
Abstract
This expert opinion addresses the prevalence of cardiovascular diseases (CVDs) among Indian women, suggesting strategies for screening and risk assessment. A panel of expert cardiologists (n = 99) developed a questionnaire for screening CVD and risk stratification, analyzing discussion points and opinions to formulate recommendations. Experts strongly agreed that ischemic heart diseases remain underdiagnosed and undertreated among Indian women. Women should be screened for future risk of atherosclerotic CVD at the age of 45–50 years if they have diabetes or other CV risk factors. Experts strongly recommended targeted screening for CVD among women during and post-pregnancy period. Women should be screened for peripartum cardiomyopathy (PPCM) risks during pregnancy and post-delivery, with dyspnea, edema, and tachycardia being the most common red flags in the diagnosis of PPCM among Indian women. This expert opinion report provides a comprehensive overview of expert cardiologists’ recommendations for screening heart diseases and risk stratification in Indian women.
Introduction
Cardiovascular diseases (CVDs) are the predominant cause of mortality and disability in India, 1 with 27.4% (25.3%–29.2%) of total deaths and 13.9% (12.2%–15.6%) of total disability-adjusted life years (DALYs) in the year 2019. 2 The latest findings from the Global Burden of Diseases (GBD) 2019 report reveal a drastic increase in CVD-related fatalities among women in India, surpassing the numbers for men and hence, CVD has now emerged as the leading cause of death among Indian women. 2 The proportion of total DALYs for CVD among females has increased from 5.4% in 1990 to 12.1% in 2019. 2 Despite the increasing disease burden and associated morbidity and mortality, CVDs among women are often under-recognized, underdiagnosed, and eventually undertreated. 3 Furthermore, women remain significantly underrepresented in cardiovascular clinical research as compared to men. 4 This results in limited understanding of impact of CVD and the broad implications of various treatment modalities on women’s health.
In India, the underdiagnosis and undertreatment of CVD among women can be attributed to a complex interplay of various social, cultural, economic, and healthcare-related factors. Due to the lack of gender-specific data, coronary heart disease is long-established as a disease of men. 5 Women typically present with heart disease 10 years older than men, a pattern often observed during the postmenopausal stage when the protective advantages of estrogen diminish.5, 6 The lack of knowledge and awareness about CVDs and their symptoms results in delayed diagnosis and treatment among women in India. Women often present with atypical symptoms of CVD compared to men. Women might experience symptoms such as fatigue, abdominal discomfort, nausea, and back pain, which could be misattributed to other conditions by healthcare professionals (HCPs). 6 Additionally, there exists uncertainty among HCPs about the ideal age for screening of heart disease in women. It is, therefore, essential to emphasize the need for targeted screening among women in India to identify risk factors at early stages and mitigate potential complications of CVD. This necessitates adopting a standardized approach with the ultimate goal of eliminating the underestimation of CVD diagnosis, reducing healthcare disparities, and improving outcomes and overall cardiovascular health in Indian women.
Considering this background, the present document about screening of heart disease and risk stratification in Indian women was developed. This expert opinion particularly focused on providing insights into early screening and diagnosis of women with ischemic heart disease/acute coronary syndrome (IHD/ACS), pregnancy and hypertension, and heart failure and peripartum cardiomyopathy (PPCM) in Indian women.
Materials and Methods
A questionnaire pertaining to screening of CVD and risk stratification among Indian women was drafted and finalized by an expert panel of cardiologists. The questionnaire included 14 questions regarding the early screening and diagnosis of IHD (ACS), pregnancy and hypertension, and heart failure and PPCM. The approved questionnaire was further discussed to seek opinions of experts in seven regional-level advisory board meetings held across India from 11 May 2023 to 21 July 2023. Each advisory board meeting was moderated by a leading expert cardiologist and attended by approximately 99 regional expert cardiologists. The expert opinions were supported by scientific evidence, their own experiences, and their collective clinical judgment. Discussions from all the meetings were compiled and analyzed to prepare this expert opinion.
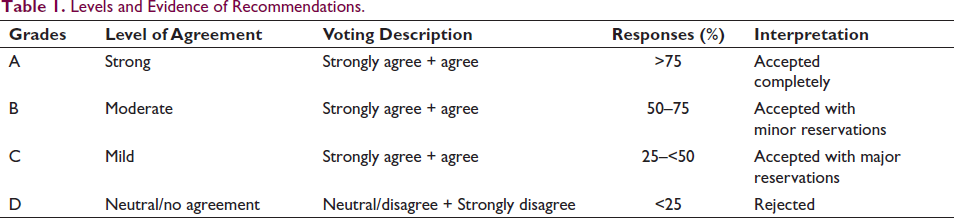
The expert opinions were analyzed in two different ways. The agreement/disagreement responses were graded into four grades: Level A as strong level of agreement (if >75% of responses, then experts accepted completely), Level B as moderate level of agreement (if 50%–75% of responses, then experts accepted with minor reservations), Level C as mild level of agreement (if 25–<50% of responses, then experts accepted with major reservations) and Level D as neutral/no agreement (≤25%) (Table 1). The remaining questions were multiple choice questions and responses for these were presented directly as numbers and percentages.
