
Abstract
Takotsubo cardiomyopathy (TCMP), also called as stress cardiomyopathy, is a transient left ventricular (LV) dysfunction. TCMP’s association with endocrine and thyroid diseases has been recently described, but TCMP in a patient of Hashimoto’s thyroiditis with encephalopathy is rarely reported. 1 Here, we present a recent case of TCMP in a patient with Hashimoto’s encephalopathy who was treated with steroids and responded well. Our case here highlights about having a lower threshold for screening of thyroid and other endocrine disorders in patients with TCMP.
Introduction
Takotsubo cardiomyopathy (TCMP) is transient left ventricular (LV) dysfunction presenting with dyspnea, hypotension, ECG changes, and raised troponin levels with no significant coronary angiogram findings. It is also known as stress cardiomyopathy as it is usually seen after emotional or physical stress. The typical variant has a hyperkinetic LV base with focal apical akinesis which results in apical ballooning. 2 TCMP’s association with endocrine and thyroid diseases has been recently recognized. However, case reports are scarce, and the mechanism by which thyroiditis triggers TCMP is also not well understood. Hashimoto’s encephalopathy itself is a rare disorder that presents as progressive confusion, seizure, ataxia, myoclonus, and psychosis in a relapsing-remitting manner. It is thought to be immune-mediated, but again its exact pathophysiology remains unclear. 3 Awareness of this entity in a relevant clinical setting is important for prompt management.
Case Report
A 48-year-old female was admitted to another hospital with complaints of fever for 7 days along with altered behavior and one episode of seizure. She was managed as a case of meningitis and was on empirical antibiotics and anti-epileptic. Contrast-enhanced computed tomography (CECT) of the brain was done at that hospital which showed no significant findings. Lumbar puncture (LP) was also done in which cerebrospinal fluid (CSF) analysis was unremarkable (Table 1). After 4 days, she developed shortness of breath and cough. In view of ECG changes and Troponin I positivity along with new symptoms and poor response to treatment, she was referred to our hospital.
Relevant laboratory investigations
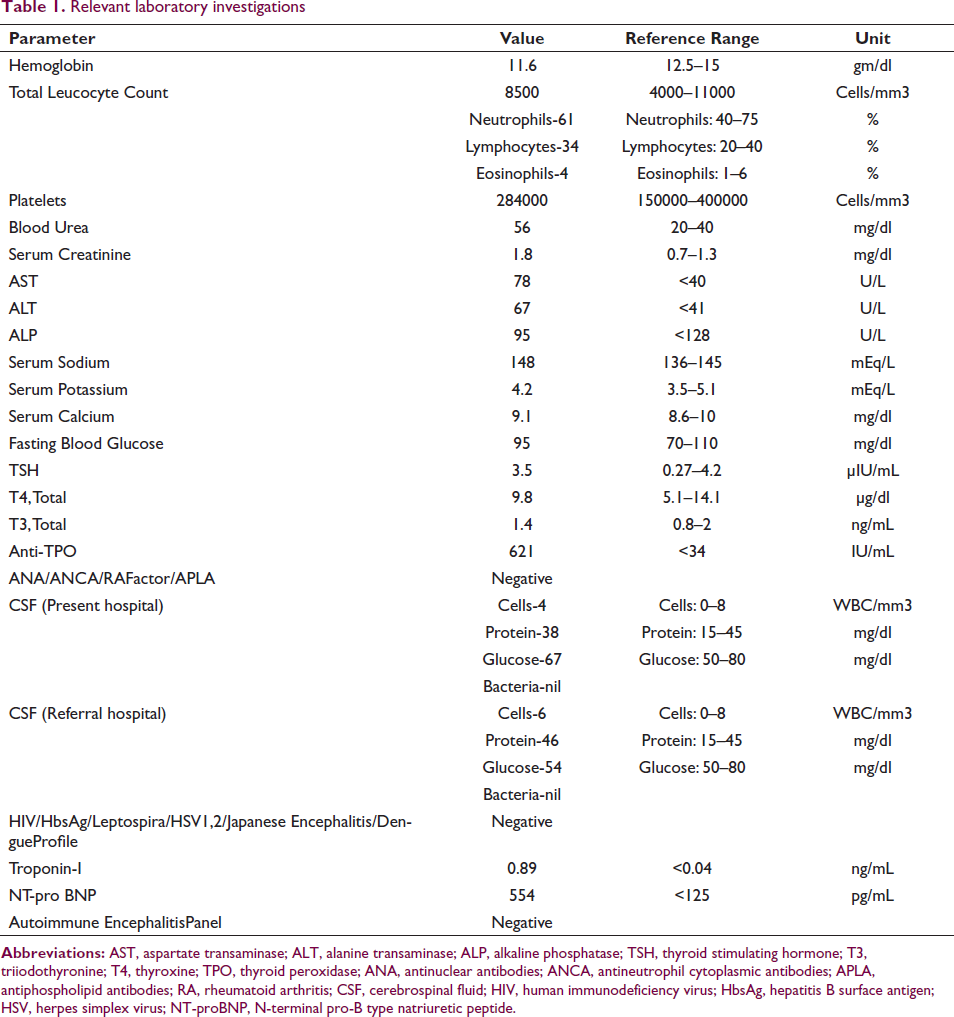
She was a manual laborer by occupation and had no history of any cardiac illness, diabetes, hypertension, tuberculosis, thyroid, or renal illness in the past. She was an occasional tobacco chewer with no other significant personal or family history. On examination, she was found to be febrile, irritable, and dyspneic. Her pulse was 120/min and her blood pressure was 140/88 mm of Hg. Oxygen saturation was 98% on room air. On neurological examination, the planter reflex was bilateral extensor and knee jerk reflexes were normal. Kernig’s sign was negative and brain stem reflexes were intact. There was no obvious focal deficit. A cardiovascular examination revealed tachycardia with gallop rhythm and no murmur. On chest auscultation, the patient had bilateral basal fine crepitations. A routine blood investigation along with Troponin I, NT proBNP, and blood culture was sent. The patient had mildly deranged liver and renal function along with elevated troponin I and NT-proBNP (Table 1).
