
Abstract
A high-grade stenosis of the inferior vena cava (IVC) can cause swelling, discoloration of the lower extremities, and the development of venous ulcers. These patients may be unable to participate in physical activities as well. Although anticoagulation and compression therapy may help alleviate symptoms and prevent repeated thrombosis, few patients develop progressive symptoms.
We present a case of an elderly female who had progressive venous claudication, edema, heaviness, and discoloration of both lower limbs. Despite endovascular laser therapy for varicose veins, the symptoms worsened, jeopardizing her quality of life. Endovenous intervention with a stent to treat high-grade stenosis at the junction of the suprahepatic IVC and right atrium (RA) could completely relieve her symptoms and improve her quality of life.
Isolated severe stenosis of the IVC at the confluence with the RA is a rare cause of chronic venous congestion. Its leads to refractory venous congestion with secondary skin change with an adverse impact on quality of life. Endovenous intervention using an appropriate endovascular prosthesis is the treatment of choice.
Introduction
It is uncommon to have chronic non-malignant high-grade stenosis of the suprahepatic segment of the inferior vena cava (IVC). Endovascular recanalization using balloon angioplasty and self-expanding stents for non-malignant symptomatic venous obstruction is practically demanding; yet, treatment is safe and durable. stent implantation for persistent IVC stenosis/occlusion has been described in just a few limited case studies and individual cases.1–4 In a retrospective analysis by Erben et al. projected patency rates of IVC stenting at 36 months were more than 85%, with good clinical outcomes. 4 We present a case of idiopathic stenosis at the junction of the suprahepatic IVC and the right atrium (RA), which resulted in symptoms of chronic venous congestion in both lower limbs. For persistent non-malignant IVC stenosis, we performed endovenous intervention with an appropriate stent rather than open surgical surgery.
Case Report
A 66-year-old female with hypertension reported to the outpatient clinic with a 6-month history of progressive swelling and stiffness in both lower limbs. She received endovascular laser therapy for varicose veins in both legs two years ago. Since then, the leg symptoms have steadily deteriorated, including calf hardness, redness, and a local rise in temperature. Walking was difficult because of leg heaviness. There was evidence of lipo-dermato-sclerotic alterations with brownish discoloration and non-pitting pedal edema below the knees on inspection. There are a few varicosities around the ankle defined as “corona phlebectatica.” Due to edema, bilateral pedal pulses were not perceptible, although biphasic signals were detected. Her vital signs and test results were unremarkable (Figure 1). The revised Venous Clinical Severity Score (VCSS) of our case before treatment was 13. 5

Our patient had a revised VCSS of 13 prior to therapy. (Pain – 2; Varicose veins − 1; Venous edema – 2; Skin pigmentation – 2; Inflammation – 2; Induration – 2; Active ulcer − 0; Use of compression therapy – 2).
The initial ultrasound and venous Doppler examination of both lower limbs revealed compressible popliteal veins with occluded treated GSV but no signs of deep vein thrombosis. Her local practitioner suggested she take antibiotics for potential cellulitis, which did not improve her problem. Additionally, an ultrasound of the abdomen showed a small defect in the suprahepatic portion of the IVC without any significant collaterals with normal liver size and echotexture. No other intraabdominal abnormality was found. Lymphedema was also suspected, and patients were advised to undergo lymphoscintigraphy before beginning compression therapy. It revealed normal lymphatic drainage of both lower limbs (Figure 2A).
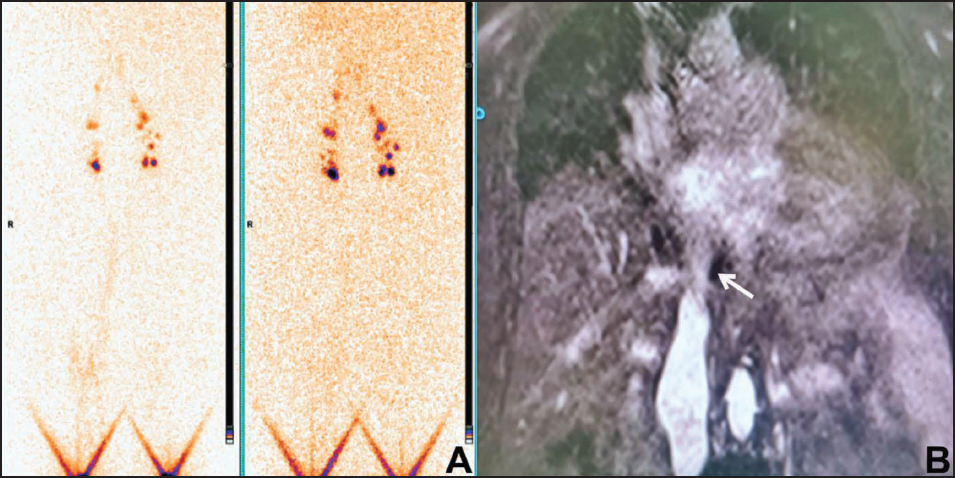
A vascular surgeon recommended MRI venography of both lower limbs as there was no relief of her symptoms despite compression therapy, which revealed a focal area of moderate to severe abrupt luminal narrowing of the hepatic segment of IVC distal to the confluence of hepatic veins with a small intraluminal hypo intensity suggestive of partial obstruction to the hepatic segment of IVC due to stricture or membrane (Figure 2B, Video 1). Routine screening for malignancy and hypercoagulable states were unremarkable.
