
Abstract
Pericardial disorders in connective tissue diseases (CTD) are common and may present as acute or chronic pericarditis. Their presentation as cardiac tamponade is rare. The availability of echocardiography has enhanced the ability to make a early diagnosis of pericardial effusion and tamponade. We report a case of mixed connective tissue disease (MCTD) manifesting as cardiac tamponade at presentation and review of the literature.
Keywords
Introduction
Mixed connective tissue disease (MCTD) is an unusual systemic autoimmune disease characterized immunologically by high-titer autoantibodies against the U1 ribonucleoprotein (RNP) and the U1 small nuclear RNP auto-antigen. Clinically, it has overlapping features of systemic lupus erythematosus (SLE), cutaneous systemic sclerosis, rheumatoid arthritis, polymyositis (PM), and dermatomyositis (DM). MCTD can manifest with any of the clinical manifestations of the connective tissue disease (CTD), predominantly rheumatoid arthritis, SLE, or DM.
MCTD involves multiple body organs, including joints, skin mucosa, blood vessels, muscles, lungs, the heart, and the digestive system. Pericarditis is the most common cardiac involvement seen in 10%-20% of patients; however, the presence of effusion is rare. Cardiac disease, as the initial manifestation of the disorder, is rare. We report a case of MCTD manifesting as cardiac tamponade:
Case
A 32-year-old female presented to Medicine department with exertional dyspnea lasting 2 weeks and a fever lasting 3 days. She has been taking thyroid supplement (50 microgram per day) for her hypothyroidism. Before the presentation, she had a history of fatigue, proximal extremities myalgia, and polyarthralgia involving the interphalangeal joints, wrist joints, elbow joints and knee joints. She consulted a local doctor for the above complaints, and she had relief from the analgesics prescribed by the doctor.
