
Abstract
Extensive myocardial dystrophic calcification is rare and indicates a poor prognosis with a risk of arrhythmia and recurrent heart failure. We present a long term survivor of extensive myocardial infarction presenting as myocardial calcification related unstable ventricular tachycardia needing an implantable cardioverter defibrillator.
Case Summary
A 67-year-old hypertensive gentleman, with a history of anterior wall ST elevation myocardial infarction, thrombolyzed with streptokinase 15 years earlier, underwent elective bare metal stent in the right postero-lateral ventricular branch. He had moderate left ventricular systolic dysfunction and was kept on medical management for moderate lesions in left anterior descending and left circumflex coronary arteries.
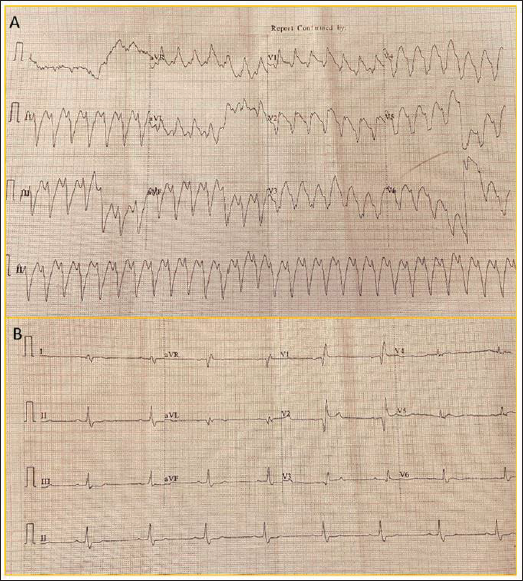
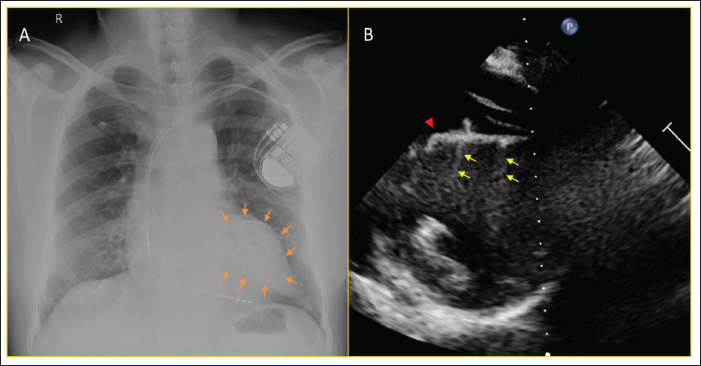
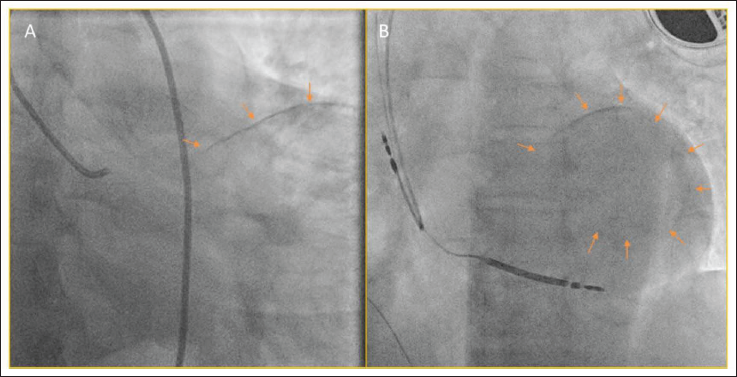
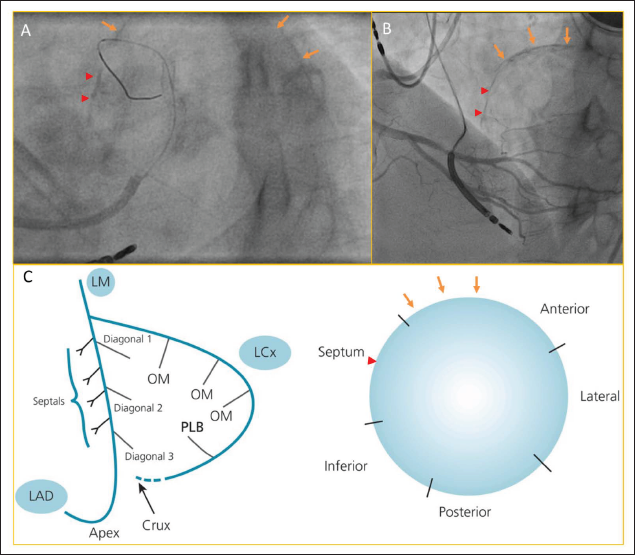
Now he presented with hemodynamically unstable ventricular tachycardia (VT) which was terminated with 200J of direct current cardioversion (Figure 1A). The baseline electrocardiogram showed bifascicular block (Figure 1B). His troponin T and NT-proBNP were elevated. Cardiogenic shock improved with conservative management. Chest X-ray showed a round calcific ring on the left side of cardiac silhouette (Figure 2A). The echocardiogram revealed dilated left ventricle, severe systolic dysfunction with thinning and akinesia of anterior and apical segments of left ventricle along with a hyperechoic probable calcific rim of lesion along endocardial border with backscatter reflections (Figure 2B, Supplementary videos 1 and 2). During coronary angiogram, fluoroscopy confirmed the presence of rim of dystrophic calcification of the likely non-viable myocardium (Figure 3A, 3B). Localization and its schematic depiction have been given in Figure 4A–C, Supplementary videos 3 and 4. Electrocardiogram during VT having north-west axis, small r and deep S in V6 with right bundle branch block pattern in V1 also suggested VT exit from left ventricular apex. Coronary angiogram showed left main shaft severe stenosis with significant in-stent restenosis of right coronary artery stent. He underwent dual chamber implantable cardioverter defibrillator (ICD) and angioplasty for left main coronary artery and right coronary lesion. Myocardial dystrophic calcification in long term survivors of myocardial infarction has been reported. 