The in-depth discussion points and opinions of the experts were used to formulate a set of opinion-based recommendations for screening of CVD and risk stratification among Indian women.
Levels and Evidence of Recommendations.
Results
A total of 99 cardiologists from seven regions across India were convened in the advisory board meetings for the development of this expert opinion.
Ischemic Heart Disease (Acute Coronary Syndrome [ACS])
Diagnostic Challenges of IHD
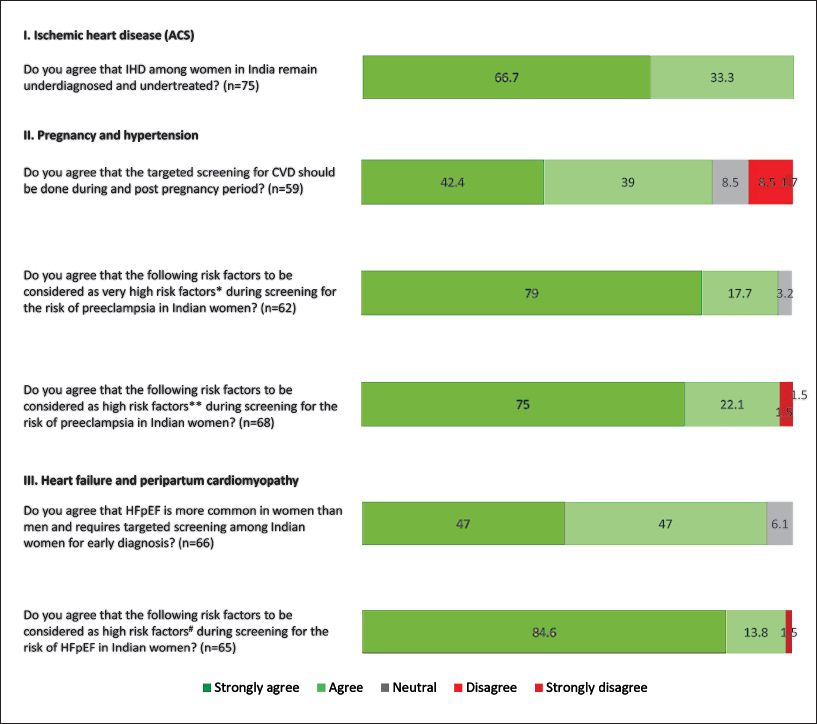
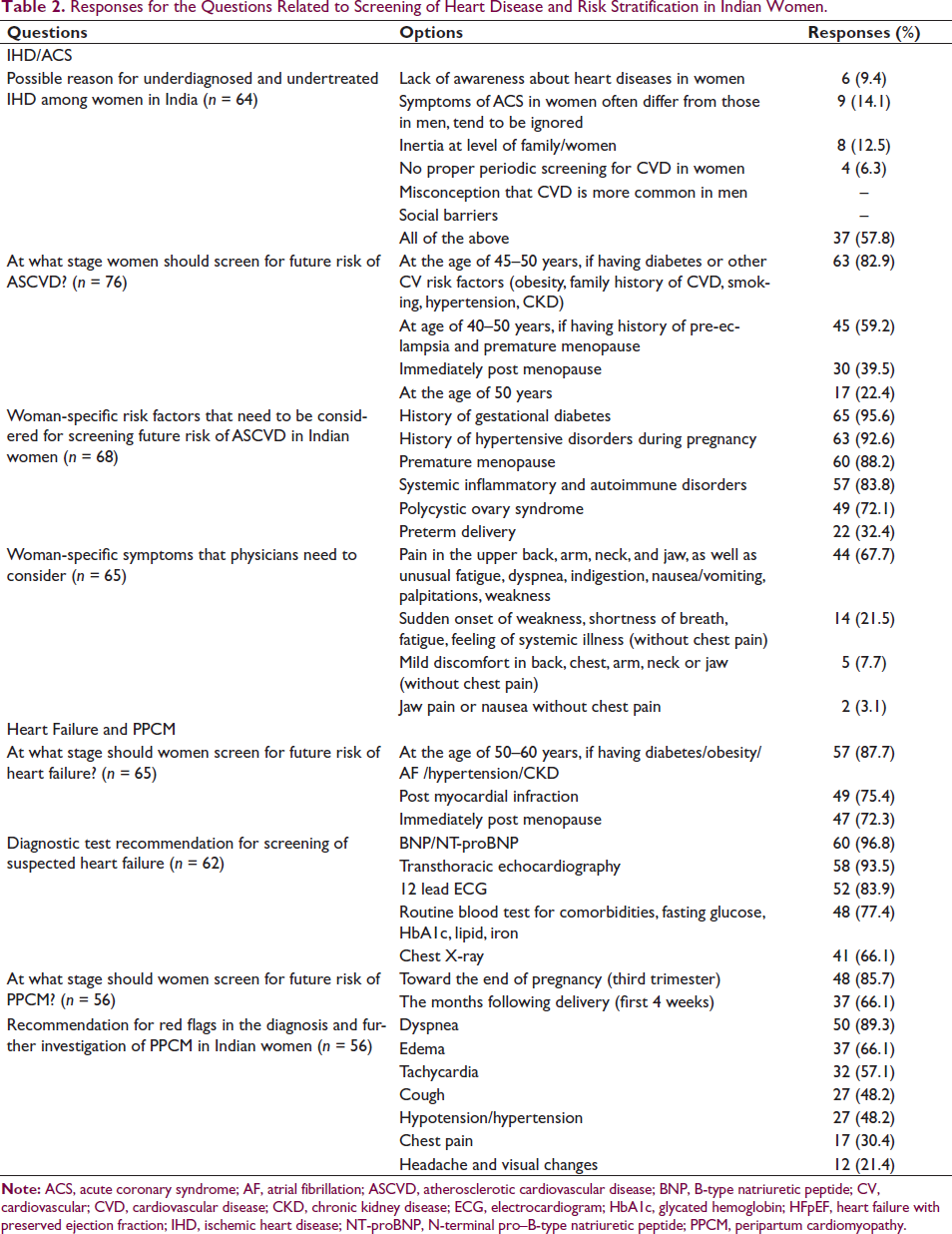
There was a strong level of agreement (Level A; strongly agreed/agreed: 100%) that IHD remains underdiagnosed and undertreated among women in India (Figure 1). Overall, 57.8% of experts (37/64) opined that lack of awareness about heart diseases in women, symptoms of ACS in women often differ from those in men and tend to be ignored, inertia at the family level or by the woman herself, no proper periodic screening for CVD in women, the misconception that CVD is more common in men are collectively, the possible reasons for underdiagnosed and undertreated IHD among Indian women (Table 2).
Responses for the Questions Related to Screening of Heart Disease and Risk Stratification in Indian Women.