She was then suggested to undergo catheter cacography for additional assessment. The right femoral vein was cannulated using 5 Fr. Femoral sheath and 20 ml of contrast injection demonstrated a membrane-like severe stenosis of suprahepatic IVC-RA junction (Figure 3A). Also, there was a mean pressure gradient of 10 mm Hg across the stenotic segment Mean IVC pressure distal to the stenosis – 15 mm Hg and Mean RA pressure – 5 mm Hg). Following a thorough review of the case, the CEAP classification (Clinical-Etiological-Anatomical-Pathophysiological) was C3, 4a, 4b, S (Edema, Pigmentation, lipodermatosclerosis, Symptomatic); En (absence of identified venous aetiology); AD6 (deep venous system involving IVC); Pn (unidentified venous pathophysiology); and L III (Level of investigation – Invasive). 6 Therefore, we intended to perform endovenous intervention using a novel endoluminal prosthesis.
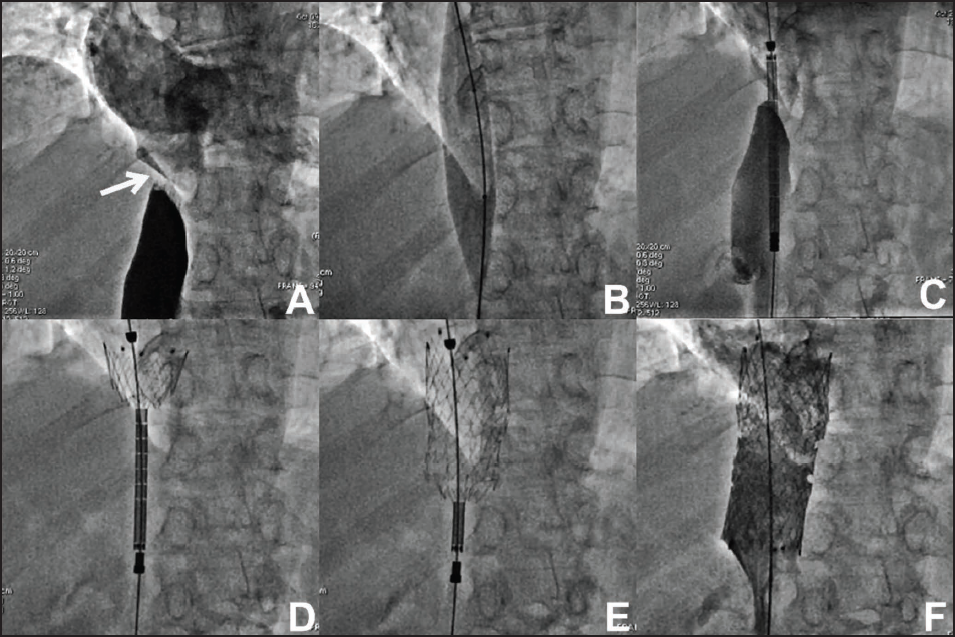
The right femoral vein was cannulated with 14 Fr. sheath after adequate pre-dilatation using graded dilators. The IVC lesion was crossed with 0.035” Terumo guidewire which was exchanged with Amplatz super stiff guidewire. It was predicted using an 18 × 40 mm Atlas balloon at 6 atmospheres pressure for 20 sec (Figure 3B). The lesion was stented with a 28 × 70 mm ‘mc-a’ (Medicut Stent Technology GmbH, Pforzheim, Germany) self-expandable nitinol stent (Figure 3C−E). There was improved cardiac hemodynamic documented with no residual gradient or stenosis across the IVC-RA junction with normal venous flow (Figure 3F, Video 2).
