
Abstract
Coronary artery anomalies are a rare group of congenital cardiac disorders with an incidence of less than 1% in general population. Coronary cameral fistula (CCF) are abnormal vascular communications between coronary artery and a cardiac chamber. These fistulae result from congenital abnormalities or are acquired as a result of trauma or cardiac surgery. We present the transcatheter closure of a large CCF from right coronary artery (RCA) to right atrium in an eight-year-old girl.
Introduction
Coronary artery anomalies are a rare group of congenital cardiac disorders with an incidence of less than 1% in the general population. 1 A coronary-cameral fistula is an atypical vascular linkage connecting a coronary artery to a cardiac chamber. These fistulae result from congenital abnormalities or are acquired as a result of trauma or cardiac surgery. We present the transcatheter closure of a sizeable coronary cameral fistula (CCF) from the right coronary artery (RCA) to the right atrium (RA) in an eight-year-old girl.
Case Description
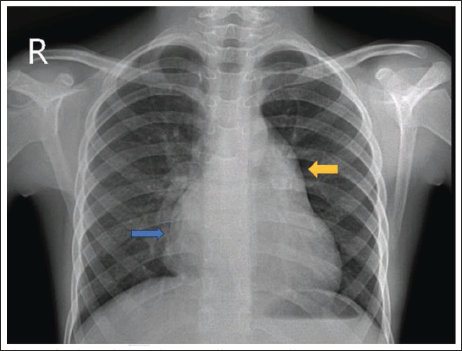
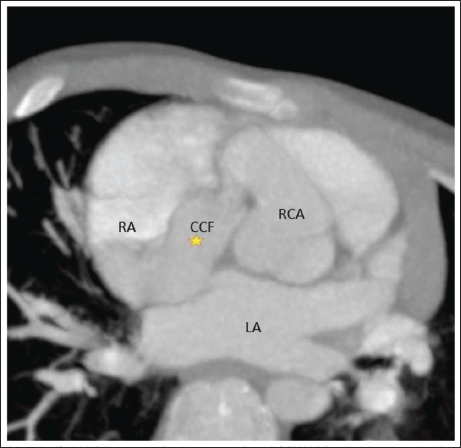
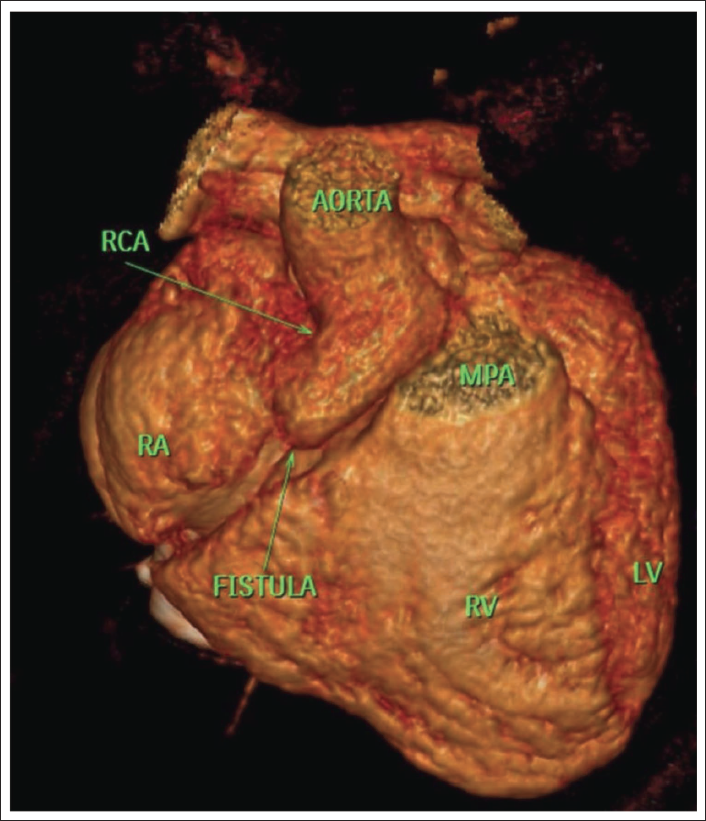
An eight-year-old girl, born out of a non-consanguineous marriage with normal developmental milestones and no prior hospital admissions was referred to us by a pediatrician for evaluation of abnormal heart sounds. On examination, there was mild cardiomegaly and a grade 3/6 continuous murmur was audible in the right lower sternal border. Her chest X-ray showed right atrial enlargement (Figure 1) and her Echocardiogram showed a CCF connecting the RCA to the RA, through an opening close to the lateral wall with a gradient of 70/35 mmHg. CT coronary angiogram confirmed a CCF involving the RCA with the tortuous course of the fistulous tract into the RA (Figures 2 and 3). A selective coronary angiogram of the RCA showed a hugely dilated fistulous tract opening into the RA (Figure 4A). The proximal RCA was dilated giving rise to a fistulous tract and its caliber was normal 10mm away from the right aortic sinus. The size of the fistula near the RCA end was 7 mm but widened out distally before opening into the RA.
CT Coronary Angiogram (Axial MIP [Maximal Intensity Projection] Images) Showing, Coronary Cameral Fistula (Indicated by *) Involving the Right Coronary Artery with Tortuous Course of the Fistulous Tract into the Right Atrium.
