
Abstract
Carcinoma of lung (CoL) is the fourth most common cancer in India. It is classified as either small-cell or non-small-cell lung cancer, with adenocarcinoma being the most common variant. CoL can present either as paraneoplastic or non-paraneoplastic manifestation. We discuss a case of a patient who had an abrupt onset of sustained ventricular tachycardia and was subsequently diagnosed with metastatic non-small cell lung cancer with no cardiac infiltrates.
Keywords
Learning Points
Ventricular tachycardia (VT) can be the only presentation of asymptomatic lung carcinoma.
To the best of our knowledge, this is the first case of carcinoma of lung (CoL) reported with VT presentation.
Arrhythmia can be caused by paraneoplastic syndrome of lung cancer.
VT in CoL could predict poor outcomes.
Introduction
Carcinoma of lung (CoL) accounts for 5.9% of all cancers and 8.1% of cancer-related deaths in India. CoL is the fourth most frequent cancer in India and also the leading cause of cancer among males. 1 Histologically CoL can be divided into small-cell and non-small-cell-type lung carcinoma. Adenocarcinoma (a non-small-cell variety) is the most common among CoL and constitutes 36% of cases. Approximately 6.5% of cases are asymptomatic and are detected incidentally, the majority of them in advanced stages. 2 CoL manifestations have been classified as thoracic, extra-thoracic, and paraneoplastic syndromes. The cardiac manifestation is classified as a thoracic manifestation mostly due to metastatic infiltration of the carcinoma into the cardiac tissue. There are few cases of nonsustained ventricular tachycardia (NSVT) described among patients with CoL in the past that had definite cardiac infiltration.3, 4 We describe a case of sustained ventricular tachycardia (VT) in poorly differentiated adenocarcinoma of the lung detected incidentally, with no cardiac metastatic infiltration of any sort.
Case Presentation
A hypertensive male of 63 years suffered from intermittent, transient palpitations lasting for 2 months which were treated symptomatically at a local clinic. He then presented to the emergency room with sudden onset, persistent palpitation, and symptoms of presyncope. His vitals showed tachycardia with a thready pulse, hypotension of 96/62 mmHg, tachypnoea of 45/minutes, was afebrile.
Investigations
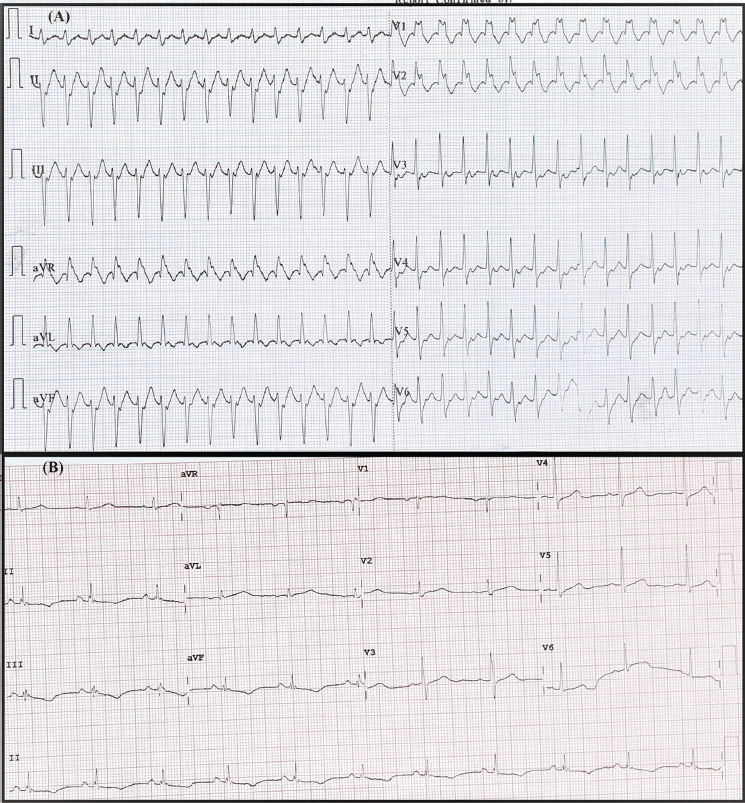
His electrocardiogram (ECG) showed broad complex tachycardia of 182 rate/minute, with right bundle branch block (RBBB) morphology and wide QRS duration of approximately 140 milliseconds (Figure 1A). This RBBB morphology is associated with left axis deviation and R>R’ (rabbit ear morphology). The ECG changes mentioned above aroused the possibility of VT vis-a-vis supra-VT with aberrancy. Echocardiography showed good left ventricular function. Other blood-related workups showed normal hemoglobin of 11.7 g/dL, normal white blood cells of 9.2 × 109/L, normal platelet count of 186 × 109/L, normal serum creatinine of 0.9 mg/dL, low albumin levels of 3.0 gm/dL, normal serum globulin of 2.1 gm/dL, high serum C-reactive protein of 2.0 mg/dL, erythrocyte sedimentation rate of 14 mm/h, normal highly sensitive troponin I of 10 ng/L, normal thyroid profile with the thyroid-stimulating hormone of 3.5 mU/L, normal serum sodium of 137 mEq/L, normal serum magnesium of 0.9 mMol/L, normal serum potassium of 4 mMol/L, normal serum calcium of 2.3 mMol/L and normal angiotensin-converting enzyme levels of 20 nanomoles/milliliter/minute.