Screening of IHD
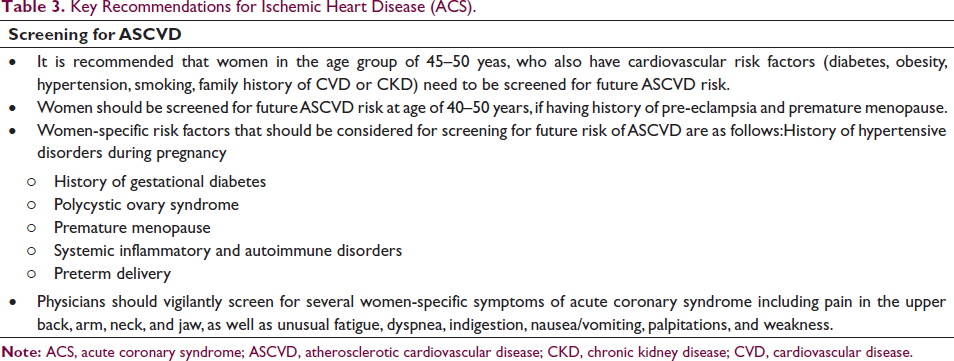
A majority of experts (82.9%) believed that women should be screened for future risk of atherosclerotic cardiovascular disease (ASCVD) at the age of 45–50 years, if having diabetes or other CV risk factors (obesity, family history of CVD, smoking, hypertension, chronic kidney disease [CKD]). According to the experts, the women-specific risk factors that need to be considered for screening future risk of ASCVD in Indian women include history of gestational diabetes (95.6%), history of hypertensive disorders during pregnancy (92.6%), premature menopause (88.2%), systemic inflammatory and autoimmune disorders (83.8%), polycystic ovary syndrome (PCOS) (72.1%), and preterm delivery (32.4%).
Women-specific Symptoms of IHD
A total of 67.7% of experts opined that women-specific symptoms that physicians need to consider are pain in the upper back, arm, neck, and jaw, as well as unusual fatigue, dyspnea, indigestion, nausea/vomiting, palpitations, weakness (Table 2). Key recommendations regarding screening for ASCVD in women are summarized in Table 3.
Key Recommendations for Ischemic Heart Disease (ACS).