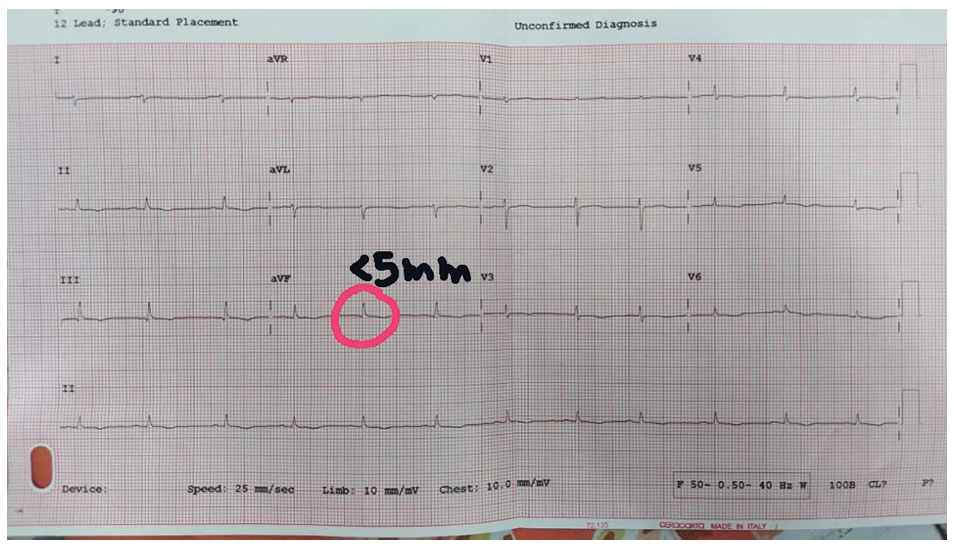
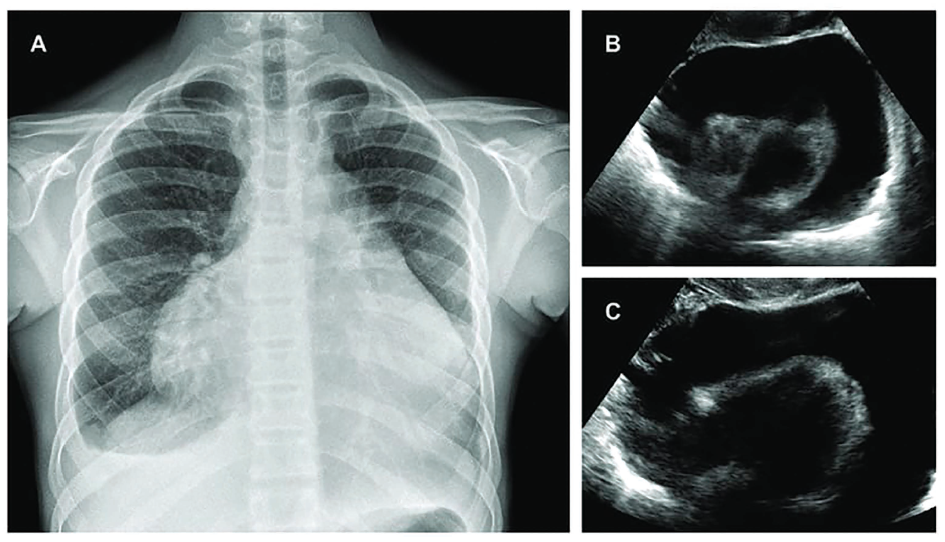
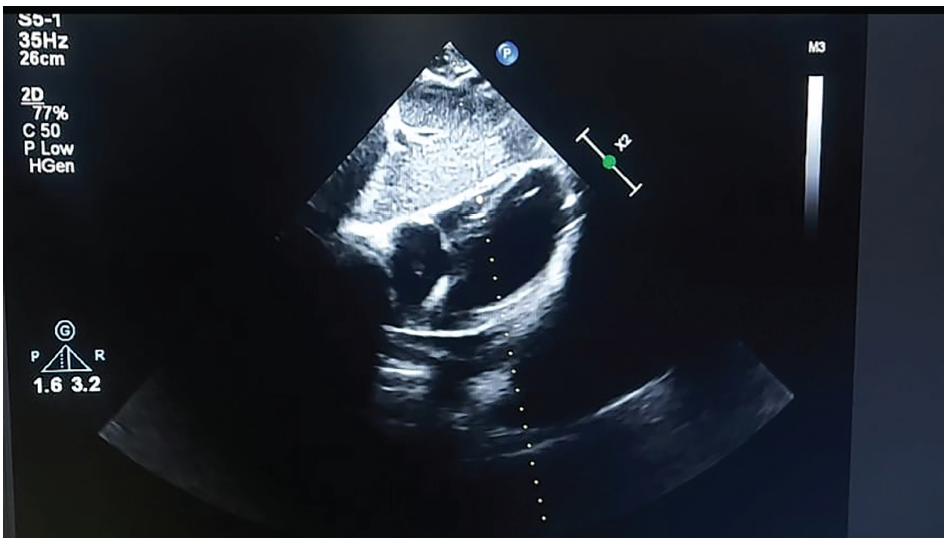
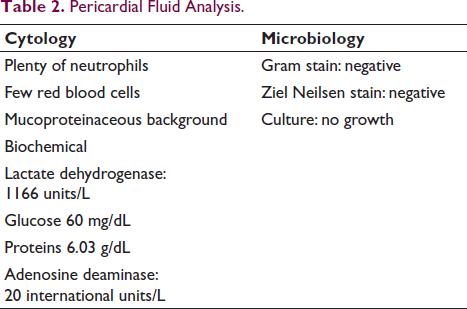
On admission, her blood pressure was 100/80 mm Hg, and her temperature was 37.2°C. Physical examination of the patient showed malar rash and boutenniere deformity (Figure 1). The power of muscles was graded 4/5 in both upper limbs and normal in both lower limbs. The electrocardiogram showed sinus rhythm, low-voltage QRS complexes, and poor R-wave progression (Figure 2). A chest X ray done showed massive cardiomegaly with clear lung fields (Figure 3). In view of cardiomegaly, cardiology consultation was made. Over the next hours of admission, she became tachypneic and hypotensive (90/60 mm Hg), her heart rate was 40 beats per minute with a raised jugular venous pulse. Pulsus paradoxus of 12 mm Hg was recorded on sphygmomanometer. Her heart sounds were distant on auscultation. A bedside 2D echocardiography showed massive pericardial effusion with a swinging heart sign (Figure 3). A diagnosis of cardiac tamponade was made, and emergency pericardiocentesis was done. The patient improved hemodynamically following the procedure and review echo showed no pericardial effusion (Figure 4). The fluid was sent for routine and specific investigations (adenosine deaminase levels, lactate dehydrogenase, and triglyceride levels). The lab profile of the patient and pericardial fluid analysis are shown in Tables 1 and 2.
