
Abstract
Giant right atrial aneurysms are rare defects with different clinical presentations ranging from lack of symptoms to heart failure. They are diagnosed based on incidental findings. It is commonly found when echocardiography or chest X-ray is performed. Concurrent congenital heart disease and large atrial size are risk factors that may increase the risks of complications such as thromboembolism, fatal arrhythmias, aneurysm rupture, and sudden death. The best treatment has been controversial, with some patients managed surgically and others conservatively. We present a case of a giant right atrium aneurysm that was incidentally detected during a routine examination. The patient underwent successful surgical resection of the right atrial aneurysm.
Introduction
Giant right atrial aneurysms (RAA) are extremely rare congenital cardiac defects that are usually detected incidentally at any time between antenatal and adult life. The clinical presentation shows high variability. Patients with a right atrial aneurysm are known to have a high risk of arrhythmias and thromboembolisms.
Case Report
A 14-year-old boy was referred to our hospital for a giant RAA detected during a routine examination. Physical examination was normal, except for a grade 3 systolic murmur heard at the left sternal border. The patient’s heart rate was 78 beats/minute and was regular, the respiratory rate was 16 breaths/minute, the blood pressure was 110/70 mmHg, and the O2 saturation was 97% in the room air. Electrocardiography showed a normal sinus rhythm. The chest radiograph showed significant cardiomegaly and a prominent RA border (Figure 1). Transthoracic echocardiography showed a giant right atrial aneurysm measuring 8.45 × 28.12 cm in size (Figure 2). The tricuspid valve and the rest of the cardiac anatomy were normal. It was decided to perform surgical resection of the aneurysm after discussing different options with the family due to the risk of future thromboembolic events and arrhythmias. Surgery was performed through a median sternotomy and normothermic cardiopulmonary bypass. The pericardium was normal. A giant thin-walled aneurysm was observed throughout the free wall of the right atrium (Figure 3). After establishing cardiac arrest, the aneurysm was opened. There was no evidence of thrombosis or inflammation within the right atrial aneurysm. The aneurysm was resected (Figure 4). After excision of the affected atrial wall, the defect was closed with a continuous 4-0 Prolene suture and care was taken not to compromise the right coronary artery. The resected aneurysm was sent for pathological study, which revealed interstitial fibrosis and reduction of the muscular elements without evidence of an inflammatory reaction. The postoperative course was uneventful. The patient was discharged on the sixth postoperative day. At 25 years of age, he is asymptomatic with a normal right atrial size.

Chest X-ray showing severe cardiomegaly and right atrium enlargement.
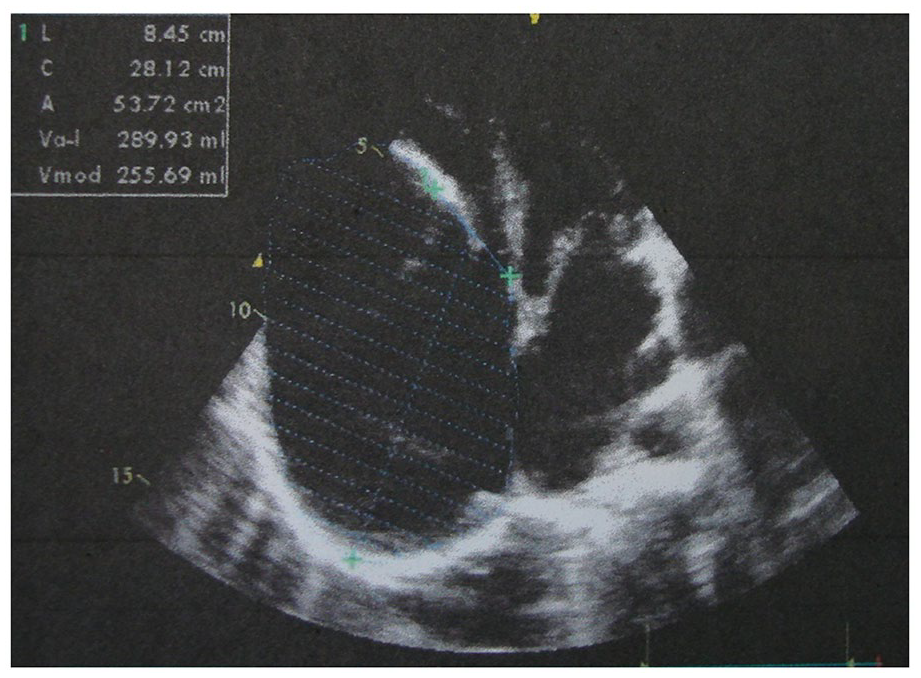
Echocardiography showing a giant right atrium aneurysm.

Intraoperative photographs view after the median sternotomy.

The resected right atrial aneurysm.
Discussion
The congenital aneurysm of the right atrium is a rare condition. It was first described by Bailey in 1955. 1 About 22 cases have been reported around the world. 2 RAA has been documented from the fetal stages to adulthood. 3 It is found most frequently in the third decade of life 4 and is more common in male patients than in female patients. 3 An atrial aneurysm is defined as an atrial dilation that involves all layers of the atrial wall. Its etiology is controversial, and the disease can be acquired or congenital. It is believed to be caused by dysplasia of the muscular wall of the right atrium. 5 Associated conditions consist of the atrial septal defect, ventricular septal defect, and coronary sinus diverticula. 6 The acquired type is seen in cases of pulmonary artery hypertension, congenital heart disease, and inflammatory changes in the myocardium. Giant aneurysms in the right atrium can be associated with annular dilatation and regurgitation of the tricuspid, which was not found in our patient. Right atrium aneurysms are rarer than left atrial aneurysms. 7 Many patients are asymptomatic, while some of them present with arrhythmias, palpitation, chest pain, and shortness of breath or fatigue. Major complications include heart failure, arrhythmias, rupture of the aneurysmal wall, and pulmonary embolism. Five deaths have been reported in patients with right atrial aneurysms. 8 The diagnosis can be confirmed by echocardiography, which can reveal underlying pathologies in addition to the right atrial aneurysm. Computerized tomography or cardiac magnetic resonance imaging is more sensitive and specific due to the description of cardiac structures. 9 Echocardiography was the technique of choice to establish the diagnosis in our case. The differential diagnosis includes pericardial effusion or cysts, tumors, mediastinal mass, and Ebstein’s anomaly. The management strategy ranges from conservative treatment using anticoagulation in asymptomatic patients to aneurysmectomy. Conservative management and regular monitoring are recommended for asymptomatic patients with no high-risk factors, but may not prevent complications. Due to the potential risk of life-threatening complications, early surgical resection is strongly recommended. Furthermore, surgical resection provides an active life without the use of anticoagulation. Giant right atrial aneurysms can be damaged during sternotomy, and the surgical team was aware of this complication. The long-term follow-up of our patient (11 years) showed an excellent overall prognosis.
Conclusions
The giant right atrial aneurysm is a very rare disease. It can be asymptomatic or present with various symptoms. Cardiac echocardiography plays a pivotal role in the diagnosis of this disease. Due to the risk of fatal complications, if a right atrial aneurysm is diagnosed in a patient, the appropriate treatment should be surgery even in the asymptomatic patient. The surgeon must be aware of damage to the right coronary artery and aneurysm during surgery.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors reviewed and approved the final manuscript.
Informed Consent
The patient gave his written consent for the publication of this report.