The patient was discharged on 2nd-day post-procedure with the advice of dual antiplatelet therapy in the form of aspirin and clopidogrel, antihypertensive medications, amlodipine 5 mg once daily, and atorvastatin as she had nonobstructive coronary artery disease. She has a complete 6-month follow-up with complete relief of her symptoms with improvement in walking distance.
Discussion
A multitude of aetiopathogenesis may lead to high-grade stenoses of the IVC, including hypercoagulability, vasculitis, traumatic injury, external compression, and iatrogenic causes. Patients’ levels of physical activity and lifestyle may influence the onset of symptoms. 3 In our situation, the patient came with edema of both lower limbs, resulting in significant disability in everyday physical activities. Raju et al. observed 97 individuals (99 lower extremities) in the chronic symptoms group had symptoms of chronic venous disease ranging from mild to severe in one of the largest data sets of obstructive lesions of the IVC. One-third of patients had symptoms in both limbs. 14% of the patients had a complete occlusion and the remainder had stenoses of the IVC at various levels. 2
Further testing using contrast-enhanced MR venography indicated the existence of high-grade membrane-like stenosis of the IVC, which is treatable with endovascular angioplasty and stenting. Such observations are best made on coronal views. To determine the level of disease involvement and the proper diagnosis, we use contrast-enhanced MR venography to examine the native venous system in its entirety. Diagnostic catheter venography was conducted to aid in the design of the endovascular operation and to determine the hemodynamic significance of the stenosis.
Endovascular therapy of persistently blocked IVC has been the subject of multiple case series published since the early 2000s.1–4, 7 Endovascular therapy of symptomatic patients with persistent non-malignant IVC blockages was something we wanted to look at from the perspective of our institution. The use of venous stents has also been reported in patients with Budd-Chiari syndrome as well as in those who have developed obstruction due to caval anastomotic narrowing, kinking, or torsion following liver transplantation. 7 In the latter case, the patency rate has reached 90% after seven years. Stent implantation in the IVC was effective in 19 of 20 patients, with primary patency after 24 months at 67% and secondary patency at 83%, according to Grøtta et al. 1 These positive outcomes have prompted us to turn to endovascular treatment options for chronic venous high-grade stenosis of the IVC.
The characteristics of the IVC wall have a significant impact on the risk of stent misplacement/migration, and the immediate increase in venous return following vena cava stent implantation may alter cardiac contractility by raising preload. 8 Consideration of local anatomy and lesion features is essential when designing a stent in order to reduce the risk of migration or protrusion into the RA. 9 This suprahepatic IVC stenosis at the RA confluence has no specialized or approved devices, however, existing stents may be considered for off-label use. We required a stent with more radial force and reliable foreshortening, these designs are more effective. Even more comprehensive covering may be required for the larger-diameter, longer, and more dynamic environment of the IVC, particularly for stents that are not barbed.
Wallstents have the benefit of being widely accessible in large diameters and nominal lengths, but they are prone to displacement and need repositioning. Another issue with these stents is that unpredictability in shortening and ends with no continuous wire interweaving lead them to stretch and foreshorten well beyond their specified size.8, 10 As a result, we needed a secure implantation with an ‘mc-a’ stent, despite the fact that the local anatomy provided a significant risk of migration. It has a self-expanding nitinol stent, a flexible stent design, and a closed-cell architecture for enhanced fixation. 11
Conclusion
Idiopathic high-grade stenosis of the IVC may have a serious influence on the quality of life of an older age group. Because of substantial vein wall thickening, they are not suitable for simple angioplasty and must be treated with IVC stenting and re-creation of IVC-RA confluence to preserve patency. Endovenous stenting is safe, with hardly any associated morbidity, and reintervention rates are low in the midterm follow-up. Though a longer period of observation is required to determine its long-term durability, the functional outcomes are promising, with the majority of patients able to resume their normal daily activities.
Footnotes
Authors’ Contributions
PJ was the primary consultant of the case and drafted the manuscript. VJ was engaged in the intervention, while VRJ is the case’s referring physician.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent to Participate
Informed consent was obtained from a patient for education purposes including data and images unless her identity was not revealed. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Written Consent for Publication
This manuscript has not been submitted to any journal before for publication as a part or complete version. I give complete consent and rights to the journal for its publication.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.