
Abstract
Aconite is a plant with deceptively beautiful flowers that contain a deadly cardiotoxin. Aconite toxicity presents with often fatal ventricular arrhythmias that are refractory to conventional antiarrhythmic medications. An electrical storm (ES) is an acute cardiac emergency that carries a high mortality. We report one such case of acute aconite toxicity presenting with ES that was managed successfully with hemodynamic support, overdrive pacing, and charcoal hemoperfusion with high-flux ultrafiltration.
Introduction
Aconite is a highly cardiotoxic alkaloid present in plants belonging to the Aconitum species. Patients with severe aconite toxicity present with fatal resistant arrhythmias that are difficult to manage due to the absence of a specific antidote.
Case Report
A 62-year-old male, with no prior medical history, had a history of sudden loss of consciousness at home after ingestion of an ayurvedic preparation (Giloysat & Swasari Ras) that he had acquired over the counter for a sore throat. At a nearby hospital, he had 8 episodes of monomorphic ventricular tachycardia (VT), requiring DC cardioversion (150 J, sync) following which he was mechanically ventilated, started on fluids and inotropes to combat shock, and shifted to our center where he developed 9 more episodes of monomorphic VT (Figure 1) necessitating DC cardioversion.

He was started on intravenous (IV) amiodarone and lidocaine infusions. Lab workup looking for the reversible cause of electrical storm (ES) did not reveal any potential causes. Serum potassium was 3.8 meq/l and iv potassium supplementation was done to maintain potassium levels between 5.0−5.5 meq/l. Baseline serum magnesium was 1.9 mg/dl. 2D Transthoracic echocardiogram revealed normal-sized cardiac chambers with global hypokinesia of the left ventricle (LV) and mild LV systolic dysfunction (LVEF = 50%).
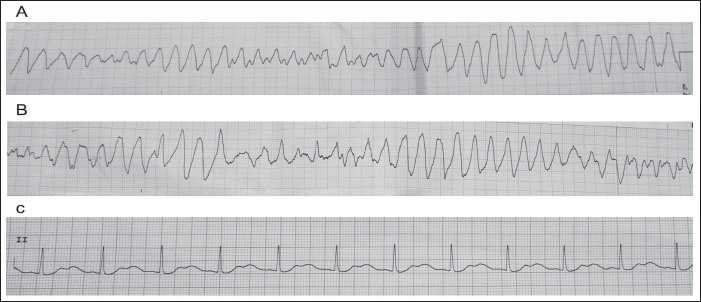
Four hours after admission he developed an episode of polymorphic VT (Figure 2A&B) with prolonged QT interval (Torsades de Pointes [TdP]) which was DC cardioverted due to hemodynamic instability and IV magnesium bolus was given. The baseline ECG post-cardioversion showed a prolonged QT interval with prominent U waves (Figure 2C). The patient had 8 more episodes of TdP thereafter. Isoprenaline infusion was started to maintain the heart rate above 100 beats per minute (bpm). Transcutaneous pacing was initiated at demand mode to pace at a minimum rate of 100 bpm.
On discussion with the ayurvedic physician, it was revealed that the preparation taken by the patient contained aconite. The patient had consumed 20 g of the preparation. The patient’s attendants denied any history of the patient having consumed any allopathic medications (antibiotics or antihistamines) concurrent with the ayurvedic preparation for his sore throat. A serum sample to screen for aconite was sent to the toxicology lab which came back strongly positive (qualitative test) for the presence of aconite in the serum. A quantitative test kit was unavailable at the toxicology lab and hence only a qualitative test was done.
Later, he developed asystole and was resuscitated as per ACLS protocol and pacing mode set to continuous mode at a rate of 110 bpm. Following this, he had two more episodes of monomorphic VT which were DC cardioverted with 100 J synchronized shock.
High flux ultrafiltration and charcoal hemoperfusion was done. The patient did not have any further episodes of VT or any other arrhythmia thereafter. External pacing was reduced to demand mode and isoprenaline infusion was reduced with a target heart rate of 90 to 100 bpm. Inotropes were gradually weaned off over the next 24 h. A second toxicology sample sent to the lab showed no significant circulating levels of aconite in the serum on qualitative testing. The patient was successfully extubated and taken off ventilatory support 48 hours after his last episode of VT and had no neurological deficits.