Pregnancy and Hypertension
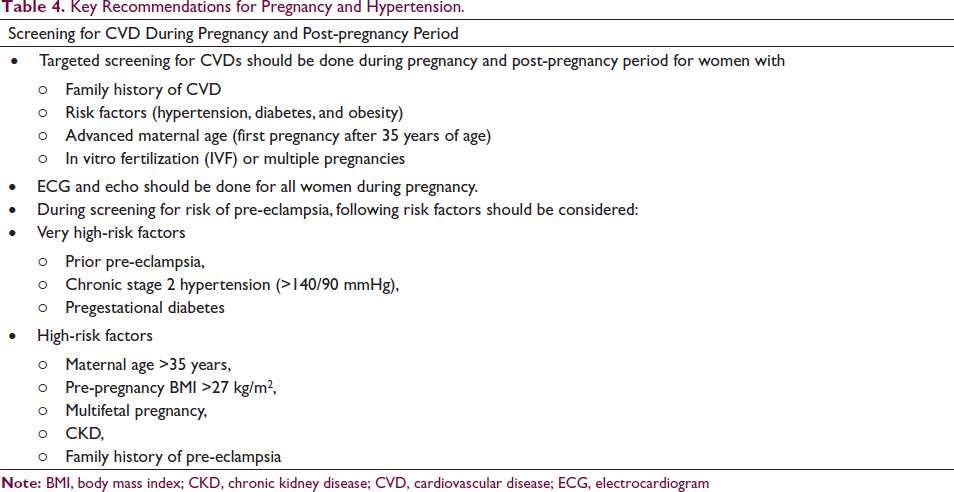
Experts strongly agreed that the targeted screening for CVD should be done during and post-pregnancy period (Level A; 48/59, 81.4%). There was a strong level of agreement that prior pre-eclampsia, chronic stage 2 hypertension (>140/90 mmHg), and pregestational diabetes to be considered as very high-risk factors during screening for the risk of pre-eclampsia in Indian women (Level A; 60/62, 96.7%). A strong level of agreement was obtained for several factors (including maternal age >35 years, pre-pregnancy body mass index [BMI] >27 kg/m2, multifetal pregnancy, CKDs, family history of pre-eclampsia) to be considered as high-risk factors during screening for the risk of pre-eclampsia in Indian women (Level A; 66/68, 97.1%; Figure 1). Table 4 summarizes the key recommendations provided by the cardiologists on screening for CVD during pregnancy and post-pregnancy period.
Key Recommendations for Pregnancy and Hypertension.
Heart Failure and Peripartum Cardiomyopathy
HFpEF in Women
Experts strongly agreed that heart failure with preserved ejection fraction (HFpEF) is more common in women than men and requires targeted screening for early diagnosis among Indian women (Level A; 62/66, 94.0%). Experts strongly believed that high BMI/obesity, diabetes, hypertension, atrial fibrillation, CKD to be considered as high-risk factors during screening for the risk of HFpEF in Indian women (Level A; 64/65, 98.4; Figure 1).
Screening of Heart Failure
Experts recommended that women should screen for future risk of heart failure at the age of 50–60 years, if having diabetes/obesity/atrial fibrillation/hypertension/CKD (87.7%), post myocardial infarction (75.4%), and immediately post menopause (72.3%). The diagnostic tests recommended by the experts for screening suspected heart failure include B-type natriuretic peptide/N-terminal pro–B-type natriuretic peptide (BNP/NT-proBNP, 96.8%), transthoracic echocardiography (93.5%), 12 lead electrocardiogram (ECG, 83.9%), routine blood test for comorbidities, fasting glucose, glycated hemoglobin (HbA1c), lipid, iron (77.4%), and chest X-ray (66.1%).
Peripartum Cardiomyopathy
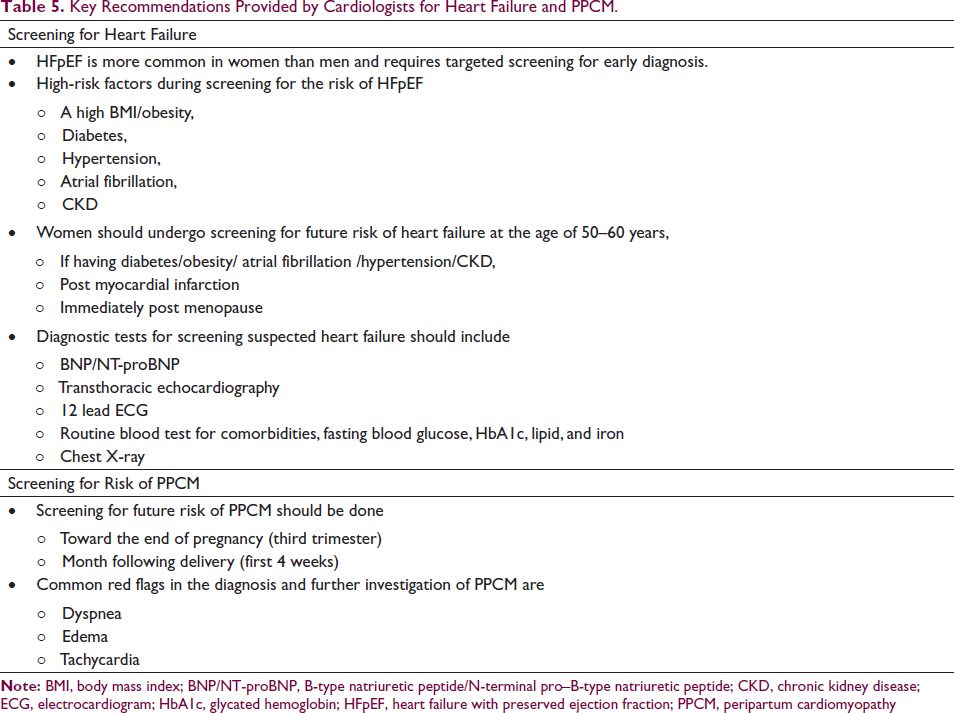
Experts recommended that women should screen for future risk of PPCM toward the end of pregnancy (third trimester) (85.7%) and the months following delivery (first 4 weeks) (66.1%). According to the experts, dyspnea (89.3%), edema (66.1%), and tachycardia (57.1%) are the most common red flags in the diagnosis and further investigation of PPCM in Indian women (Table 2). Key recommendations provided by cardiologists for heart failure and PPCM are summarized in Table 5.
