
Abstract
Introduction
QRS voltages for electrocardiographic left ventricular hypertrophy (ECG-LVH) are more prominent in Black athletes than non-Black athletes. The underlying physiological relationships of ECG-LVH in BA remain enigmatic despite their greater predisposition to arterial hypertension.
Objectives
To determine the frequency of eight eponymous ECG-LVH criteria in male collegiate athletes in Nigeria; To determine the diagnostic performance of the most prevalent criteria; To determine the predictors of ECG-LVH.
Methods
34 (thirty-four) athletes and 49 (forty-nine) non-athletic controls with normal electrocardiograms and echocardiograms were retrospectively recruited from an existing pre-participation screening cohort. They were all normotensive, non-obese and normoglycemic, and matched for age and body mass index (BMI).
Results
The four most frequent criteria were Sokolow-Lyon index (67.6% vs. 36.7%; χ2 = 7.7; p = .006), Romhilt’s criterion (52.9% vs. 8.2%; χ2 = 20.6; p < .001), Peguero-Lo Presti criterion (38.2% vs. 22.4%; χ2 = 2.43; p < .144), and Mazzoleni’s criterion (35.3% vs. 4.1%; χ2 = 13.95; p < .001). The sensitivity, specificity and accuracy of these criteria ranged between 23.8%–57.1%, 38.5%–53.9%, and 32.4%–50.0%, respectively. Athletic activity (OR = 4.49; 95% confidence interval, CI = 1.63–12.36; p = .004) and lower BMI (OR = 0.78; 95% CI = 0.63–0.97; p = .026) were independent predictors of ECG-LVH by the Sokolow-Lyon criterion.
Conclusions
Voltage ECG-LVH criteria all poorly predict the presence of echocardiographic LVH in young male Black athletes. However, the Sokolow-Lyon criterion seems to be associated with a benign cardio-metabolic profile in such athletes and appears hypothetically superior to other voltage criteria for identifying physiological cardiac remodeling in them. This hypothesis should be tested in future studies.
Keywords
Introduction
Cardiac adaptation to regular and intense exercise training often takes the form of an increase in left ventricular mass, QRS voltages, or both. 1 Historically, this expression of left ventricular hypertrophy (LVH) has been more pronounced in male athletes and Black athletes. 1 Notably, the sickle cell trait (SCT), which is uniquely far more prevalent in Black athletes than Caucasian athletes, has not been demonstrated to significantly influence QRS voltages in Black athletes. 2
Pure voltage criteria for ECG-LVH are often favored by physicians because these criteria are inherently simple and easy to apply. 3 In general, the prevalence of ECG-LVH in athletes is as high as 64% with the Sokolow-Lyon voltage criterion. 4 This sharp contrast between the high prevalence of ECG-LVH, on the one hand, and the low event rates for cardiac death and morbidity in active athletes on the other, suggests that the consensus adoption of ECG-LVH as a physiological (rather than pathological) expression of the Athlete’s Heart4, 5 is, on purely epidemiological grounds, quite logical. Nevertheless, while the available ECG-LVH criteria admittedly lack sensitivity in the general population,6, 7 their considerably even poorer diagnostic performance among athletes is an ongoing puzzle and concern.8 –10 It is also not known if particular voltage criteria are superior in screening efficacy in specific athlete or sport populations 9 or, indeed, have intrinsically greater prognostic significance than others. This would be of particular concern in West Africa where previous studies among athletes have shown a high prevalence of echocardiographic LVH (“Echo-LVH”) especially of the concentric type.11 –14
Overall, there is a paucity of work on the diagnostic accuracy and clinical predictors of ECG-LVH in young athletes who have undergone a comprehensive cardiovascular pre-participation screening exercise. This study is the first in a racially homogeneous Black African context and aims to aid clinical decision-making in this increasingly dispersed and numerically prominent segment of the global sporting community.
Materials and Methods
This was a retrospective secondary analysis of the male population of an earlier comparative cross-sectional study in a leading federal university in Nigeria, the most populous Black African country. Ethical approval for the primary cohort was obtained from the Ethical Committee of the University Teaching Hospital.