(A) The Patient’s Face Shows a Malar Rash and a Depressed Nasal Bridge with a Broad Mandible. (B) Fexion of the Proximal Interphalangeal Joint with Hyperextension of the Distal Interphalangeal Joint (Boutonniere deformity)*Consent Given by the Patient.

(A). Chest X-ray PA View Showing Massive Cardiomegaly (Water Bottle Sign) with Pencil Borders Suggesting Pericardial Effusion. (B and C). 2D Echocardiography Subcostal View Showing Massive Pericardial Effusion with “swinging heart” Sign.
Echocardiography Subcostal View Showing Successful Pericardiocentesis.
Laboratory Profile of the Patient (Biochemical and Connective Tissue Disease Profile).
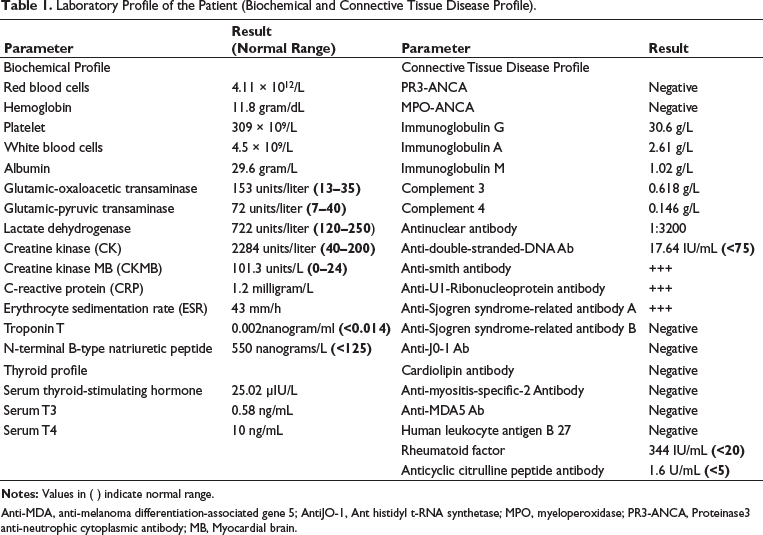
Anti-MDA, anti-melanoma differentiation-associated gene 5; AntiJO-1, Ant histidyl t-RNA synthetase; MPO, myeloperoxidase; PR3-ANCA, Proteinase3 anti-neutrophic cytoplasmic antibody; MB, Myocardial brain.
Pericardial Fluid Analysis.
After the blood profile showed positive antibodies, a diagnosis of MCTD was made. She was started on colchicine 0.5 mg tab once daily. Methylprednisolone 20 mg/day. Within a week of initiation of the medicines, she had improved. Blood investigations were sent to assess the response. However, there was no change in the markers (CK, CKMB, CRP, and ESR). Disease-modifying drugs were added. Tab. mycophenolate mofetil (500 mg/day) was initiated, and intravenous (IV) methylprednisolone (40 mg/day) was given for a week. Following this, there was no change in the markers. The dose was escalated to 750 mg/day of mycophenolate mofetil and 60 mg/day of IV methylprednisolone. The markers declined after a week of therapy. She was kept on maintenance dose of prednisolone and other supplemental medication. She is under regular follow up and there was no recurrence of symptoms there after.