He was discharged in a stable state and a transthoracic 2D echocardiogram done prior to discharge showed good LV systolic function (LVEF = 65%). A year since the episode, he is doing well on regular follow-ups with normal LV function.
Discussion
Aconite, Monkswood, or Wolfsbane (Aconitum napellus) is an innocuous-looking plant with beautiful blue or purple flowers. It is classified as a cardiotoxic poison. The alkaloid toxins, mesoaconite, and hypoaconite are typically present in its roots and seeds. Many native non-allopathic preparations contain trace amounts of aconite. Typically the cardiotoxicity of aconite manifests as malignant ventricular arrhythmias. 1
The cardiotoxic effects of aconite and related alkaloids from the Aconitum species are mediated via high affinity binding to the voltage-sensitive sodium channels leading to the persistent activation of these channels, which become refractory to excitation. The electrophysiological mechanism of induction of arrhythmias is triggered activity due to delayed after-depolarization and early after-depolarization. Anticholinergic effects of aconite mediated via the vagus nerve also play a role in its arrhythmogenicity. Due to its activation of the ventromedial nucleus of the hypothalamus, aconite can cause hypotension and bradycardia. 2 Ventricular ectopy, tachycardia, and/or fibrillation often precede asystole. Conduction defects commonly seen include a widened QRS, a prolonged QT interval, and a bundle branch block. The toxic effects may manifest as early as 20 min to 2 h after ingestion. 3
ES is defined as “the occurrence of three or more distinct episodes of VT or ventricular fibrillation (VF) in 24 hours, requiring the intervention of the defibrillator (anti-tachycardia pacing [ATP] or shock).” Patients with ES are known to have a higher risk of all-cause mortality. 4
Polymorphic VT associated with a prolonged QT interval and characterized by a gradual change in the amplitude and twisting of the QRS complexes around the isoelectric line is known as TdP. TdP is refractory to DC cardioversion and may degenerate into VF. Magnesium is the drug of choice for the treatment of TdP in addition to the correction of etiological factors. Some authorities have recommended maintaining a potassium level towards the high normal range (5.0−5.5 meq/l) which is said to promote rapid repolarisation and prevent TdP. Isoprenaline, cardiac pacing and mexilitine to maintain heart rates of 90–100 bpm have a role in TdP with acquired prolongation of QT interval as bradycardia precipitates further episodes of TdP. 5
Management of aconite poisoning is predominantly supportive with therapy directed at the maintenance of hemodynamic stability with supportive management and cardiopulmonary bypass. Charcoal hemoperfusion has also been reported to be useful in management.1, 6
Aconite toxicity presenting as malignant arrhythmias have been scarcely reported in medical literature in a few cases reports from China and other eastern countries due to its use in Oriental medicine. Most of the cases that we reviewed had few ventricular ectcalcopics and one to two episodes of VT or hypotension. In our review of Indian literature done during the course of writing this report, this is the first reported case from India of Aconite toxicity presenting with ES and surviving to discharge.
We are reporting this case due to a rare etiology of a relatively common tachyarrhythmia seen in the ICCU. Cardiopulmonary bypass which is recommended as the front-line of therapy is often out of reach of the common populace due to costs or availability at many centers in developing countries like ours.
Our case highlights the successful management of a case of Aconite toxicity who presented with ES which in itself carries a dire prognosis. Our patient was managed with a combination of supportive therapy directed at maintaining hemodynamic parameters, prevention of ventricular arrhythmias by overdrive transcutaneous pacing as well as isoprenaline infusion and charcoal hemoperfusion with high-flux ultrafiltration. The use of charcoal hemoperfusion has only been rarely reported to be of use in such cases but we were able to use it successfully to clear the toxin from the bloodstream of this patient as was evidenced by the absence of any arrhythmias as well as the negative qualitative blood test for aconite post charcoal hemoperfusion.
Thus, even in the absence of cardiopulmonary bypass support such cases can be successfully managed in the ICU setting with timely intervention and hemodynamic support which can help tide over the acute crisis and aid in patient survival.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
Institutional Ethics Committee approval was obtained for the publication of this case report.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient for publication of this case report.