The objectives of this study were: To determine the frequency of voltage criteria for ECG-LVH in male athletes of the university; To determine the diagnostic performance of the most prevalent criteria; To determine the independent predictors of ECG-LVH.
Recruitment into the study was offered to all the members of the university sports team. From the original 51 male respondents, 14 were initially excluded: three with blood pressure (BP) ≥140/90 mmHg; three with normal BP but body mass index (BMI) ≥30.0 kg/m2; two with BP and BMI ≥140/90 mmHg and 30.0 kg/m2, respectively; a sprinter (age <18), a wrestler (age >40); another sprinter (estimated GFR <60 ml/min/1.73 m2); a new member of the swimming team (weekly training duration <4 hours); two (a high jumper and a swimmer) with structural echocardiographic abnormalities; and a judoka with an abnormal ECG. Three other athletes (a sprinter, a shot-putter and a member of the taekwondo team) voluntarily withdrew before the conclusion of the study and their data was therefore excluded from the statistical analysis. Other exclusion criteria included: a history of bronchial asthma, use of performance-enhancing substances, or known diagnosis of (or treatment for) a cardiovascular disease. In total, thirty-four athletes were finally recruited. Forty-nine non-athletic male controls who satisfied the inclusion and exclusion criteria, and who were matched for age and BMI with the male athletes, were recruited from a pool of 54 male subjects recruited consecutively for the original study. “Non-athletic” was defined as engaging in <2 hours of leisure time/organized physical activity per week. 14 78.2% of the controls were from the College of Health Sciences while the remainder were from other faculties.
A structured questionnaire was administered and the athletes were then grouped into different combinations of dynamic and static sport types according to Mitchell’s classification. 15 Static component was categorized as low, moderate and high if the estimated percentage of maximum voluntary contraction (MVC) was <20, 20–50, or >50, respectively, while dynamic component was categorized as low, moderate and high if the estimated percentage of maximum oxygen uptake was <40, 40–70, or >70, respectively. 15 Training duration was self-reported. Standard protocols for anthropometry, 16 BP measurements, 17 resting electrocardiography, 18 and trans-thoracic echocardiography 19 were adopted. Resting 12-lead electrocardiograms (ECGs) were recorded with a Schiller Cardio Vit AT-2 Plus machine (Schiller AG, Altgasse, Switzerland). A portable Sonosite Micromaxx ultrasound imaging system (Sonosite, Gersweiler, Germany), equipped with a 2.5 Hz transducer, was employed for trans-thoracic echocardiography. Left ventricular mass (LVM) was indexed to body surface area (BSA), that is, left ventricular mass index (LVMI), and values of ≥116 g/m2 were considered diagnostic of LVH. 22 Relative wall thickness (RWT) of <0.42 with LVMI <116 g/m2, RWT ≥0.42 with LVMI <116 g/m2, RWT ≥0.42 with LVMI ≥116 g/m2, and RWT <0.42 with LVMI ≥116 g/m2, respectively, defined normal left ventricular geometry, concentric left ventricular remodeling, concentric LVH, and eccentric LVH. 19
Electrocardiograms were interpreted with the 2017 International Criteria (IC). 4 R-wave amplitudes in leads I, II, aVL, aVF, V5, and V6, as well as S-wave amplitudes in leads III, a VR, V1, V2, V3 and V4, were determined. The deepest S-wave amplitude across all 12 leads was determined and termed S-D. All wave amplitudes were expressed in millimeters (mm). The following eponymous voltage criteria were then specifically investigated: Gubner (R-I ≥15 mm or R-I + S-III ≥25 mm), Goldberger (R-aVF ≥20 mm), Schack (S-aVR ≥19 mm), Cornell (S-V3 + R-aVL ≥28 mm in men), Sokolow-Lyon (R-aVL ≥11 mm, or S-V1 + R-V5 or V6 ≥35 mm), Wilson (S-V1 ≥23 mm, or R-V5 ≥33 mm, or R-V6 ≥25 mm), Mazzoleni (S-V2 ≥25 mm), 6 and Peguero-Lo Presti (S-D + S-V4 ≥28 mm in men). 7
Ten milliliter of venous blood was taken for hemoglobin electrophoresis, hematocrit, and assays for fasting plasma glucose, total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, serum sodium, potassium, bicarbonate, urea, creatinine, albumin and calcium. All specimens were analyzed in the Hematology and Chemical Pathology departments of the university teaching hospital.
