
Abstract
Right atrial aneurysm (RAA) is a rare congenital anomaly. It usually occurs due to dysplasia of the atrial myocardium or localized absence of pericardium. We present a case of asymptomatic RAA in an adolescent, which was detected incidentally because of a bulge in the right heart border.
Case Description
A 15-year-old boy was incidentally detected to have a bulge in the right heart border on a chest X-ray at the age of 1½ years. He was diagnosed with a right atrial aneurysm on echocardiographic evaluation after considering the differentials of pericardial cyst, loculated effusion, and cor triatriatum dexter. On follow-up, the skiagram showed an enlargement at the right atrial border (Figure 1A) without any other abnormalities. The cardiovascular examination and electrocardiogram were normal. An anechoic space measuring 49 × 25 mm was detected posterosuperior to the right atrium on an echocardiogram (Figure 1B, C and Supplementary Video 1), but the heart was structurally normal otherwise. However, a cardiac MRI showed a well-defined 38 × 28 × 26 mm outpouching from the lateral wall of the pectinate portion of the right atrium, inferior to the opening of the right atrial appendage (Figure 1D), indicating a right atrial aneurysm. The pericardial layer adjacent to the outpouching was not clear, and absence of filling defects ruled out any thrombus. The patient was kept on medical follow-up because of the asymptomatic status and the small size of the aneurysm. Interval imaging since diagnosis (10-year interval) showed an insignificant increase in size (Figure 1E, F). The patient has been asymptomatic for 15 years without any signs of arrhythmias or thromboembolism. Hence, he was kept on annual medical follow-up.
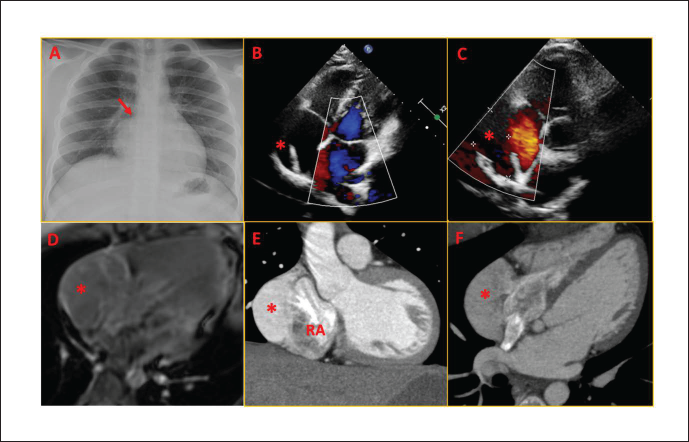
Asterisk (*): right atrial aneurysm.
Right atrial aneurysm (RAA) is a rare anomaly, with less than 50 reported cases worldwide. It has been described as a congenital anomaly due to dysplasia of the atrial myocardium or localized absence of pericardium, with many instances identified prenatally. Long-standing atrial hypertension secondary to pulmonary hypertension or tricuspid valve disease can cause an acquired RAA. Usually asymptomatic, it is diagnosed when evaluated for an incidentally detected cardiomegaly in a chest X-ray. Sometimes, the diagnosis of RAA is mistaken for Ebstein’s anomaly. Transthoracic echo is less sensitive than other tests such as CT, MRI, and transesophageal echo in detecting RAA. RAA might serve as a nidus for thrombus formation or a focus for atrial arrhythmias. 1 Management is not clearly defined, given its rarity. Medical follow-up with regular imaging is considered sufficient in asymptomatic patients with small aneurysms. Anticoagulation may be started in the presence of significant spontaneous echo contrast in those at risk of thrombus formation. 2 Surgical repair may be considered for giant atrial aneurysms to prevent the occurrence of such complications. 3
Authors’ Contributions
SSK (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead). SM (Conceptualization: Equal; Investigation: Equal; Supervision: Equal). SB (Conceptualization: Equal; Formal analysis: Lead; Writing – review & editing: Lead).
Data Availability Statement
No new data were generated or analyzed in support of this research.
Footnotes
Declaration of Conflicting of Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its amendments. Informed written consent was obtained from the patient concerned. No patient identity particulars have been disclosed.
Funding
The author received no financial support for the research, authorship and/or publication of this article.