
Abstract
Cardiac amyloidosis is an increasingly recognized cause of heart failure. It remains underdiagnosed despite a significant morbidity and mortality rate. The mean survival in patients with cardiac amyloidosis is less than 1 year in untreated primary light-chain amyloidosis and less than 4 years in wild-type transthyretin amyloidosis. We report a unique case of a 78-year-old male with transthyretin cardiac amyloidosis, who presented with persistently elevated troponin and progressive heart failure unresponsive to conventional therapy. With this case, we would like to highlight the role of cardiac biomarkers in the early diagnosis of cardiac amyloidosis.
Introduction
Amyloidosis is an abnormal localized or systemic deposition of insoluble protein fibrils in the extracellular space prompting tissue and organ dysfunction. 1 The heart is among the most widely recognized solid organs involved in systemic amyloidosis usually due to light-chain protein fibril (AL) and transthyretin fibril (TTR) deposits. 1
Cardiac amyloidosis (CA) remains underdiagnosed despite a high fatality rate. 2 It is also known for mimicking other cardiovascular diseases, including congestive heart failure (CHF). 3 It is an increasingly recognized cause of heart failure (HF) with a prevalence of 13% among patients with HF and preserved ejection fraction. 4 We present this case to highlight the role of cardiac biomarkers in the early diagnosis of CA.
Case presentation
A 78-year-old African-American male with a history of paroxysmal atrial fibrillation, syncope, hypertension, and HF with reduced ejection fraction of 30%–40% (diagnosed 2016) presented to the emergency department with increased exercise intolerance, episodic chest pressure, and shortness of breath. Other past medical history included stroke, chronic kidney disease, and small bowel obstruction. Home medications were rivaroxaban, beta blocker, statin, angiotensin-converting enzyme (ACE) inhibitor, and torsemide. The vital signs on arrival were normal. The physical examination was significant for a non-obese male with an irregular heartbeat, elevated jugular venous distention (6 cm above sternal angle), bilateral lower extremity edema, and inspiratory crackles. Cardiac auscultation did not reveal any extra heart sounds. Labs were significant for troponin I (TnI) of 0.27 ng/mL (normal < 0.03 ng/mL) and brain natriuretic peptide (BNP) of 389 pg/mL (normal < 100 pg/mL), both of which were higher than his known baselines (0.14 ng/mL and 300 pg/mL, respectively). Furthermore, chart review revealed a persistently elevated TnI (mean = 0.145 ng/mL) for approximately 10 years (5 years before his CHF diagnosis). All other labs, including kidney and liver function, hematology, and urine drug screen, were normal.
Chest X-ray revealed no acute cardiopulmonary abnormalities. Electrocardiogram (Figure 1) showed normal sinus rhythm with low voltage, but no signs of ischemia. The patient was admitted for management of non-ST elevation myocardial infarction (NSTEMI) and CHF exacerbation.

Electrocardiogram with low-voltage, left axis deviation, first-degree AV block.
Transthoracic echocardiography (TTE) (Figure 2) revealed a progressive decline in left ventricular ejection fraction (LVEF) to 25%–35%. It was also significant for worsening diastolic dysfunction with E/A of 3.5 and medial E/E′ of 24, despite the patient’s adherence to medical management. The initial TTE done 3 years prior to this presentation showed LVEF 50%–55% and mild diastolic dysfunction with E/A 0.78. The repeat TTE done 1.5 years later revealed a decline in LVEF to 30%–40%.

Top image on admission 04/17: image showing (a) concentric LVH with profound septal hypertrophy, (b) diastolic dysfunction on transmitral Doppler flow with E/A of 3.5. Bottom image on 09/18: increase myocardial echogenicity, (c) severe dilated left atrium, (d) restrictive filling pattern with grade III diastolic dysfunction.
Given the progressive decline in LVEF, a cardiac MRI (magnetic resonance imaging) was performed to rule out apical ventricular thrombi. The MRI revealed diffuse late gadolinium enhancement concerning for amyloidosis. Follow-up nuclear bone imaging (Figure 3) revealed increased cardiac uptake greater than bone, suggestive of grade III CA. Fat pad biopsy and mass spectrometry confirmed TTR amyloidosis. The patient was managed conservatively with diuretics, with significant improvement in symptoms, and was discharged with appropriate follow-up in place. Metoprolol was discontinued on discharge due to concerns of worsening the amyloidosis symptoms.
