable. Initially presented to a neurologist, a full workup including an MRI of the brain, Carotid Doppler, and EEG was done and was normal. An ECG showed sinus rhythm, LBBB morphology, QRSD 148 ms, PR interval 126 ms (Figure 1). 2D echo showed a normal ejection fraction of 60% with no regional wall motion abnormality. The patient was put on a 7-day external loop recorder, which showed no episodes of bradycardia, pauses, or tachycardia. Furthermore, he was evaluated with a head-up tilt table test, which was negative. A coronary angiogram and diagnostic electrophysiology study were performed after obtaining written informed consent. The coronary angiogram revealed normal epicardial coronary arteries. The electrophysiology study showed an AH interval of 76 msec, prolonged HV interval of -75 msec (consistent with LBBB). 1:1 AV conduction was observed up to 280ms, after which an AV block at the AV nodal level occurred (Figure 2). CSNRT was assessed at two cycle lengths and was found to be normal. With atrial extra stimuli, there was no HV prolongation or block. No inducible arrhythmias were detected, except for transient, hemodynamically stable, self-terminating atrial fibrillation with atrial double extra stimuli. Right carotid massage showed >3 seconds pause with a drop in systolic pressure from 100 mmHg to 20 mmHg (Figures 3 and 4). At this point, RV pacing was initiated. Left carotid massage did not show any pause. He was diagnosed as having hypersensitive carotid sinus syndrome with mild infra-Hisian disease conduction. A dual-chamber pacemaker DDDR (Attesta Medtronic) was implanted.
ECG demonstrating sinus rhythm with LBBB morphology with normal PR interval.
Electrophysiology tracing demonstrated HV interval-76 msec.
Central monitor showing hypotension (Bp-60/30 mmHg) and pause.
Electrophysiology tracing during carotid massage demonstrating sinus pause of >3 seconds.
Discussion
Syncope is a common clinical condition. Hypersensitive carotid sinus syndrome is rare. On the other hand, prevalence increases with age. It is 2.4% in the sixth decade and increases to 9.1% in the seventh, reaching 40% in people above the age of 80 years. It is diagnosed by reproduction of clinical syncope during carotid sinus massage. Hypersensitive carotid sinus syndrome can manifest in three forms: with a cardioinhibitory response if asystole is longer than 3 seconds or AV block occurs, or a vasodepressor response if there is a drop of more than 50 mm Hg in systolic BP, or mixed cardioinhibitory and vasodepressor response.¹ In our institute we perform carotid massage along with EPS, both for logistic convenience and safety as backup pacing is available in the presence of a long pause. Though rare, it should be considered in the differential diagnosis of patients presenting with syncope, particularly in old age. The diagnosis of hypersensitive carotid sinus syndrome should be approached cautiously after excluding alternative causes of the syncope. Once diagnosed, dual-chamber pacemaker implantation with rate drop response is recommended for a patient with recurrent syncope or falls resulting from hypersensitive carotid sinus syndrome that is cardioinhibitory or mixed (class 2A/IIa, level of evidence B-R).1–3
Footnotes
Abbreviations
AH interval: Interval between onset of atrial signal to the onset of His bundle signal
AV conduction: Atriovenous conduction
CSNRT: Corrected sinus node recovery time
DDDR: Dual-chamber rate modulated pacemaker
EEG: Electroencephalogram
ECG: Electrocardiogram
EPS: Electrophysiology study
HV interval: Interval between onset of His deflection to the onset of QRS
LBBB: Left bundle branch block
MRI: Magnetic Resonance Imaging
QRSD: QRS duration
RV: Right ventricle
Acknowledgement
The authors thank the technical staff of Electrophysiology-lab KIMS especially Bhaswanth Chaitanya O for his immense support during the EP study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Informed Consent
Informed written consent was obtained from the patient about publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.