Key Recommendations Provided by Cardiologists for Heart Failure and PPCM.
Discussion
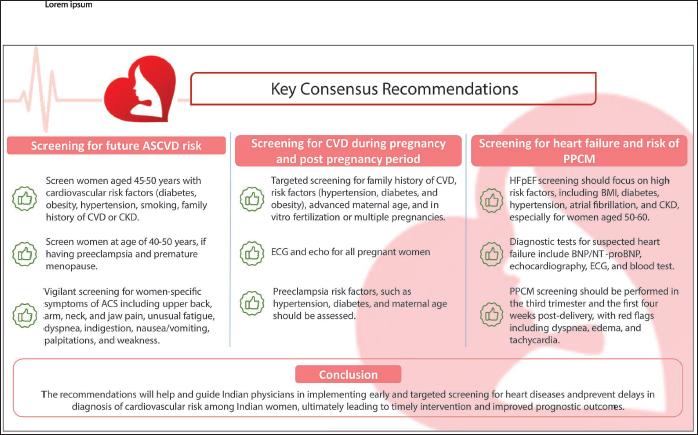
Till date there has been no expert opinion focused on the screening of CVDs in Indian women and this is the first expert opinion report from India that comprehensively discusses opinion-based insights and recommendations with respect to the screening of heart disease and risk stratification in Indian women throughout their life (Figure 2).
Summary of the Expert Opinion
Early Screening and Diagnosis of IHD
All the experts agreed that IHD continue to be both underdiagnosed and undertreated in the female population of India. They posit that several factors contribute to the underdiagnosis and undertreatment of IHD. These factors encompass limited awareness of heart diseases in women, disparities in the presentation of ACS symptoms compared to men, familial or personal complacency, the absence of routine CVD screenings for women, and the misconception that CVD primarily afflicts men. The available data corroborate with the statement that women with IHD are underdiagnosed and undertreated compared to the male counterparts across the world.5, 7 The inclusion of women in major Indian ACS registries, typically ranging between 16% and 29%,8–11 underscores the persistently low representation of women in such studies. This further reinforces the agreement that women continue to be underdiagnosed and undertreated for heart diseases in India.
Experts also emphasized that women tend to have worse outcomes and prognosis for coronary artery disease (CAD). They often present with atypical symptoms of IHD, making diagnosis challenging. Additionally, delay in seeking medical treatment is common among women with IHD. Socioeconomic factors and atypical symptom presentation contribute to underdiagnosis and undertreatment. Women have low awareness and undergo less screening for IHD compared to men. Experts also mentioned that the medical fraternity occasionally contributes to the underdiagnosis and undertreatment of IHD in women when women’s symptoms of IHD are occasionally belittled or dismissed by healthcare professionals, leading to incomplete investigations. Delays at various stages of care can lead to increased morbidity and mortality among women with IHD. The observations from the recent study (North India ST-Elevation Myocardial Infarction registry [NORIN-STEMI]) 10 corroborate with the expert opinions in this document. Mortality outcomes such as in-patient mortality, 30-day mortality and 1-year mortality were significantly higher in women compared to men. One of the experts also suggested that raising awareness among women, especially in rural areas, is crucial for regular risk factor monitoring and prevention of IHD. A review by Shivam S, et al. has discussed the factors contributing the underdiagnosis of heart disease in women and these included the cultural stigma surrounding women openly discussing their health issues, which is further exacerbated by challenges such as limited access to medical care, lower socioeconomic status, and reduced educational attainment. 12
The prevailing agreement among a majority of experts was that women should undergo screening for future risk of ASCVD around the ages of 45–50 years, especially if they have diabetes or other cardiovascular risk factors such as obesity, a family history of CVD, smoking habits, hypertension, or CKD. On the other hand, more than half of the experts also believed that women should be screened for future ASCVD risk at age of 40–50 years, if having history of pre-eclampsia and premature menopause. Experts also opined that women are at reduced CVD risk, with estrogen providing protective benefits. Furthermore, they highlighted that few physicians may wrongly assume that women under the age of 40–45 are protected by estrogen levels. Women who experience premature menopause face an increased risk of CAD, similar to that of younger men. Besides the age factor, consumption of oral contraceptive pills, those having diabetes, hypertension, hypercholesterolemia, stressful lifestyle, PCOS contribute to the risk of ASCVD. Most of the problems associated with menopause are encountered much earlier when the woman has PCOS, requiring an early investigation. Women receiving radiotherapy or chemotherapy, those who smoke, and those with autoimmune diseases also require thorough CV risk check-up. Experts also recommended that females over the age of 35 should undergo regular health check-ups, and those with a genetic or familial history should have their health checked even earlier. There are incidences of multivessel disease, calcified disease among women aged 40–50 years, which was never the case before a decade. Experts also suggested that certain risk factors like the use of hormonal pills and ovulation induction drugs also play a significant role in CVD; these factors are under-studied and should also be included in the risk analysis of women. Screening in women with early menopause and pre-eclampsia is also necessary because the protective effect of estrogen in these patients might be weak. Therefore, women with a history of higher risk factors should undergo screening by the age of 40 years. The attributable factors reported for the substantially high mortality rates among women in NORIN-STEMI registry were older age at presentation, high prevalence of diabetes and hypertension in women, delays in seeking healthcare, and low rates of invasive strategies. 10