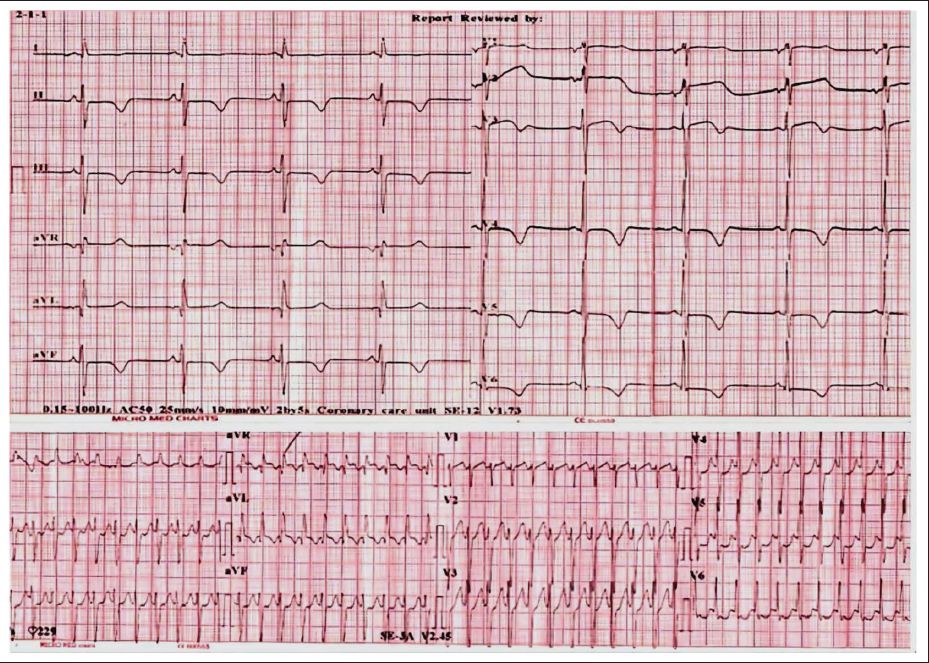
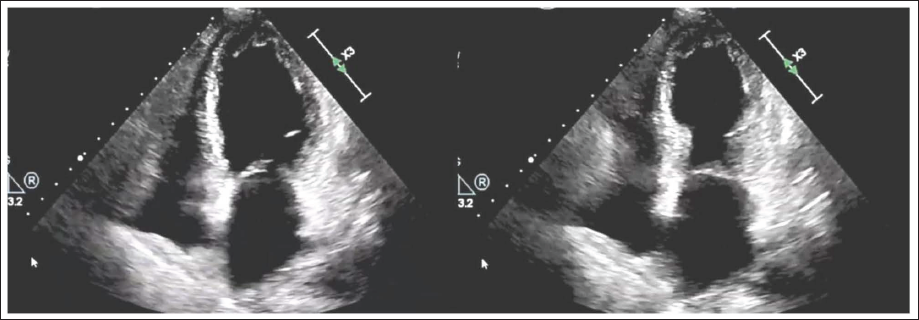
A few hours after hospitalization, patient complained of heaviness in the chest with palpitation and she became drowsier and more irritable. She also developed hypotension (blood pressure of 86/54 mmHg) with ECG showing narrow complex regular tachycardia – supraventricular tachycardia (SVT) for which she was immediately DC cardioverted. Post-cardioversion ECG showed left anterior hemiblock with diffuse T-wave inversion, subtle ST depression of 0.5 mm in leads II, III, aVF, and V6, and QTc prolongation (QTc – 520 msec) (Figure 1). Echo showed apical hypokinesia more pronounced in the apical anterior septum and anterior wall with normal to hyper-contracting basal segments (Figure 2). Overall ejection fraction was reduced. InterTAK Diagnostic Score 4 was calculated and it was 53 (Female sex-25, Physical stress-13, Neurological disorder-9, QTc prolongation-6) which was suggestive of TCMP.
