
Abstract
Coronary cameral fistula (CCF) is an uncommon congenital anomaly that is typically discovered incidentally or may manifest with symptoms of angina. We present a case of CCF originating from the right coronary artery (RCA) and extending to the main pulmonary artery (MPA), characterized by aneurysmal dilatation at the pulmonary artery end. The patient presented with angina and exhibited ischemic changes in the inferior leads on electrocardiography. Additionally, the patient had coexisting stenosis of the left anterior descending artery (LAD). Consequently, the patient underwent a successful surgical closure of the fistula, along with surgical revascularization of the LAD.
Keywords
Introduction
Coronary cameral fistula (CCF) is relatively rare, occurring in up to 0.2% of angiographic studies. 1 CCF refers to an anomalous connection between the coronary artery and the heart’s chambers. The right coronary artery (RCA) (55%) is most commonly involved. CCF can be detected incidentally on angiography or can present with various symptoms.
Diagnosis and Treatment Plan
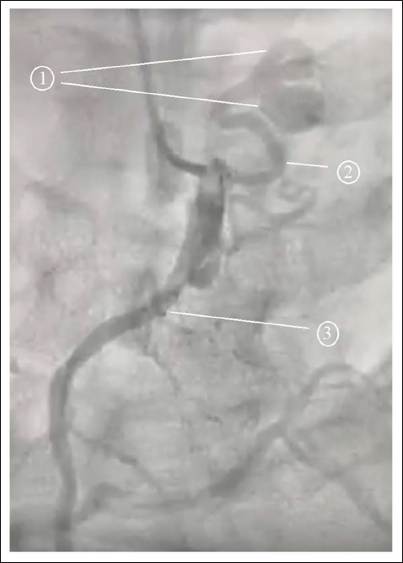
A middle-aged man of 50 years old presented with stable angina, which had been persisting for two weeks. Electrocardiography showed ST depression in inferior leads. A coronary angiogram revealed CAD involving left anterior descending artery (LAD) associated with a CCF between the conus branch of the RCA and the main pulmonary artery (MPA) (Figure 1). The patient underwent successful surgical closure of the fistula and surgical revascularization of LAD.
The angiographic picture of the CCF. (1) Aneurysmal hood, (2) CCF, (3) RCA.
Treatment Progress
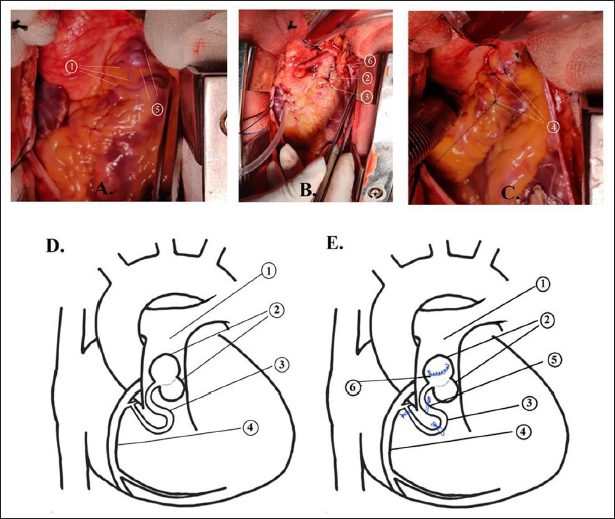
Mediastinum was accessed via median sternotomy. A tortuous vessel connecting the conus branch of RCA to MPA was observed with aneurysmal dilatation of the fistula at the MPA end (Figure 2). This tortuous vessel was interrupted at multiple sites with 4-0 polypropylene. The aneurysm was opened and the opening into the MPA was secured. Coronary artery bypass surgery was carried out under cardiopulmonary bypass and cardioplegic arrest, involving the use of the left internal thoracic artery for the LAD and a saphenous vein graft for the D1 branch.
Intraoperative photographs of the CCF. (A) Before surgery. (B) After surgery. (C) Magnified view of the operative site. 1-CCF, 2,3,4- interruption of fistula at multiple points, 5- aneurysmal hood, 6- the opening of fistula into MPA. An illustration of the CCF. (D) Before surgery. (E) After surgery. 1- MPA 2- aneurysmal hood, 3- CCF, 4- RCA, 5- fistula interrupted at three locations, 6- opening of the fistula over MPA closed with sutures.
Treatment Outcomes
The patient experienced a smooth postoperative recovery and was discharged home on the fifth day after the surgery without any complications.
Discussion
CCFs typically remain asymptomatic and are usually diagnosed during childhood when symptoms of congestive heart failure or infective endocarditis become apparent. The presentation of CCF with angina in adults is generally due to coronary steal that may be aggravated by concomitant CAD in other coronaries.
A definitive diagnosis of CCF is usually made through angiography. If large enough, it can also be detected on echocardiography, but this is operator dependent. Advanced imaging studies like multi-detector computed tomography or cardiac magnetic resonance imaging can be employed to detect the precise anatomy, flow, and function of the lesion.
The management depends upon various factors like the origin, size, and extension of the fistula, and various patient factors (age, symptoms, hemodynamic compromise, complications, and concomitant conditions). Small fistulas can usually be followed-up with regular imaging, whereas larger and symptomatic fistulas need intervention. The options for management include surgical ligation or interventional closure using coil embolization, detachable balloons, or vascular plugs, with a lack of data showing the superiority of one over the other. Excessive tortuosity of the fistula, aneurysmal dilatation, and multiple openings of the fistula can preclude interventional closure, as in this case. Due to its tortuous nature, aneurysmal dilatation, and associated CAD that needed surgical revascularization, this patient underwent surgical management. Mavroudis et al. 2 and Cheung et al. 3 reviewed long-term follow-up of surgical correction of CCF, revealing that surgical ligation was a safe procedure with a recurrence rate of 10%. In a comparative study, Armsby et al. 4 examined a cohort of 33 patients who underwent successful transcatheter occlusion of CCF and found no significant differences in outcomes and complications when compared to published surgical reports.
Conclusion
Patients with CCF presenting with excessive tortuosity, aneurysmal dilatation, and associated significant CAD should preferably undergo surgical management.
Footnotes
Ethical Approval
The case report was approved by the Institutional Ethics Committee (REC number: ECR/353/Inst/AP/2013/RR-19).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.