Electrocardiogram Showing Broad Complex Tachycardia With Right Bundle Branch Block and Left Axis Deviation (A). Image showing electrocardiogram with narrow complex tachycardia with T-wave inversion in inferior leads.
Differential Diagnosis
The differential diagnosis of initial ECGs would be VT or supra-VT with aberrancy.
Treatment With Outcome and Follow-up
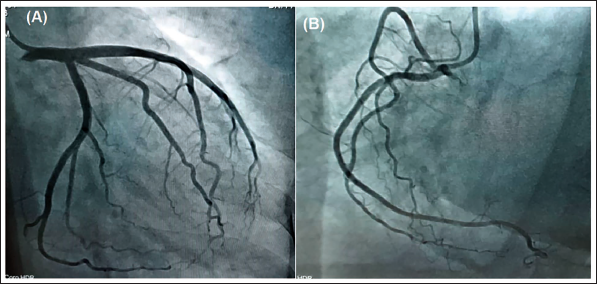
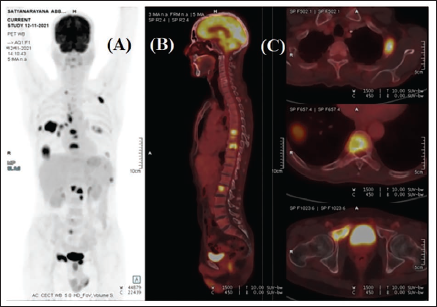
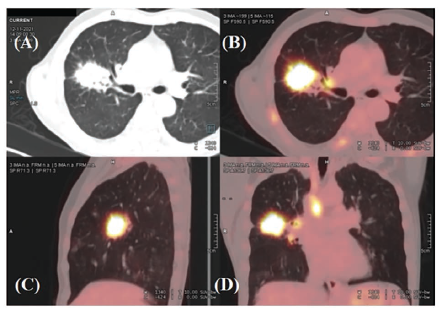
The patient was immediately started on amiodarone 150-mg bolus dose followed by slow infusion for 26 hours along with intermittent intravenous magnesium sulfate infusion of 1 g twice daily. Following this, the rhythm reverted to sinus rhythm (Figure 1B). He was started on bisoprolol of 2.5 mg twice daily, atorvastatin of 40 mg once at night, dual anti-platelet therapy (DAPT) of aspirin 75 mg, and clopidogrel of 75 mg in view of suspicion of coronary artery disease (CAD). He underwent a coronary angiogram which revealed mild CAD with mild plaques in proximal left anterior descending artery with no flow-limiting disease (Figure 2). His DAPT was de-escalated to a single anti-platelet of aspirin 75mg once daily with atorvastatin of 20 mg once daily He underwent cardiac magnetic resonance imaging which showed no late gadolinium enhancement of the myocardium (Videos 1 and 2), but MRI showed a lobulated parenchymal mass lesion in the right upper lobe of the with right hilar and pre-carinal adenopathy. A positron emission test (PET) with computed tomography (CT) confirmed the MRI finding and showed heterogeneously enhancing soft tissue density mass lesion measuring 3.6 cm × 3.8 cm × 3.1 cm with intense heterogeneous FDG uptake with another smaller mass lesion in anterior, basal segments of the lower lobe of right lung measuring 2.2 cm × 6.8 cm × 2.6 cm. Other metastatic lesions were noted in mediastinal nodes, bilateral ribs, multiple dorso-lumbar vertebrae, and pelvic bones (Figures 3 and 4).
Coronary Angiogram Showing Left the Dominant System With Mid-Left Anterior Descending Artery Showing Mild Atheromatous Plaque With No Flow-Limiting Lesion (A). The image shows a nondominant right coronary artery.
Whole-Body Positron Emission Test Showing FDG Uptake in Anteroposterior (A) and Lateral Views (B). The image shows metastasis to ribs and vertebral bodies (C).
Positron Emission Test With Computed Tomography Showing Right Upper Lobe Lobulated Lesion With FDG Uptake (A-C) and Mediastinal Metastasis (D).