Statistical Analysis
Data analysis was performed with IBM SPSS Statistics (Version 23). The Shapiro-Wilkes test was used to determine normality of distribution of continuous variables. Correlation of LVMI with both normally and non-normally distributed QRS voltages was done with Pearson and Spearman’s coefficients, respectively. A 2-tailed p value of ≤.05 was considered statistically significant. Strength of correlation was ranked as negligible (0.00–0.10), weak (0.10–0.39), moderate (0.40–0.69), strong (0.70–0.89), or very strong (0.90–1.00). 20 The magnitude of observed inter-group differences, that is, effect sizes (Hedges’ g) was calculated using an interactive online tool (Statology, 2022) and obtained values were assigned the following interpretations: 0.2 = small; 0.5 (medium); >0.8 (large). 21 Chi-square analysis was performed to compare the prevalence of various ECG-LVH criteria in athletes and non-athletes. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of the most frequently occurring ECG-LVH criteria were calculated. The relationships of the following physiological variables (with proven influence on ECG-LVH in an athletic and/or young healthy population) were subsequently assessed for the most frequently occurring ECG-LVH criterion: BMI/obesity,4, 6, 23, 24 age, 22 SBP, 25 heart rate/pulse rate, 24 and FPG. 25 A similar approach was adopted for Echo-LVH. Parameters with a p value of <.20 on univariate regression were selected for multiple binary logistic regression. In the final models, variables with a p value of ≤.05 were considered statistically significant.
Results
Clinical and Non-electrocardiographic Characteristics
The mean age (in years), BMI (in kg/m2), and training duration (in years) of the athletes were 25.7 (4.4), 23.6 (2.3) and 7.1 (4.5), respectively. Six major sports disciplines were represented: track and field (16 athletes; 47.1%), judo (four athletes; 11.8%), swimming (five athletes; 14.7%), taekwondo (five athletes; 14.7%), badminton (three athletes; 8.8%), and squash (one athlete; 2.9%). They were categorized as high static-low dynamic (nine athletes; 26.5%), moderate static-moderate dynamic (12 athletes; 35.3%), high dynamic-moderate static (six athletes; 17.6%), and high dynamic-low static (four athletes; 11.8%). Three athletes (8.8%) were tagged “unclassified” due to the inadvertent omission of specific data (e.g., actual distance covered during their respective events) in the self-reported section of the questionnaire. The other clinical characteristics of the athletes and controls are summarized in supplemental Table 1. Most of the athletes had concentric left ventricular remodeling or concentric LVH (supplemental Table 2).
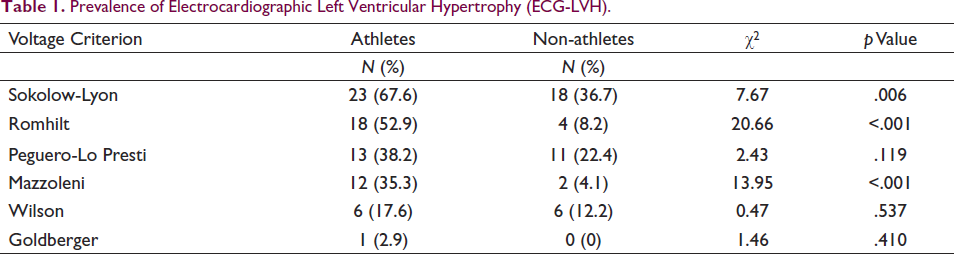
Prevalence of Electrocardiographic Left Ventricular Hypertrophy (ECG-LVH).
