
Abstract
Background
Left main stenting with significant stenosis in symptomatic patients is an alternative strategy of revascularization in cases of low syntax scores with high surgical risk. Stent dislodgement is a rare complication, even rarer when it is already deployed. Percutaneous retrieval of a stent when it is fully deployed, is usually not recommended as it predisposes to a higher rate of dreaded vascular complications.
Case presentation
A case of dislodgment of a fully deployed stent in the left main is reported here, which was successfully deployed in another vascular bed without requiring invasive surgical retrieval.
Conclusions
Meticulous efforts for stent sizing, landing zone, and balloon expansion are of utmost importance, especially in cases of left main stenting where the risk of systemic embolization is higher. Monitoring stent position during balloon deflation, withdrawal, or manipulation of guide catheters is critical for promptly detecting stent dislodgement. Deploying a fully dilated dislodged stent in a favorable vascular bed is an important bail-out strategy.
Background
Stent dislodgement during percutaneous coronary intervention and subsequent entrapment in the lower limb are associated with significant adverse events. Moreover, percutaneous retrieval of dislodged stents is not usually recommended as it increases the risk of life-threatening complications. 1 A rare case of deployed stent dislodgement into the descending aorta and successful deployment of the stent in the external Iliac artery, is reported here, avoiding surgical retrieval.
Case Presentation
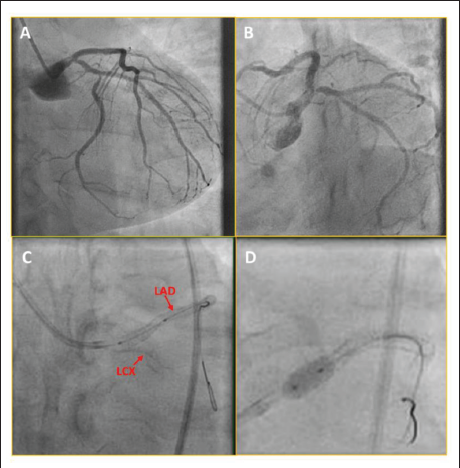
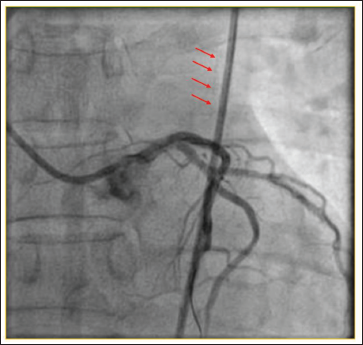
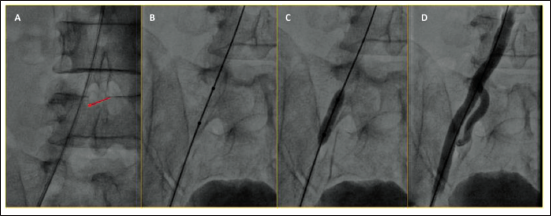
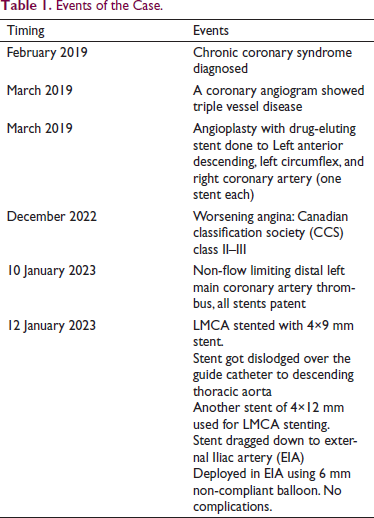
A 53-year-old gentleman with diabetes, systemic hypertension, dyslipidemia, and chronic smoking had angina since 2019. He underwent percutaneous coronary angioplasty (PCI) to all three vessels, that is, the Left anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) for triple vessel disease. Now, he presented with worsening angina. A coronary angiogram (CAG) revealed a non-flow limiting thrombus in the distal left main coronary artery (LMCA) (Figure 1A). LCX had ostioproximal 50%–60% stenosis with patent stents in all three vessels (Figure 1B). The patient opted for PCI over coronary artery bypass graft surgery (CABG). LCX and LAD were wired with 0.014 Runthrough™ (Terumo interventional system, Somerset, US) workhorse wire, using a 6-French JL3.5 guide catheter. LCX ostioproximal lesion was predilated with a 2×10 mm semi-compliant balloon with a fair result. The LMCA was pre-dilated with a 4×8 mm semi-compliant balloon. A 4×9 mm Resolute Integrity™ drug-eluting stent (Medtronic, Galway, Ireland) was deployed in distal LMCA across the stenosis (Figure 1C and D). The stent position was satisfactory. During post-dilatation, we noticed that the stent had dislodged from LMCA. Upon tracing the guide catheter through cine images, the stent was found over the guide catheter in the descending thoracic aorta (Figure 2). We continued the procedure as we were sure the stent could not go out of the guide catheter (as the coronary wire was placed till distal LAD). Another longer 4×12 mm Resolute Onyx™ drug-eluting stent (Medtronic, Galway, Ireland) was implanted from the left main ostium extending into LAD (Supplementary Figure 1). Proximal optimization was done with a 4.5×8 mm non-compliant balloon (Supplementary Figure 1). Kissing balloon dilatation was done to optimize LAD and LCX ostium (Supplementary Figure 2). The final angiogram showed good expansion of the stent with no complications. As we finished the stenting, the dislodged stent could not be visualized, and we screened the whole aorta with fluoroscopy. The stent was found (Figure 3A) just below the probable origin of renal arteries. We had a vascular surgery consultation for stent retrieval after bringing the stent into the femoral artery. We took a 4×12 mm stent balloon, passed through the dilated stent, and started bringing down the stent into the femoral artery. Unfortunately, the stent could not be brought further beyond the external Iliac artery (Figure 3B). So, the option of surgical retrieval was left to us. However, we planned to deploy the stent in the external Iliac artery and deployed it with a 6×12 mm balloon (Figure 3C). The post-deployment angiogram showed no occlusion, perforation, or dissection with the normal distal flow and branching of the common Iliac artery just above the stent (Figure 3D). Five months post-procedure, the patient is doing well without complications with normal bilateral lower limb pulses. Case events have been depicted in Table 1.