Electrocardiograms (ECG) of the patient: Top graph showing diffuse T-wave inversion, subtle ST depression in inferior leads and QTc prolongation, and bottom graph showing narrow complex regular tachycardia suggestive of supraventricular tachycardia (SVT).
Echocardiograms of the Patient Showing Apical Hypokinesia with Normal Contracting Basal Segments (Apical Ballooning).
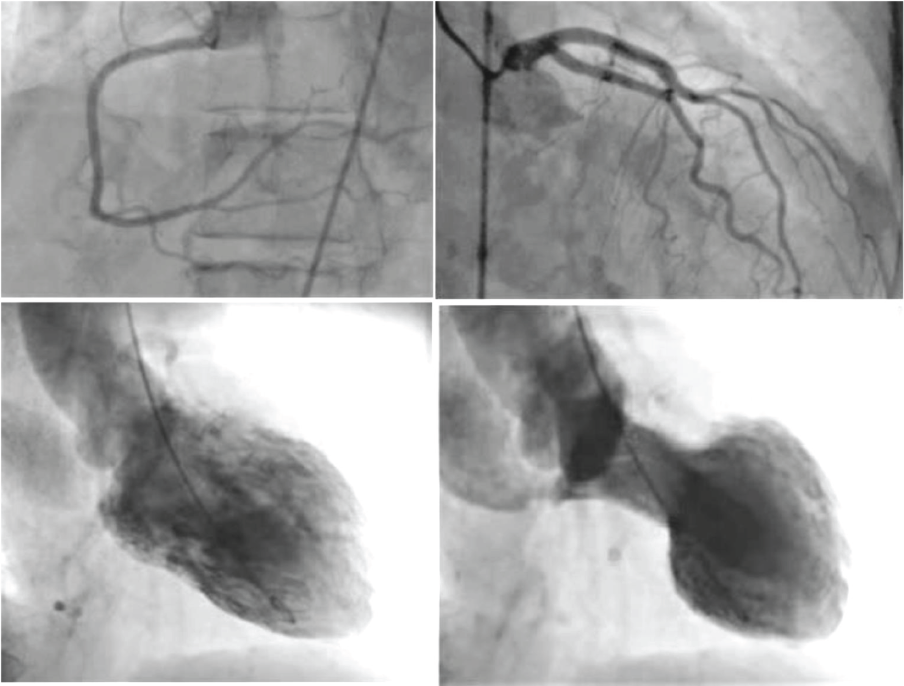
The patient was taken up for cardiac catheterization. The coronary angiogram revealed normal epicardial coronary arteries, and the LV angiogram showed apical hypokinesia with basal sparing (Figure 3). Hence, the diagnosis of TCMP was confirmed and the patient was started on aspirin, beta blockers, and diuretics. ACE inhibitors were not given as serum creatinine was elevated. It was added later at the time of discharge.
Coronary Angiograms of the Patient Showing Normal Coronaries Along with left ventricular (LV) Angiogram Showing Apical Ballooning.
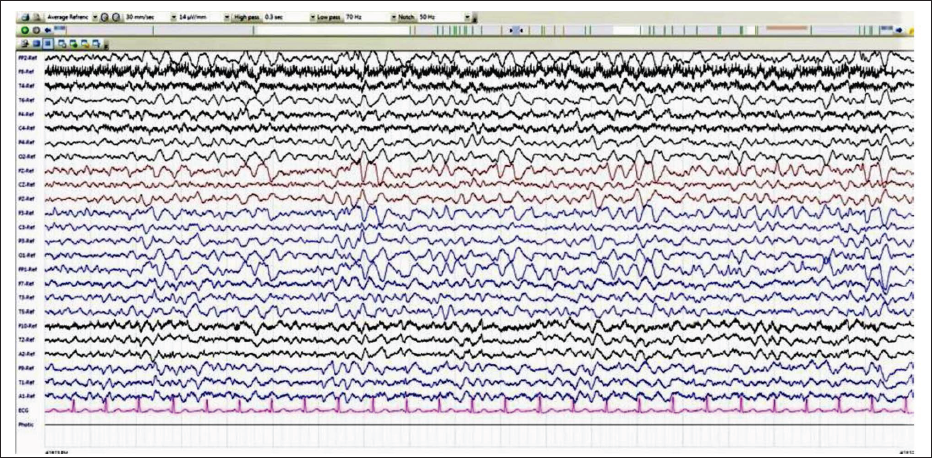
MRI brain and EEG were done on subsequent days. MRI revealed normal study and EEG showed generalized high amplitude, frontally dominant slow waves suggestive of encephalopathy, respectively (Figure 4). CSF analysis and blood culture did not reveal any abnormality. Based on clinical presentation, poor response to the empirical treatment, and normal CSF evaluation, the possibility of autoimmune etiology was considered.