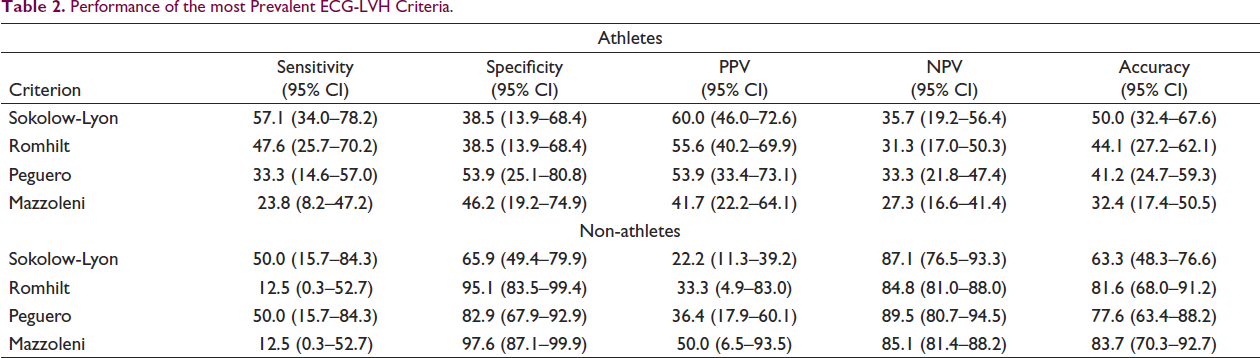
Performance of the most Prevalent ECG-LVH Criteria.
Electrocardiographic Characteristics
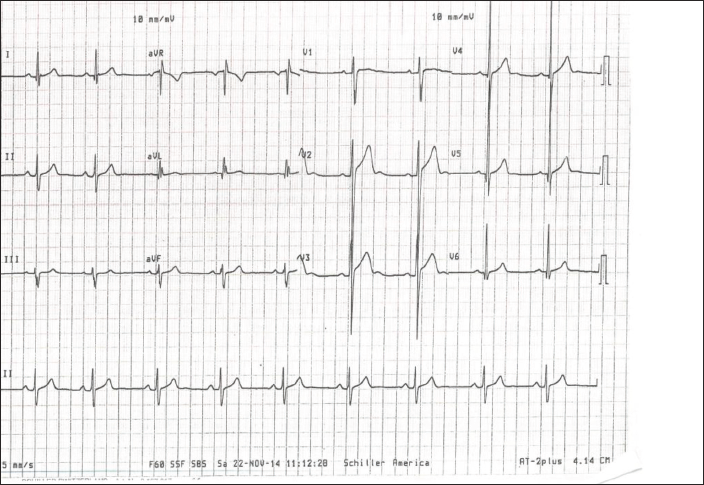
There was no significant correlation between LVMI and QRS voltages in the athletes (supplemental Table 3). There was moderate positive correlation between LVMI and both S-V4 and S-V3 + R-aVL voltages in non-athletes (supplemental Table 4). The prevalence of ECG-LVH is summarized in Table 1. Only one athlete fulfilled a limb lead criterion in the entire study population. The overall prevalence of ECG-LVH in athletes ranged from 2.9% (Goldberger) to 67.6% (Sokolow-Lyon). Figure 1 is an ECG of an athlete who met multiple precordial voltage criteria.
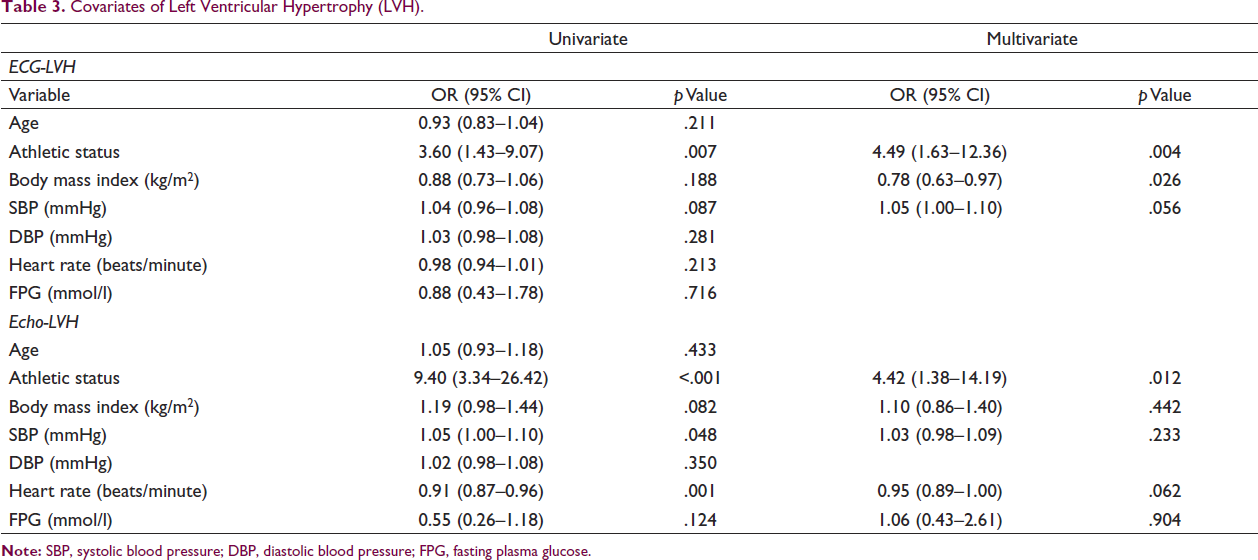
Covariates of Left Ventricular Hypertrophy (LVH).