Experts provided a strong level of agreement that history of hypertensive disorders during pregnancy, history of gestational diabetes, PCOS, premature menopause, and systemic inflammatory and autoimmune disorders are all women-specific risk factors that need to be considered for screening for future risk of ASCVD in Indian women. In the 2019 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines, early menopause and pre-eclampsia were described as two specific risk factors unique to women that increase the risk of CVD. 13 Furthermore, various other risk factors specific to women, such as early onset of menstruation, PCOS, multiple pregnancies, adverse pregnancy outcomes, and hormone therapy, also play a role in impacting a woman’s risk of CVD across her life. 14 Premature menopause is a strong driver for early heart failure and atrial fibrillation. Data suggests that premature menopause is associated with 33% increased risk of early heart failure and 9% increased risk of atrial fibrillation.15, 16 In addition, preterm delivery is also a risk factor of CVD that needs to be emphasized while screening ASCVD risk in women. This indication is in concordance with the observations of previous systematic review and meta-analysis wherein preterm delivery has been linked to a rise in future adverse cardiovascular outcomes for mothers, notably a two-fold increase in mortality attributable to coronary heart disease. 17 Evidence from a longitudinal cohort study (n = 70,182) indicates that preterm delivery was associated with a 42% increased risk of developing CVD in comparison to women who had a full-term delivery (≥37 weeks) during their first pregnancy. 18
Majority of experts suggested that physicians need to look carefully for several women-specific symptoms of ACS including pain in the upper back, arm, neck, and jaw, as well as unusual fatigue, dyspnea, indigestion, nausea/vomiting, palpitations, weakness. They further emphasized that jaw pain is an important characteristic of angina or CAD and dyspnea is more common presentation of CVD than chest pain especially in women. A high index of suspicion is required in women exhibiting the above-mentioned symptoms who often ignore or attribute these symptoms to other systemic disorders.
Hypertension and Pregnancy
During pregnancy and the postpartum period, there exists a chance to recognize risk factors in women, enabling them to enhance their long-term well-being. Adverse pregnancy outcomes such as gestational hypertension, gestational diabetes, pre-eclampsia, preterm birth, and small for gestational age were associated with a two to fourfold increased risk of composite. 19 Pregnancy exerts distinct demands on the female cardiovascular system, presenting particular diagnostic and treatment complexities when addressing heart conditions during pregnancy. Additionally, it gives rise to novel cardiovascular risk factors associated with gestation. This expert opinion report also gathered viewpoints of experts regarding diagnosis of CVD risk in pregnant women with hypertension.
Experts provided a strong level of agreement that targeted screening for CVDs should be done during pregnancy and post-pregnancy period. Pregnancy can act as a cardiovascular stress test. The development of pregnancy complications such as gestational diabetes, hypertensive disorders of pregnancy, preterm birth, delivery of a neonate with fetal growth restriction, and significant placental abruption can help to identify women at increased risk for CVD. Pregnancy and the postpartum period present an opportunity to detect the underlying, often undiagnosed CV risk factors that increase the risk of future CVD among women. The targeted screening for CVD in at-risk reproductive-ages women might thus, preserve and improve the long-term CV health outcomes in them. 20
Experts believed that targeted screening for CVD becomes a priority because of the atypical symptom presentation in women. Certain parameters such as blood pressure, lipid profile, and glucose levels are often deranged during pregnancy. Experts recommended that women having family history of CVD, those having risk factors (hypertension, diabetes, and obesity), advanced maternal age (first pregnancy after 35 years of age), those having in vitro fertilization or multiple pregnancies should undergo targeted screening for CVD during pregnancy as well as in post-pregnancy period. They further emphasized that ECG and echo should be done for all women during pregnancy.