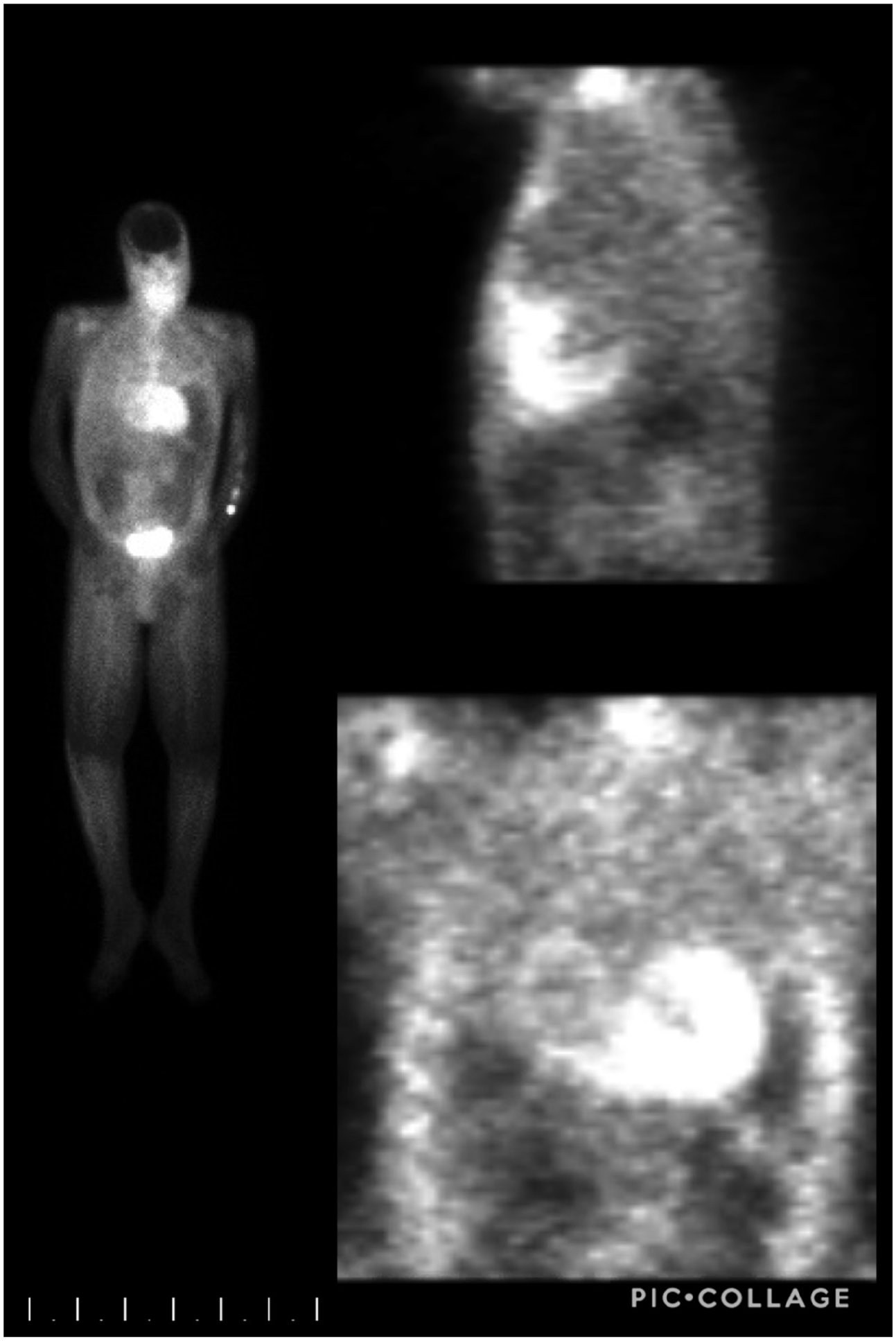
Technetium pyrophosphate NM bone scan spect reveals abnormal radiotracer uptake within the cardiac myocardium that is greater than bone uptake. Findings were characteristic of grade III cardiac amyloidosis. 5
Discussion
CHF is generally classified into two main categories: heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF). Based on current research, pharmacological therapies directed at HFpEF have not shown any morbidity or mortality benefit. 6 Thus, the treatment for HFpEF is mostly aimed at treating the underlying causes such as long-standing hypertension, obesity, coronary artery disease, chronic obstructive pulmonary disease, and diabetes mellitus. A rare and underdiagnosed cause of HFpEF is infiltrative cardiomyopathy, such as CA. However, studies have shown abnormal TTR protein on autopsy in 17% of elderly patients with HFpEF, which suggests that the etiology of HF had been misdiagnosed in many patients. 7
Patients with CA often present with similar signs and symptoms as those with decompensated HF. The electrocardiogram usually reveals low-voltage, poor R wave progression, and atrioventricular node conduction abnormalities. Low voltage combined with left ventricular hypertrophy, in particular, should always raise suspicion for infiltrative cardiomyopathies and prompt further workup. 8
Various imaging modalities can assist in the diagnosis of CA. As seen in our patient, diastolic dysfunction is usually one of the earliest findings on TTE (Figure 2). Common findings include decreased ventricular chamber size, bi-atrial enlargement, and ventricular hypertrophy, although they have been reported to be nonspecific or nonsensitive. 9 The addition of two-dimensional speckle tracking echocardiography has improved the diagnostic accuracy of the TTE. The presence of apical sparing regional longitudinal strain pattern greater than 2:1 ratio or increased LVEF to global longitudinal strain ratio greater than 4 is suggestive of CA. 10 Cardiac MRI can provide more precise analysis of cardiac function. Amyloid deposits in the myocardium can often be detected as patchy or diffuse late enhancement of gadolinium on t-1 mapping with a sensitivity of 85% and specificity of 92%.5,9 In addition, nuclear bone imaging with Tc-99m pyrophosphate can often demonstrate myocardial involvement in TTR CA (Figure 3) and provide information about disease severity based on a visual grading scoring system. 11 However, there have been questions about its sensitivity and specificity. 12 Traditionally, TTR CA diagnosis requires an endomyocardial biopsy, although it is not easily attainable and associated with increased risk of complications. 13 With the accuracy of these imaging modalities, there is now a general consensus for non-biopsy diagnosis for TTR CA. 14 The proposed diagnostic algorithm (Figure 4) recommends the combination of TTE and cardiac MRI with nuclear imaging with Tc-99m pyrophosphate or Tc-99m diphosphono-1,2-propanodicarboxylicacid, while evaluating AL amyloidosis with serum and urine electrophoresis.14,15 It is important to note that screening with serum and urine electrophoresis is insensitive, and AL CA can sometimes lead to increased cardiac uptake on bone scintigraphy. 15 Thus, nuclear imaging must be accompanied with serum and urine electrophoresis. Patients with abnormal results must be evaluated by the hematologist, and a cardiac biopsy should be considered. 15 In this context, nuclear imaging provides an excellent non-biopsy diagnosis for CA.