Electroencephalogram (EEG) of the Patient Showing Generalized High Amplitude, Frontally Dominant Slow Waves.
She was started on treatment with steroids with which she showed drastic improvement in her sensorium. Thereafter, she was worked up for any systemic autoimmune disease. Her ANA profile, ANCA, RA factor, APLA panel, and autoimmune encephalitis panel were negative. However, the Anti-TPO antibodies showed elevated titers (Table 1). The thyroid gland was normally palpable with no evidence of goiter. A thyroid ultrasound was done which was suggestive of thyroiditis. The thyroid function test did not reveal any abnormality. The patient was eventually discharged on a tapering dose of steroids along with anti-epileptics, aspirin, beta-blockers, diuretics, and ACE inhibitors. Anti-TPO antibody titers showed a declining trend on the follow-up visits but were still elevated. After 3 months, the echocardiography showed normal LV function and there was no recurrence.
Discussion
Hashimoto’s encephalopathy also called steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) was first described by Fatourechi. 5 It is a rare condition to diagnose due to its varied presentation. Hence, many times it is underdiagnosed. It should be considered in the presence of neuropsychiatric symptoms and other systemic manifestations, but with no significant CSF/imaging finding. Such patients show markedly elevated antithyroid antibodies in serum and show a good response to immunosuppressive therapy. If left untreated, this can lead to coma and death. Although the exact pathophysiology is unknown, it is believed that a common marker of autoimmunity for thyroiditis and encephalopathy may be present. TCMP as explained earlier is a transient and reversible LV dysfunction with normal coronaries. InterTAK Diagnostic Score which calculates various points for the female gender, emotional trigger, physical trigger, absence of ST-segment depression, psychiatric disorder, neurological disorder, and QTc prolongation is a sensitive tool to diagnose and differentiate it from acute coronary syndrome. 4
Several variants of TCMP have been described. A typical variant has a hyperkinetic base with hypokinesia or akinesia in the focal apical segment of LV, but inverted or basal pattern, mid-level circumferential hypokinesia, and RV pattern are also uncommonly reported. 4
Takotsubo cardiomyopathy is a form of myocardial stunning but with different cellular and biochemical mechanisms when compared to acute coronary syndrome-related transient ischemia. Its pathophysiology is complex and unclear, but hypothalamus-pitutary-adrenal (HPA) axis-mediated, catecholamine-driven cardiac dysfunction is the most accepted hypothesis. Beta-adrenoceptors are in greatest density at the apical myocardium which explains its regional nature of involvement as described. 6 The adrenergic and thyroid systems are closely related so much that manifestations of hyperthyroidism mimic the hyperadrenergic state. The catecholamine’s action potentiating effect of thyroid hormone is suggested by the studies showing upregulation of beta-adrenergic receptors in the myocardium despite normal circulating levels of catecholamines. 7 Other hypotheses consider vasospastic angina and an imbalance of sympathetic and vagal system modulation. There are few case reports of TCMP associated with Grave’s disease, toxic multinodular goiter, following thyroidectomy, and radioactive iodine treatment. 8 TCMP has also been shown to occur in the hypothyroid or subclinical hypothyroid state although the increased risk of atherosclerosis and myocardial dysfunction associated with hypothyroidism should be kept in mind. 9 Other endocrine disorders that have shown close relation with TCMP are pheochromocytoma, adrenal insufficiency, diabetes mellitus, autoimmune polyendocrine syndrome, and syndrome of inappropriate antidiuretic hormone secretion.
Conclusion
At present, it is difficult to reliably estimate the frequency of associations between TCMP and various endocrine disorders. The overall causal connection between TCMP and thyroid or other endocrine disorders is also in debate. Larger studies and TCMP registries are needed to have a better understanding of TCMP’s relationship with thyroid and other endocrine diseases. Acknowledgment of an endocrine condition with TCMP and hence lower threshold for screening of such disorder in patients with TCMP will offer a great therapeutic advantage.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All procedures performed in this case were in accordance with the ethical standards of the institutional and/or national research committee. All identifiable patient information has been removed from this manuscript.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Patient’s Consent
The patient’s consent was taken for this publication, and the identity of the patient has not been disclosed.