
Abstract
Coronary artery calcification in patients with coronary artery disease is associated with increased major adverse cardiovascular events. They are usually diagnosed on a computed tomography scan or on an invasive coronary angiography. A 60-year-old male was diagnosed with acute coronary syndrome after presentation with one month of worsening angina. Coronary angiography showed triple vessel disease (mid left anterior descending artery and mid right coronary artery having total occlusion and a 70% stenosis in the left circumflex artery). Apart from this, there was a heavily calcified right coronary artery with a C configuration evident on fluoroscopy. A computed tomography coronary angiography was done to visualize the distal vessels. The calcium score was 5988. Retrospectively, on inspection of the chest X-ray, there was calcification on the right heart border. The patient was medically managed and referred to a cardiothoracic vascular surgeon for coronary artery bypass grafting. Coronary artery calcification on X-ray is rare and hence being presented along with the review of the literature.
Keywords
Introduction
Radiologic detection of calcification within the heart is quite common and is of varied etiology. Calcification of the aortic, mitral valve may indicate a hemodynamically significant valvular disease according to the calcium density over the valves. Myocardial calcification is a sign of prior infarction, while pericardial calcification strongly suggests constrictive pericarditis. The amount of coronary artery calcification (CAC) as quantified by the Agaston score strongly correlates with the severity of coronary artery disease (CAD). Detection of the calcification of the heart on imaging modalities has clinical implications. All these calcifications have characteristic radiological appearances aiding in their identification. Coronary stents may be visible on chest X-rays particularly the old-generation stents (due to increased strut thickness and they being bulky). However, the coronaries being small structures, radiologically the stents appear like a chicken-wire mesh. These cannot be differentiated when the coronaries are heavily calcified.
Coronary calcification is an active process related to widespread atherosclerosis, frequently observed in advanced lesions. There is strong evidence that radiographically detectable coronary calcium predicts future major adverse cardiovascular events (MACE). Currently, there is an increasing trend to rely on CAC detected on computed tomography (CT) scans to detect subclinical CAD, which is not cost-effective.
Chest radiographs have low sensitivity in detecting CAC despite their low cost and easy availability. Coronary calcification and delineation of the anatomic structures can be well defined by the newer imaging modalities because of better temporal and spatial resolution (i.e., fluoroscopy, electron beam CT, and double helical CT).
Case
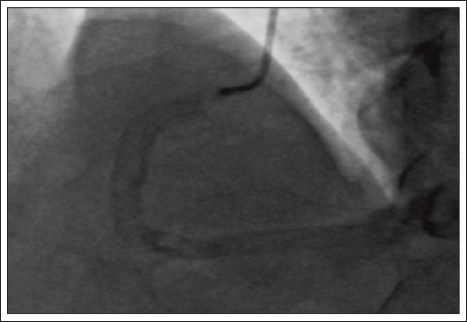
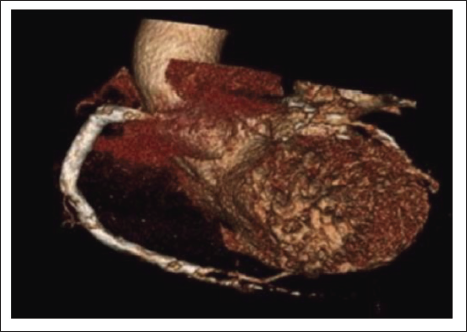
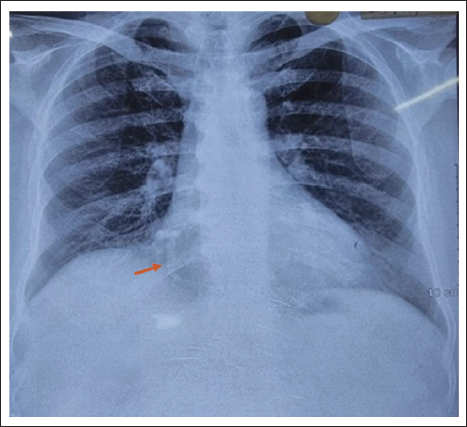
A 60-year-old male, hypertensive, diabetic presented with worsening angina of a month duration. At presentation, electrocardiography (ECG) showed T wave inversions in the precordial leads. The serial troponin levels were normal. The echocardiography showed global hypokinesis of the left ventricle with moderate left ventricular dysfunction. A diagnosis of unstable angina with ECG changes was made. The biochemical profile and other routine blood investigations were normal. He was posted for an angiogram. Fluoroscopy showed calcification of the right coronary artery (RCA) (Figure 1). The angiography showed chronic total occlusion of the mid left anterior descending (LAD) coronary artery and the RCA, 90% stenosis in the left circumflex artery (LCX), and the posterior descending artery (PDA). A CT angiography was planned to see the extent of calcification and the distal vessel configuration. It confirmed the invasive angiography findings (Figure 2). The total calcium score was 5988. When his chest X-ray was reevaluated, there was C C-shaped calcification on the right heart border (Figure 3). He was planned for early coronary artery bypass grafting and was discharged on optimal medications.
Discussion
Inflammation and calcification play important roles in the pathophysiological progression of atherosclerosis. In the early phase of atherosclerosis, inflammation plays a predominant role in plaque progression. 1 The repeated wear and tear of the process leads to calcification of the vessel walls. The extent of vessel wall calcification provides a clue regarding the clinical prognosis. 2 There are two types of calcifications―Macro and Micro―macrocalcification signifies a stable stage, whereas microcalcification signifies instability, risk of plaque rupture, and increased cardiac events. To identify the microcalcification, imaging has been used as a screening tool for initiating preventive measures in intermediate to high-risk individuals. There is robust evidence, regarding the CAC as a marker of plaque burden and independent prognostic value.3–5
The CT coronary angiography (CAG) is the gold standard for the detection of CAC. Apart from the luminal extent, the advantage lies in the detection of adventitial calcium, spotty calcification, and positive remodeling of the wall compared to conventional angiography. Chest X-ray has a low sensitivity in detecting them (42%). 6 A radiographic triangle yielding high detection of CAC has been defined with borders of vertebral column medially, heart border laterally, and an imaginary horizontal line at one-third of the distance between the left bronchus and the diaphragm along the left heart border inferiorly (CAC triangle).7, 8 Of the coronaries, LAD is the most common to be calcified (93%) followed by LCX (77%) and then the RCA. 9 The proximal segments calcify more than the distal segments. A low KVp is required while doing CT imaging for detection of the calcification, as a high KVp will lead to blooming artifacts.
Conclusion
Coronary artery calcification is a marker of severe atherosclerosis. The usual diagnostic test of choice for identification is CT angiography or invasive angiography. Its identification on chest X-ray is rare and hence being presented.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.