A proposed flow diagram demonstrates the critical requirement to exclude light-chain amyloidosis (AL) by serum and/or urine testing and concomitant use of nuclear scintigraphy to identify the presence of ATTRCM. It is emphasized that serum-free light chains and serum and/or urine immunofixation electrophoresis are the appropriate tests to exclude a monoclonal gammopathy, which also may be present in patients with ATTRCM. Nuclear imaging can also be performed concurrent to light-chain assessment, even in the case of a detected monoclonal gammopathy, for additive information.
Cardiac biomarkers such as highly sensitive cardiac troponin T (hs-TNT) and N-terminal pro-BNP have been proven to be of prognostic value in CA.16,17 The proposed mechanism for troponin leak includes cardiac myocyte damage from extracellular deposition of protein fibrils and increased myocardial strain. 17 In a study involving 102 patients with biopsy-proven CA, higher hs-TNT was closely associated with cardiac involvement. 17 Furthermore, another study conducted on 96 patients with CA showed that 73 were TTR CA. Elevated levels of hs-TNT were found to be suggestive of CA with a cut-off value of 0.0312 ng/mL (p < 0.001), a sensitivity of 74%, and a specificity of 76%, suggesting that hs-TNT can help differentiate CA from other etiologies of HFpEF. 18
In addition, persistently elevated troponin levels may be an early indication of cardiac dysfunction with CA. Kraemer et al. 19 reported a case of CA that was diagnosed after persistently elevated troponin for about an year, and our patient had persistently elevated troponin levels for approximately 10 years (6 years prior to his HF diagnosis) (Figure 5). This suggests that elevated troponins may play a role in the early diagnosis of CA.

Graph showing persistent elevation of troponin I (normal < 0.03 ng/mL). Point A denotes approximate time of HFpEF diagnosis. Point B denotes time of CA diagnosis.
Management of CA can be difficult. Overall treatment depends on the type of amyloid protein involved. In AL amyloidosis, the mainstay treatment is chemotherapy to halt disease progression. 20 Tafamidis, a benzoxazole derivative, appeared to be effective in TTR cardiomyopathy. In a recent study, Maurer et al. 4 demonstrated reduced all-cause mortality, quality of life, and hospitalization in patients who received Tafamidis compared to placebo.
HF in CA can be managed with salt restriction and loop diuretics. Torsemide and bumetanide are favored because of the bioavailability and potency. 21 Patients with CA have a small chamber size, resulting in a low fixed stroke volume. Therefore, medications such as beta blockers are not recommended as they may decrease stroke volume. In addition, ACE inhibitors/angiotensin-receptor blockers (ARBs) may worsen symptoms by provoking autonomic dysregulation. 22
Conclusion
Our case illustrates that serial cardiac biomarker monitoring can aid in the early diagnosis of CA. Persistently elevated troponin should prompt further investigation for other causes of cardiac dysfunction, despite normal LV function. Given that patients with CA may decline rather swiftly, more frequent echocardiograms may be necessary to monitor disease progression and prompt guideline-directed therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.