1 It is associated with poor prognosis. The calcifications correspond to areas of un-excitability and represent a fixed boundary of re-entry circuits acting as substrate for scar related re-entrant VT.2, 3 Although it indicates likely non-viable myocardium, our decision to re-vascularize left main coronary artery was to protect the left circumflex territory. This case emphasizes that dystrophic myocardial calcification, which can sometimes be picked up in routine chest X-ray, can cause scar-related VT. Although cardiac CT or magnetic resonance imaging would have given better idea of the extent of involvement, it could not be done, which was a limitation of this report.
A. Wide-complex Tachycardia with North-west Axis Suggesting Ventricular Tachycardia; B. Post-termination Sinus Electrocardiogram Showing Prolonged PR Interval With Right Bundle Branch Block.
A. Chest X-ray Showing a Round Calcific Ring (Arrows) in Left Cardiac Silhouette, Post-ICD Implantation; B. Echocardiogram in Modified Short Axis Apical View Showing Hyperechoic Probable Calcific Rim (Arrowhead) Along Endocardial Border of Left Ventricle with Backscatter Reflections (Arrows).
Plain Fluoroscopy Confirming the Presence of Calcific Round Shadow with Well Circumscribed Border Due to Dystrophic Calcification of the Likely Non-viable Myocardium.
A. LAO 38°, Caudal 33° View Showing Apical LAD Territories are Calcified, Arrowheads and Arrows Indicate Septal and Anterior Wall Calcification respectively; B. LAO 40°, Cranial 10° View Showing the Same; C. Schematic Depiction of the Walls Involved and Probable Location of the Calcification Has Been Marked in LAO, Cranial View. LAO - Left anterior oblique.
Footnotes
Author Contribution
SM (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead); RRR (Conceptualization: Equal; Investigation: Equal); HKS (Investigation: Equal; Supervision: Equal; Validation: Equal).
Consent
The authors confirm that consent for submission and publication of this case report has been obtained from the patient in line with COPE guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.