Pregnancy-related physiological changes can cause signs and symptoms that can be mistaken for CVD. Therefore, it can be challenging to develop a universal CVD risk screening protocol for all women during and postpartum period. However, targeted screening decisions can be made depending on patient-to-patient scenario. Using information provided by patients about their symptoms, along with their vital signs and physical examinations, healthcare professionals can recommend additional CVD assessments, which may include laboratory tests such as BNP and troponin, as well as other diagnostic procedures like ECG, chest X-rays, or stress tests. 21
Experts unanimously were in agreement with the statement that risk factors including prior pre-eclampsia, chronic stage 2 hypertension (>140/90 mmHg), and pregestational diabetes are very high-risk factors during screening for risk of pre-eclampsia in Indian women. They also provided strong level of agreement that risk factors including maternal age >35 years, pre-pregnancy BMI >27 kg/m2, multifetal pregnancy, CKD, and family history of pre-eclampsia should be considered as high-risk factors during screening of preeclampsia in Indian women.
Heart Failure and PPCM
Heart failure is a condition that exhibits some of the most significant sex differences in cardiovascular medicine. Men are more susceptible to develop heart failure with a reduced ejection fraction (HFrEF) than women, while women are at higher risk of developing HFpEF. 22
Experts acknowledged in majority that HFpEF is more common in women than men and requires targeted screening for early diagnosis of HFpEF among Indian women. Experts further explained that comorbidities such as diabetes, hypertension, obesity, and female as a gender are the risk factors of HFpEF. Experts added that HFpEF is more common in the elderly population. The life expectancy of females is comparatively longer than males; one of the possible reasons for the higher incidence of HFpEF among women. These propositions were supported by Scantlebury et al., 23 who reported that risk factors associated with HFpEF are older age, hypertension, obesity and diabetes. However, the most significant difference when comparing HFpEF and HFrEF is the gender disparity, with a typical odds ratio of 2.29, indicating that more women are affected with HFpEF than men. 24 Additionally, experts opined that obstructive sleep apnea (OSA), atrial fibrillation, and CKD are other risk factors of HFpEF. Evidence indicates that HFpEF is associated with obesity, anemia, diabetes, chronic obstructive pulmonary disease, CKD, and transthyretin-related amyloidosis. In addition, OSA may be a significant risk factor for HFpEF. 25 Ariyaratnam et al. discussed that AF and HFpEF often occur together; and they both involve a complex left atrial (LA) disorder that affects its structure, function, and electrical activity. Additionally, AF and HFpEF have numerous overlapping risk factors including obesity, high blood pressure, diabetes, OSA, alcohol use, and smoking.26–29
In light of the above discussion, experts provided strong level of agreement that high BMI/obesity, diabetes, hypertension, atrial fibrillation, and CKD to be considered as high-risk factors during screening for the risk of HFpEF in Indian women. On parallel lines, a review article by Teramoto et al. indicated the correlation between HFpEF and cardiovascular risk factors such as hypertension, diabetes, obesity, and AF, alongside non-cardiovascular conditions such as chronic obstructive pulmonary disease and CKD. 30
Women face an increased likelihood of experiencing concentric left ventricular remodeling and reduced ventricular dilatation in response to arterial hypertension than men. This can potentially lead to diastolic dysfunction, systolic dysfunction, and diminished ventricular reserve during stress. 23 According to the experts, HFpEF is not always an easy diagnosis unless, there is a high index of suspicion. Therefore, experts suggest that paying attention to pulmonary hypertension, diastolic function is important in women for the diagnosis of HFpEF. Chest X-ray, ECG, echo, and NT-proBNP are important investigations for the diagnosis of HFpEF and diastolic dysfunction. The collective consideration of all these factors necessitates targeted screening for early diagnosis of heart failure among Indian women.
Experts recommended that women should screen for future risk of HF at the age of 50–60 years (if having diabetes/obesity/atrial fibrillation/hypertension/CKD), post myocardial infarction, and immediately post menopause. CVD poses a substantial health concern among the elderly, and women aged 50 and older are consistently observed to be more vulnerable to CVD compared to their male counterparts in the same age group. This heightened risk can largely be attributed to the onset of menopause, during which a significant decrease in estrogen levels occurs. This hormonal shift ultimately exerts a more pronounced influence on CVD risk in women compared to men. 31 A strong wall of evidence indicates that women experience a significant surge in the risk of CVD when they reach menopause, with an increase of up to two to four times.31, 32 Myocardial infarction (MI) continues to be the prevailing reason for HF. The development of HF is common following hospitalization for a myocardial infarction (MI) and discharge from the hospital. 33 Sulo et al. reported that HF occurred in 13% of patients within 30 days and in another 32.6% between 30 days and 1 year after MI discharge. Moreover, the occurrence of HF after discharge following an acute MI is most frequent during the initial months and tends to decrease at one year after the index AMI event. 34 Based on this evidence and expert opinions gathered, women should be screened for future risk of HF at the age of 50–60 years (if having diabetes/obesity/atrial fibrillation/hypertension/CKD), post MI, and immediately post menopause.