Three Dimensional Volume Rendered CT Image Showing the Coronary Cameral Fistula Involving the RCA into the Right Atrium.
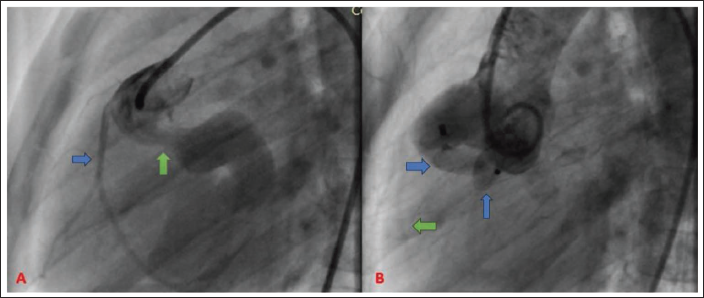
Right coronary injection in the left anterior oblique and lateral views demonstrated a dilated and tortuous fistulous tract with the native RCA arising proximally from the tract. A 7 JR guide was advanced into the fistula and a size 12 AMPLATZER™ vascular plug II (AGA Medical Corporation, Plymouth, Minnesota, USA) was deployed distal to the origin of the RCA. Angiogram after the device deployment showed good flow into the RCA and the fistulous tract was completely closed (Figure 4B). The child is doing well at three years of follow-up.
Discussion
Coronary artery anomalies encompass variations in origin, termination, structure, and course. Within this category, coronary artery fistulae (CAF) represent abnormal connections, either linking a coronary artery to a cardiac chamber (CCF) or extending to systemic or pulmonary vasculature, known as coronary arterio-venous fistula. CCF can be either single or multiple & occur between one or more coronary arteries & cardiac chambers. They occur in 0.08%–0.3% of unselected patients undergoing diagnostic coronary angiography. 2 Depending on the communication with the cardiac chamber, they can be classified as arterio-luminal (direct communication with the cardiac chamber) and arterio-sinusoidal (communication via a sinusoidal network). These CAFs can be either congenital or acquired. A congenital coronary fistula may manifest independently or as part of congenital cardiac anomalies linked to obstructions in the right and left ventricular outflow tracts, such as pulmonary atresia with intact ventricular septum and aortic atresia with hypoplastic left heart syndrome. Acquired CAF are usually seen after trauma, cardiac surgery and rarely following cardiac catheterization and angioplasty.
Clinical presentation of these fistulae depends on the size and the location of the fistula. The majority of these fistula are small, clinically insignificant, and picked up as incidental findings on routine examination and angiography. Most patients remain asymptomatic. Nevertheless, these anomalies have the potential to progress into hemodynamically significant fistulas, leading to symptomatic manifestations in 19% of patients aged below 20% and 63% of individuals aged 60 years and above. 3 Rarely these fistulae are large and hemodynamically significant resulting in coronary steal in the segment of myocardium supplied by the coronary artery distal to the fistula. Angina may be the presenting feature in patients with multiple fistulae. Additional complications encompass atrial fibrillation, bacterial endocarditis, cardiac failure, rupture, aneurysm formation, and the potential for sudden cardiac death.
Echocardiography usually reveals a dilated coronary artery and the site of drainage and helps quantify cardiac chamber enlargement. Cardiac CT provides accurate delineation of anatomy and cardiac catheterization is indicated primarily for shunt quantification and before intervention directed at closure of the defect.
Asymptomatic patients with hemodynamically insignificant fistula can be regularly followed up as there is a tendency for smaller fistulas to progress in size with age. Recommendations advocate for the elective closure of congenital coronary fistulas at an early age, particularly in cases where patients exhibit symptoms or present with a persistent murmur. 4 Though surgical ligation used to be the preferred method of treatment, transcatheter occlusion is increasingly becoming the method of choice. The various devices that have been used are vascular plugs, ductal occluders, covered stents, detachable balloons, Gianturco coils, and interlocking detachable coils. Careful case selection is important as device closure may not be suitable in small children with large fistulas requiring large-sized guide catheter, large wide fistula, fistula with multiple openings, the distal origin of fistula, fistulae near large coronary artery branches that may be inadvertently blocked off. The case described had a large CAF, however, slightly older age group, adequate separation from the RCA and the choice of device were factors contributing to the success of the procedure. The risks of transcatheter occlusion are risks of injury to the coronary artery by catheters/wires, coronary artery spasm, ventricular arrhythmias, and perforation. Other complications are myocardial ischemia due to occlusion of coronary artery branches, device embolization, residual shunt, and formation of thrombus proximal to the fistula.
Conclusion
Our illustrative case demonstrates that even large CCF can be safely closed by transcatheter techniques. Careful patient and device selection and pre-operative imaging are recommended to avoid complications.
Author Contributions
Conceptualization: Dr. Harikrishnan K N and Dr. Vishwanath Karthik.
Writing [original draft]: Dr. Nitin Naik and Dr. MallaPhanindra.
Review & editing: Dr. Deepa., Dr. Krishnamoorthy.
All authors read and approved the final manuscript.
Consent
The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the relatives of the patient inline with COPE guidelines.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.