ECG of a 19-year-old sprinter who met the Mazzoleni, Peguero-Lo Presti and Sokolow-Lyon voltage criteria.
Among athletes, the most sensitive (57.2%, 95% CI: 34.0–78.2) and most accurate (50.0%, 95% CI: 32.4–67.6) ECG-LVH criterion was the Sokolow-Lyon index, whereas the Peguero-Lo Presti criterion (53.9%, 95% CI: 25.1–80.8), was the most specific. The test characteristics of the four most common ECG-LVH criteria are summarized in Table 2.
Logistic regression analysis results for ECG-LVH (Sokolow-Lyon criterion) are summarized in Table 3. Being an athlete (OR = 4.49, 95% CI: 1.63–12.36, p = .004) and having a lower BMI (OR = 0.78, 95% CI: 0.63–0.97, p = .026) were the only independent predictors of ECG-LVH in a multivariable model with an AUC of 73.6% (95% CI: 62.9–83.4; p < .001) (see supplemental Figure 1). As depicted in supplemental *Figure 2, the equivalent figures for the Echo-LVH model were 81.4% (95% CI: 71.5–91.3; p < .001).
Discussion
The 67.6% prevalence of ECG-LVH in the athletes (by the Sokolow-Lyon index) was comparable to previous global figures. 4 This particular criterion has also been either explicitly 4 or implicitly 5 recommended by expert guidelines for ECG interpretation in athletes. One notable guideline mentions the Cornell voltage criterion as an alternative. 5 However, no athlete in this study fulfilled Cornell’s voltage criterion. Indeed, only one athlete met a limb lead criterion. This contrasts with the 8.1% prevalence of the Cornell criterion in a large and predominantly Black cohort of basketball players, 26 although the difference could be partly due to the significantly larger body size of subjects in the study in question and their sport type which has a high dynamic component.
In our study, certain voltage criteria (Sokolow-Lyon, Romhilt, and Mazzoleni) were significantly more prevalent in athletes whereas others (Peguero-Lo Presti, Wilson, and Goldberger) were not. However, in spite of the high prevalence of both ECG-LVH and Echo-LVH in our cohort, the correlation between all QRS voltages and LVMI was poor. Unsurprisingly, this translated to a poor diagnostic performance. In spite of differences in racial composition and lower Echo-LVH prevalence rates than those in our study, a similarly poor diagnostic accuracy for the Sokolow-Lyon index was found in previous studies among predominantly male and/or endurance athletes.9, 10 Therefore, even though the athlete ECG interpretation guidelines seem to favor the Sokolow-Lyon index,4, 5 the available data suggests that all current ECG-LVH criteria are unsuitable for screening for Echo-LVH in athletes and, indeed, in young people in general. 6
Logistic regression analysis revealed athletic status and lower BMI as the only independent predictors of the Sokolow-Lyon index in this study. Negative correlation of the Sokolow-Lyon index and positive correlation of the Cornell voltage criterion with BMI/obesity have been shown in other studies.8, 23, 24 Obesity was not prevalent in our athlete pool and was actually an exclusion criterion. While SBP was predictive of ECG-LVH in regularly exercising young people in the study by Lee et al., 23 it just fell short of statistical significance in our own multivariable model for ECG-LVH (OR = 1.05; 95% CI = 1.00–1.10; p = .056). We, therefore, acknowledge that, in an athlete population drawn from a region with a high prevalence of hypertension such as ours, 12 the combination of a concentric LV geometric pattern with ECG-LVH should naturally prompt consideration of systemic hypertension as a contributory factor for the observed cardiac remodeling. The current global perspective, however, is that concentric remodeling/hypertrophy is not necessarily pathological in male athletes. 28
Although arterial hypertension is the most common cardiovascular condition among athletes, 27 the most common cause of sudden cardiac death in young athletes is hypertrophic cardiomyopathy (HCM). However, the prevalence rates of this disease in the general population and the elite athletic populations are 0.2% and 0.06%, respectively,14, 29 and <2% of HCM patients have isolated voltage criteria for ECG-LVH (i.e., without repolarization abnormalities).4, 5 Against this backdrop, our study provides some evidence that isolated ECG-LVH is most likely an innocuous finding in a male Nigerian athlete who is asymptomatic, normotensive, euglycemic, and has a normal BMI.