The diagnostic tests recommended by the experts for screening suspected heart failure include BNP/NT-proBNP, transthoracic echocardiography (TTE), 12 lead ECG, routine blood test for comorbidities, fasting glucose, HbA1c, lipid, iron, and chest X-ray. Experts believe that patients with the reduced ejection fraction can be diagnosed more easily, whereas those with preserved ejection fraction can be overlooked more frequently. Similarly, the 2016 European Society of Cardiology (ESC) heart failure guidelines suggest that it is more difficult to diagnose HFpEF than HFrEF. 35 Due to the significant prevalence of comorbidities that may mimic or accompany HFpEF, as well as the lack of a single objective marker that identifies the disease, diagnosing HFpEF can be difficult. 36 For the diagnosis of HF and cardiac dysfunction, the clinical biomarkers BNP and NT-proBNP are frequently utilized. BNP and NT-proBNP levels may elevate as a result of HF and cardiac dysfunction, which can be caused by IHD, various types of arrhythmia, and cardiomyopathy. 37 However, BNP/NT-proBNP is not feasible and performed in selective patients because of its cost. Moreover, natriuretic peptides are employed to rule out HF but not to make the diagnosis. The elevation of natriuretic peptides can be caused by various cardiovascular and non-cardiovascular reasons, potentially reducing their effectiveness as diagnostic markers for HF. 35
Echocardiography is the most readily available diagnostic test for suspected HF. Transthoracic echocardiography is the preferred method for evaluating the systolic and diastolic function of both the left and right ventricles. 35 However, two-dimensional echocardiography is routinely performed because the availability of TTE might be a problem. Electrocardiogram is the baseline investigation of all cardiovascular examinations. It has a low specificity for the diagnosis of HF but can provide information on myocardial infarction. Heart failure is improbable in patients who exhibit an entirely normal ECG. Thus, ECG is used as a standard procedure to rule out HF. 35 Chest X-ray is of limited value in the diagnosis of suspected HF; however, it may reveal pulmonary venous congestion or edema in a patient with HF. 35 Experts opined that other laboratory assessments include blood investigations for fasting glucose, HbA1c, lipid profile, and iron.
Experts strongly recommended that women should screen for future risk of PPCM toward the end of pregnancy (third trimester) as well as the months following delivery (first 4 weeks). The Heart Failure Association of the ESC defined PPCM as “an idiopathic cardiomyopathy presenting with HF secondary to left ventricular (LV) systolic dysfunction toward the end of pregnancy or in the months following delivery, where no other cause of HF is found”. 38 Experts suggested that any woman with severe breathlessness, raised jugular venous pressure, right internal mammary artery (RIMA) disproportional to the pregnancy or fluid overload, or symptoms of paroxysmal nocturnal dyspnea, whether in the third trimester or postpartum period should be investigated thoroughly to rule out PPCM. Experts also referred for dyspnea, edema, and tachycardia to be the most common red flags in the diagnosis and further investigation of PPCM in Indian women. It has been reported that symptoms of PPCM similar to those of HF including fatigue, shortness of breath, tachycardia, orthopnea, paroxysmal nocturnal dyspnea, fluid retention, elevated jugular venous pressure, bilateral pulmonary crackles due to pulmonary edema, third heart sound (S3) and displaced apical pulse.39–41
Conclusion
A strong agreement emerged regarding the screening of heart diseases and risk stratification in Indian women, with experts emphasizing: (a) underdiagnosis and undertreatment of IHD among Indian women exist, (b) a strong need of targeted screening for CVD during and post-pregnancy period, and (c) need of targeted screening for HFpEF in Indian women and recommendation for considering obesity, diabetes, hypertension, atrial fibrillation, and CKD as high-risk factors during screening for HFpEF risk among Indian women. The recommendations perceived in this expert opinion will help and guide Indian physicians in implementing early and targeted screening for heart diseases and prevent delays in diagnosis of cardiovascular risk among Indian women, ultimately leading to timely intervention and improved prognostic outcomes.
Footnotes
Acknowledgements
The authors thank Rupika Pawar and Dr. Tejal Vedak (Sqarona Medical Communications, Pune) for providing medical writing assistance.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dipak Pawar, Pradip Mate, Lokesh Kumar, Kamlesh Patel are employees of Lupin Limited, Mumbai. All other authors have no conflict of interest to declare.
Ethical Approval and Informed Consent
Not applicable, as this is a review article, and no patients were involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This initiative was funded by Lupin Limited, Mumbai.