Deployed Stent Dislodged, went over the Guide Catheter and was seen in the Descending Thoracic Aorta (Red Arrows).
(A) Dilated Stent can be seen over the Guide Catheter in the Right External Iliac Artery (Red Arrow). (B, C) 6 mm Non-compliant Balloon Dilated at Nominal Pressure. (D) Final Angiogram Showing Normal Flow in the External Iliac Artery Without Complication.
Events of the Case.
Discussion
Stent dislodgement is a rare but known and potentially life-threatening complication of PCI, especially after the dislodgment of a fully deployed stent. Hence, percutaneous retrieval of fully deployed stents is not recommended. The dislodged stent can cause coronary perforation, coronary or aortic dissection, and embolization-related occlusive complications like myocardial infarction, stroke, limb ischemia, and mesenteric ischemia, depending on the vascular bed involved. 1 Factors associated with stent dislodgment are undersized or under-expanded stents, target vessel tortuosity, severe calcification and trial to deliver the stent to distal lesion through the pre-existing stent. 1 Retrieval or exclusion can be done either surgically or through percutaneous transcatheter techniques like a passage of a small distal balloon, the double-wire braiding technique or “knot” technique, the use of snaring device over a second wire, the stent-crush exclusion technique, extracting it by snaring from contralateral arterial access, and lastly deploying and crushing it in another similar sized vascular bed.2–8 Newer balloon-mounted stents with better radio-opacity made this complication rare. The prevalence of stent dislodgment is highest, with left main and LAD stenting, followed by LCX and RCA. 9
In our case, the first stent was probably undersized in reference to the length of the stent and the absence of an adequate landing zone, which was taken care of in the second attempt with a longer stent and landing part of the stent into LAD containing previous stent (landing of stent on a previous stent may hold the stent better after deploying). However, intracoronary imaging, which could have prevented the undersizing of the stent, could not be performed for financial reasons. Vijayvergiya et al. reported a case of deployed stent dislodgement from LMCA. However, it did not migrate to the thoracic aorta. Furthermore, stenting was deferred, and the patient was sent for CABG. 10 We could complete stenting with a longer stent as we were sure the dislodged stent would be over the guide catheter. We did not crush or extract from the contralateral side because of the risk of vessel injury due to the large size of the stent. We deployed it in the external Iliac artery and avoided an inevitable surgery.
Conclusions
Meticulous efforts directed towards stent sizing, landing zone and balloon expansion have made dislodgement of deployed stent extremely infrequent in the current era. This is especially true for left main stents, which are inherently associated with higher risk of systemic embolization. Early detection of stent dislodgement can be achieved by monitoring stent position during balloon elation, withdrawal or manipulation of guide catheters. Crushing the stent or extraction by snaring are acceptable rescue strategies in the setting of stent dislodgement. The larger size of the stent in this case made surgical exploration and retrieval more risky and led us to deploy stent in a more peripheral part of the vasculature.
Footnotes
Author Contribution
SM (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead).
MI (Investigation: Equal).
BLS (Investigation: Equal; Supervision: Equal; Validation: Equal).
Availability of Data and Materials
No new data were generated or analyzed in support of this research.
Consent for Publication
The authors confirm that written consent for submission and publication of this case report has been obtained from the patient in line with COPE guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Supplemental material
Supplemental material is available for this article online.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.