This study has notable limitations. The small sample size must be acknowledged. Again, although care was taken to ensure that data for all the included subjects was complete, the retrospective design has intrinsic methodological flaws. Also, bearing in mind that obesity was an exclusion criterion, the study outcomes cannot be extrapolated to obese athletes. Furthermore, in view of the high incidence of the white coat effect among athletes, 27 ambulatory blood pressure monitoring (ABPM) could potentially have clarified the relationship between ECG-LVH and SBP in this study. On the other hand, routine ABPM is impractical in a real-world cardiovascular pre-participation screening scenario. Lastly, since the study population consisted exclusively of male athletes predominantly engaged in sports with a moderate to high static component, the results cannot be logically generalized to either female athletes or male athletes engaged in predominantly dynamic (i.e., endurance) disciplines.
Conclusions
Similar to findings from a large study involving athletes of West African ancestry, 30 young male Nigerian athletes (engaged in predominantly power sports) have a high prevalence of both ECG-LVH and Echo-LVH. The presence of isolated Sokolow-Lyon index for ECG-LVH in asymptomatic athletes of this type was significantly associated with a benign cardio-metabolic profile in this study. Thus, routine echocardiography, which is expensive and not easily accessed in this geographical setting, would most likely be superfluous in such athletes. 30 Similarly, ABPM and biochemical investigations like fasting plasma glucose and lipid profile, which carry a substantial additional cost, should be requested in such asymptomatic athletes only when clinically merited, for example, in the setting of suspected systemic hypertension. Further research in a larger number of athletes from the study population is needed to validate these findings and also to clarify whether these conclusions are unique to certain voltage criteria (e.g., the Sokolow-Lyon index in this study) or whether they apply to all pure voltage criteria (including limb lead criteria) across different demographics and sporting disciplines.
List of Abbreviations
ABPM: Ambulatory Blood Pressure Monitoring
BMI: Body Mass Index
BP: Blood Pressure
BSA: Body Surface Area
CI: Confidence Interval
DBP: Diastolic Blood Pressure
ECG: Electrocardiogram
ECG-LVH: Electrocardiographic left ventricular hypertrophy
Echo-LVH: Echocardiographic left ventricular hypertrophy
FPG: Fasting Plasma Glucose
GFR: Glomerular Filtration Rate
HCM: Hypertrophic Cardiomyopathy
HDL: High Density Lipoprotein
IBM: International Business Machines
IC: International Criteria
LDL: Low Density Lipoprotein
LVH: Left Ventricular Hypertrophy
LVM: Left Ventricular Mass
LVMI: Left Ventricular Mass Index
NPV: Negative Predictive Value
OR: Odds Ratio
PPV: Positive Predictive Value
ROC: Receiver Operating Characteristic
RWT: Relative Wall Thickness
SBP: Systolic Blood Pressure
SCT: Sickle Cell Trait
SPSS: Statistical Package for the Social Sciences
Author Contributions
All authors had access to the data and participated in writing the manuscript.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Approval was duly obtained for the primary study on which this work was based.
Funding
There was no specific external funding for this manuscript; the primary work (already published) on which it is based was principally funded by Tochukwu F. Ilodibia in addition to a statutory dissertation grant from UPTH.
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.