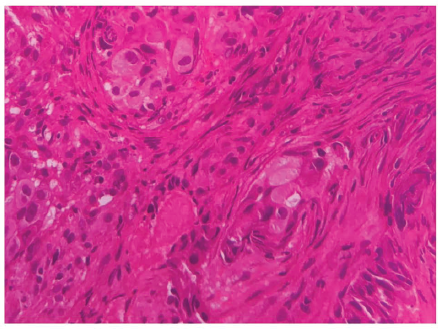
Endo-bronchial ultrasonography (EBUS) was performed to obtain a biopsy which showed polygonal cells with hyperchromatic round nuclei amidst desmoplastic stroma indicating poorly differentiated adenocarcinoma on histopathology (Figure 5). An epidermal growth factor receptor (EGFR) mutation analysis detected L858R (exon 21) mutation. The patient was started on Erlotinib for medical treatment and is symptomatically better.
Histopathology of the Lymph Node Biopsy Obtained By Endo-Bronchial Ultra-Sonography Showing Polygonal Cells With Hyperchromatic Round Nucleus Amidst Desmoplastic Stroma Indicating Poorly Differentiated Adenocarcinoma.
Discussion
Rhythm abnormalities are commonly seen in patients with neoplastic pathology of the lung in the background. The presence of arrhythmia suggests cardiac infiltration from lung neoplasia. Anker et. al showed arrhythmias (particularly NSVT) are common among cancer patients when compared to controls (8% vs 0%). 4 The same author showed that the presence of NSVT in any cancer could predict long-term mortality among cancer patients. The occurrence of VT in neoplasia of the lung is rare and moreover, arrhythmia occurrence in the absence of direct cardiac infiltration by neoplastic cells is unheard of. Our case presented as VT, which reverted to sinus rhythm after 26 hours of amiodarone infusion. The subsequent evaluation showed that the patient had poorly differentiated adenocarcinoma with metastasis. However, PET-CT showed no cardiac infiltration. Also, we ruled out all the common causes (ischemic heart disease, dilated/hypertrophic cardiomyopathy, myocarditis, sarcoidosis) of VT with the help of blood reports, ECG, coronary angiogram, cardiac MRI, and PET-CT imaging. Further molecular biochemistry of the lymph node biopsy from EBUS showed EGFR (L858R) mutation-positive. We hypothesize that the cardiac presentation of VT for the patient is possibly secondary to the paraneoplastic manifestation of lung carcinoma. This hypothesis assumes the possibility of role activation of EGFR ligands and EGFR-like ligands in the neoplastic manifestation of VT in CoL. The exact mechanism of signal pathway activation by EGFR ligands and EGFR-like ligands is not known. The effect of such signal pathway activation on the cardiovascular system is also not known completely. 5 Blood pressure regulation, endothelial dysfunction, neointimal hyperplasia, atherogenesis, and cardiac remodeling have all been linked to EGFR activation. Furthermore, elevated levels of circulating EGF-like ligands may play a role in the faster progression of vascular disease associated with chronic inflammation. 6 There is a possibility of either chronic inflammation or EGFR-like ligand-causing VT in our patient. This possible mechanism can be categorized as a paraneoplastic manifestation of the CoL. Our case is remarkable in several respects, including the fact that it is the first example of lung cancer presenting as VT to our knowledge, and there is no cardiac metastatic infiltration, pre-existing cardiac etiology, or metabolic rationale for VT causation. A long-duration follow-up of the patient will reveal whether VT like NSVT could predict long-term mortality in our patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance has been taken before submitting the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient’s attenders were informed and a detailed consent was taken for publication of the patient data.
Perspective of Patient
30 days ago: I started having a feeling of racing of heartbeat lasting a few seconds, for which a local doctor prescribed me some quite effective antacids.
Day 0: I started having palpitations with excessive sweating and a feeling of giddiness since morning. I was taken to the hospital, where they did some initial evaluation and told me that my heart rate was quite high and I need to be admitted. I was started on multiple injections and shifted to ICU.
Day 1: After many hours of injections my discomfort reduced and I could feel a sense of relief. I was later that day told that all this could be due to heart blocks so I need to undergo some tests.
Day 2: Doctors performed my angiogram and told me that it was near normal and the possible cause for my rapid heart rate could be a fault in the electrical system of the heart for which they performed MRI scan. I was quite relieved that my blood supply to heart was normal
Day 3: The doctors shifted me to the ward where they told me that the heart was quite normal but they found some abnormal mass in my lungs. And they asked me to undergo further tests. This jolted me again as to what worse is awaiting me.
Day 4: I underwent a PET scan that day
Day 5: I was told that I am suffering from possible lung cancer and a biopsy will be required to know the type of cancer. It was devastating but my family members gave me strength. I gave my consent for further evaluation.
Day 6: I underwent endoscopy after they sedated me. Later that evening I woke in ICU and I was told that the procedure happened as per plan and a biopsy was taken.
Day 9: I was discharged and told to come to OPD for further management.
Day 18: I went to a medical oncologist where he told me that there is medical management for the condition and for now oral tablets will be started and monitored for progress.