
Abstract
Stent under expansion is one of the reasons compromising the outcomes of percutaneous coronary interventions. The most common cause of the stent under expansion is calcium deposited in the atherosclerotic plaque. Adequate plaque modification is the paramount before the placement of a stent, as the options to handle under expanded stent are limited and less effective. In this case report, we explore the usage of knuckle wire for the extrastent plaque modification, after being failed with routine methods of handling stent under expansion.
Learning Objectives
If none of the available plaque modification techniques works, try extrastent plaque modification with extrastent knuckling technique.
Introduction
Stent under expansion compromises the outcomes of percutaneous coronary interventions (PCI) by increasing the incidence of target lesion revascularization. Adequate plaque modification to achieve the best possible final minimal stent area is paramount to reduce stent thrombosis or restenosis. 1 If a stent is placed and underexpanded, the options to expand it further are limited and less effective. Therefore, imaging guided adequate plaque modification before stent placement is the key in such scenarios.2,3 All methods of plaque modification rotablation, intravascular lithotripsy (IVL), OPN NC (ultra-high pressure noncompliant) balloon, and laser can be used in underexpanded stent with varying degrees of success. We report a case of underexpanded right coronary artery (RCA) stent in which knuckle wire is used for extrastent plaque modification after being failed with conventional methods.
Case
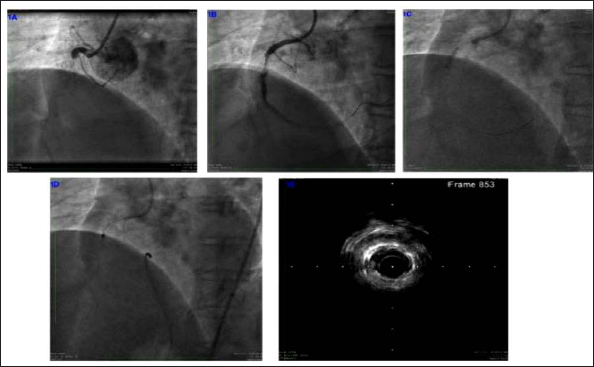
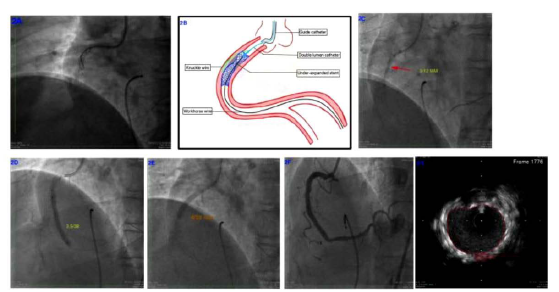
A 59-year-old, diabetic, and hypertensive male was presented to another hospital with acute coronary syndrome with unstable angina. Coronary angiogram (CAG) showed double vessel disease and PCI with stent to left anterior descending artery and RCA was performed. RCA stent was not expanded fully despite high-pressure noncompliant ballooning and OPN NC super high-pressure ballooning. Four weeks after the index procedure, he was presented with acute ST-elevations inferior wall myocardial infarction to our emergency. Check CAG showed a total cutoff of the proximal RCA from within the stent (Figure 1A). Thrombosuction was done, following which thrombolysis in myocardial infarction (TIMI II) flow was restored and the stent underexpansion was clearly visible with the stent appearing like hourglass (Figure 1B). Strategies to adequately expand the stent including high-pressure noncompliant balloon inflation (SIS Medical), 6 cycles of IVL (Figure 1C), and 1.5 mm burr rotablation (Figure 1D) were tried with no success. Intravascular ultrasound (IVUS) (Boston Scientific) showed a grossly underexpanded stent with the underlying fibrocalcific plaque (Figure 1E). Excimer laser coronary angioplasty was an option in this scenario, but we couldn’t use it due to nonavailability. Hence, we decided to use the knuckle wire technique of chronic total occlusion interventions to modify the extrastent plaque. Before using a knuckle wire, a safety wire was placed into the distal RCA through the center of the under expanded stent. Access to the extrastent plaque was achieved by scratch and go with a Pilot 200 wire (Abbott Vascular) through a double lumen catheter (Crusade; Kaneka Corporations) positioned proximal to the site of under expansion over the safety wire. As a result of gross stent under expansion, the Pilot 200 wire could be navigated into the extrastent plaque proximal to the site of underexpansion without much difficulty. Conventional scratch and go with the stiffer wires like Conquest (Asahi Intecc), Hornet (Boston Scientifics), or Gaia (Asahi Intecc) can be used in the difficult cases of subintimal entry. After confirming the Pilot 200 wire, tip was in the extrastent plaque in 2 orthogonal views, we advanced it further with a quick push to form a knuckle and pushed further beyond the zone of underexpansion and stopped a few millimeters before the distal stent edge as shown in Figure 2A, B. The double lumen catheter was removed after trapping both wires and a 3 × 12 mm (Figure 2C) noncompliant balloon was advanced over the safety wire with guideliner support, and the stent started expanding at 14 atmospheres (ATM) which was recalcitrant to 28 ATM before. The balloon was further expanded to the higher pressures after removal of the knuckle wire to avoid entrapment. This step was followed by 3.5-mm NC ballooning and stenting (Figure 2D, E). The RCA was stented with 3.5 × 38 mm and 4 × 28 mm drug-eluting stents followed by IVUS-guided optimization with 3.5 mm and 4 mm NC balloons. Final result with good stent expansion was achieved (Figure 2F). Final minimal stent area of >10 mm2 at the site of previous underexpansion was noticed in IVUS (Figure 2G). 4
(A) Total occlusion of the right coronary artery from within the previous stent, (B) right coronary artery after thrombosuction showing stent under expansion, (C) intravascular lithotripsy, (D) 1.5 mm burr rotablation, and (E) IVUS showing severely under expanded stent with the underlying fibrocalcific plaque.
(A) Knuckling of the Pilot 200 wire in the extrastent plaque, (B) graphical representation of the knuckling. Extrastent plaque entry done proximal to site of underexpansion and within the stent. Knuckle advanced beyond the point of underexpansion and stopped proximal to distal stent edge, (C) postplaque modification, 3 × 12 mm NC balloon expanded without waist, (D) 3.5 × 38 mm stent midstent expansion, (E) 4 × 28 mm stent proximal RCA stent expansion, (F) final angiogram with good stent expansion, (G) final minimal stent area of >10 mm2 at the site of previous underexpansion.
Discussion
Adequate plaque preparation is very important in fibrocalcific lesions before the stent implantation to avoid the underexpansion. Underexpanded stent limits the available interventional options and diminishes the efficacy of them in modifying the extrastent plaque. Extrastent plaque modification with the knuckle wire is one of the therapeutic options if all the other methods like rotablation, OPN NC, and IVL fail. Excimer laser is useful in such scenarios, but its availability is limited to few centers. The extrastent knuckling technique should be done with a safety wire in the distal vessel through the center of the unexpanded stent. Subintimal access can be achieved by scratch and go with a polymer jacketed wire like in this case or by the conventional scratch and go with stiff wire through microcatheter. Knuckle should never be pushed beyond the distal stent edge, preferably ending it immediately distal to the under expanded struts (Figure 2B).
A modified technique done by Michael Megaly et al 5 was published, where they used GAIA next III nonpolymer jacketed tapered stiff wire to gain access to the subintima and then deescalated to a stiffer polymer jacketed mongo wire (Asahi Intec) for knuckling. The polymer jacketed wire acts as a rail over which smaller balloons are advanced into the subintimal space and inflated followed by inflation of the NC balloon in the true lumen and then simultaneous inflation of both the balloons. Final dilatation of stent was done after the subintimal gear removal to avoid entrapment.
The extrastent knuckling technique is not a routine technique that can be used for all the cases of resistant stent underexpansion. Nevertheless, this technique is sure a bailout for the stent underexpansion that did not respond to all available conventional techniques.
This technique should be the last resort as it has the intrinsic risk of coronary perforation and subintimal hematoma compromising the distal true lumen. 6
Conclusions
The extrastent plaque modification with knuckle is a new tool for resistant stent under expansion which should be used by the operators experienced in using the knuckle wire, following all the principles of safe usage (Figure 2B) modification of the extrastent plaque and the methods to do that need further research. 2 This technique should be employed only when other conventional and more safer methods failed to achieve adequate stent expansion.
Footnotes
Acknowledgements
I would like to acknowledge Dr Chandana Poosala from the clinical research department for drafting the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.