Discussion
Almost every condition that affects the pericardium has the potential to result in an effusion. Tuberculosis continues to be a significant factor in the underdeveloped world. Idiopathic pericarditis, malignancy, and percutaneous procedure complications are the primary causes of substantial effusions in the industrialized world.
Autoimmune diseases such as SLE, rheumatoid arthritis, scleroderma, sarcoidosis, and inflammatory bowel disease can result in pericarditis and effusion. Up to 8%-10% of individuals diagnosed with acute pericarditis may exhibit symptoms of an autoimmune disorder. SLE is responsible for the most significant number of cases, with pericarditis seldom being the initial presentation of the condition. Pericardial involvement often correlates with the activity of the underlying illness. There may be concurrent myocarditis. CP is an infrequent condition, but it is most prevalent among those with rheumatoid arthritis. 1 The management of pericardial involvement focuses on effectively treating the primary illness and is most effectively achieved through close collaboration among cardiologists, rheumatologists, and clinical immunologists.
The patient displayed typical clinical features of cardiac tamponade along with features of MCTD. Pericardial involvement is the most common cardiac manifestation in patients with CTD as well as MCTD. 2 The incidence of pericardial involvement is as follows: 58%-60% in scleroderma, 43%-44% in SLE, 29% in MCTD, 22%-23% in rheumatoid arthritis, and 10% in PM/DM. 3 According to Oetgen et al., 25% of patients diagnosed with MCTD had signs of pericarditis based on their medical history, physical examination, or noninvasive cardiac test. 4 Alpert et al. observed that 30% of participants in their echocardiography study exhibited pericardial involvement. In their study, Singsen et al. found that 42% of children had pericardial abnormalities. 5 Pericardial involvement was observed in 55% of postmortem cases diagnosed with MCTD. In patients with MCTD, pericardial involvement is primarily asymptomatic, with just 8%–12% of affected individuals experiencing symptoms. Asymptomatic pericardial effusion is detected in approximately 1/3rd of patients on echocardiography.
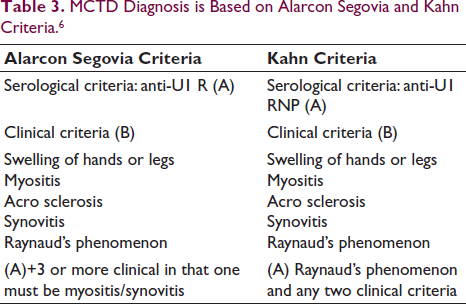
In our case, MCTD was diagnosed by Alarcón-Segovia and Kahn criteria (Table 3).
MCTD Diagnosis is Based on Alarcon Segovia and Kahn Criteria. 6
Colchicine, is effective when given alongside the conventional treatment for recurrent pericarditis and also prevents recurrences when the conventional treatment is ineffective. 7 Patients with acute, apparently idiopathic pericarditis with no more than mild tamponade can be treated for a brief period of time under careful monitoring with an NSAID and/or a corticosteroid combined with colchicine in an attempt to rapidly shrink the effusion. Patients with known inflammatory/autoimmune diseases can be treated similarly (there is no evidence that corticosteroids increase recurrences in these patients).
Immunosuppressive therapy is an alternative treatment choice. The research examined the clinical outcome of individuals with recurrent pericarditis treated with either azathioprine or mycophenolate mofetil. 8 The authors propose the use of immunosuppressive medication for individuals who do not show a response to large doses of steroids, pericardial window (pericardiotomy) and pericardiectomy are performed in patients who do not respond to the medical management. 9 MCTD can cause various pericardial diseases, ranging from acute pericarditis to cardiac tamponade. This case highlights the consideration of probability of cardiac tamponade in MCTD patient presenting with dyspnea and hemodynamic instability.
Conclusion
Pericardial disease can occur in various CTDs and may be fatal.
They go undetected clinically and are may not found until autopsy. MCTD presenting with cardiac tamponade is rare and is being presented, which responded well to pericardiocentesis and medical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Institutional Ethical Committee Approval not applicable here as it is a case report. Informed consent has been taken from the patient regarding the publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.