
Abstract
Coronary artery disease (CAD) is an important cause of morbidity and mortality worldwide. Perfusion abnormalities precede wall motion abnormalities, ECG changes, and angina in the etiology of CAD. myocardial perfusion imaging (MPI) can detect perfusion alterations due to pathology at sites such as the endothelium, microvasculature, and epicardial coronary arteries. Thus, it measures the universal burden of ischemic heart disease (IHD). Nuclear medicine MPI is an important noninvasive imaging modality to evaluate the perfusion of the myocardium. Positron Emission Tomography (PET) and single-photon emission computed tomography (SPECT) with or without computed tomography (CT) are 2 primary modalities. PET is a highly sensitive modality with an inherent ability to quantify absolute myocardial blood flow (MBF) and variations in MBF due to various stress agents. PET has immense potential to change clinical management, prognosticate, and risk stratify patients presenting with clinical or preclinical CAD. Evidence shows that early PET detection of myocardial perfusion abnormalities, followed by aggressive intervention for cardiovascular risk factors, can reinstate myocardial perfusion. This may reduce morbidity and mortality. We shall be reviewing the clinical impact of PET in CAD and preclinical CAD patients.
Keywords
Abbreviations
CAD: coronary artery disease
CFR: coronary flow reserve
CVD: Cardiovascular disease
IHD: ischemic heart disease
MBF: myocardial blood flow
MFR: myocardial flow reserve
MPI: myocardial perfusion imaging
PET: positron emission tomography
SPECT: single-photon emission computed tomography
TVD: triple vessel disease
Introduction
Cardiovascular disease (CVD) remains the forerunner cause of mortality all over the world. The prevalence is increasing in the Indian population, with increased risk factors for the disease.1,2 It has become the leading cause of death in the Indian population. 3 Detection of the disease at an early stage of pathology is crucial to reduce disease-related morbidity and mortality. It has been seen that anatomical stenosis correlates poorly with the physiological severity of the lesion, and physiological abnormality precedes anatomical disease. Many clinical trials have shown the superiority of timely detecting physiological abnormality over anatomical lesions in guiding individualized therapy. It may improve clinical outcomes in known, suspected, and at-risk patients of coronary artery disease (CAD). CAD imaging has advanced from only demonstrating epicardial vascular abnormalities to identifying lesions in their earliest pathophysiological phases. This has become possible due to recent advancements in research, clinical trials, and instrumentation. Positron Emission Tomography (PET) myocardial perfusion imaging (MPI) enables true in vivo noninvasive absolute quantification of myocardial blood flow (MBF) and myocardial flow reserve (MFR). Hybrid PET/CT is becoming increasingly popular for assessing myocardial perfusion providing excellent diagnostic and prognostic information.
The Diagnostic Criterion of PET MPI: MBF and MFR
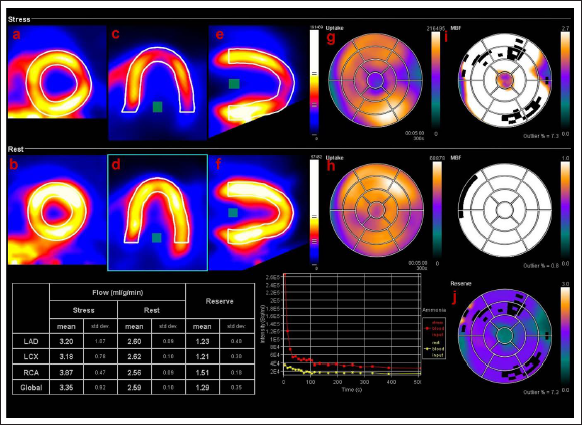
The noninvasive assessment of coronary blood flow, MBF measurement, and its responses to several vasomotor stresses have added enormous knowledge to CAD pathophysiology. 4 Gould et al showed that resting MBF remains unaltered and is proportional to cardiac workload unless epicardial stenosis attains a severity of 90%. This is because of compensatory vasodilation of the coronary microcirculation. 5 However, during hyperemic flow by pharmacologic vasodilation, epicardial lesions with ≥ 50% luminal obstruction decrease hyperemic flow. 6 PET/CT, in concert with kinetic tracer modeling, enables measurement of regional MBF in ml/gram/min. The ratio of MBF at rest and pharmacologically stimulated hyperemic state is known as the MFR. 7 The in vivo and absolute quantification of MBF and MFR provide both diagnostic and prognostic information in the patients (Figure 1). 7
N-Ammonia PET/CT myocardial perfusion imaging of a 62-year-old diabetic male. The upper row (stress images) and lower row (rest images) show blood flow in the short axis (a, b), horizontal long-axis (c, d), and vertical long axis view (e, f). A large area of the mild reversible perfusion defect is noted in the left ventricle’s apex, anterior, and anterolateral walls. The corresponding 17-segment model polar maps suggest the extent of perfusion defects (g, h) and myocardial blood flow (i, j). Coronary flow reserve (CFR) is calculated for each vascular territory (table). It shows normal rest perfusion with reduced CFR (<2). CFR is shown as a polar map (j) that depicts reduced CFR.
13
N-Ammonia PET/CT myocardial perfusion imaging of a 62-year-old diabetic male. The upper row (stress images) and lower row (rest images) show blood flow in the short axis (a, b), horizontal long-axis (c, d), and vertical long axis view (e, f). A large area of the mild reversible perfusion defect is noted in the left ventricle’s apex, anterior, and anterolateral walls. The corresponding 17-segment model polar maps suggest the extent of perfusion defects (g, h) and myocardial blood flow (i, j). Coronary flow reserve (CFR) is calculated for each vascular territory (table). It shows normal rest perfusion with reduced CFR (<2). CFR is shown as a polar map (j) that depicts reduced CFR. 13
PET Myocardial Perfusion Imaging (MPI) for Clinical Management
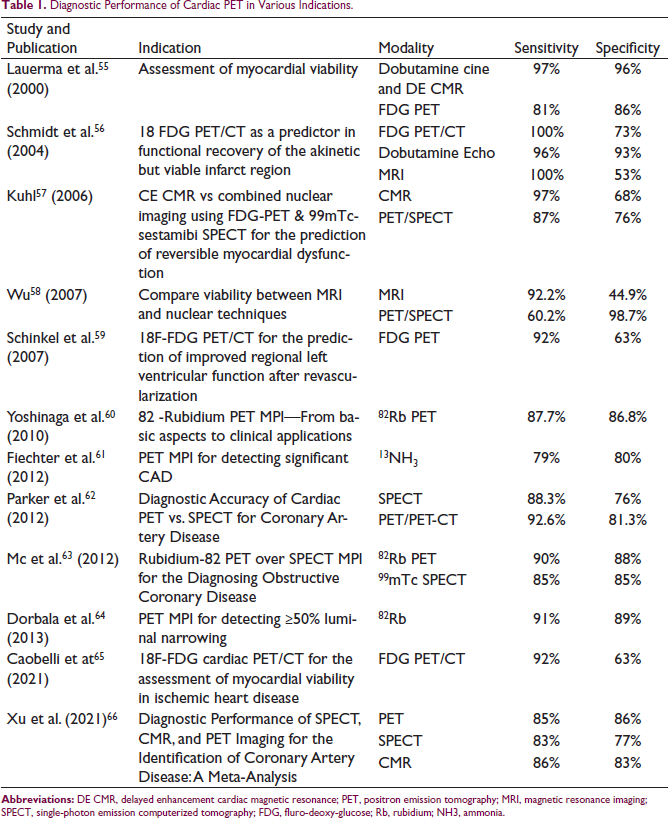
In addition to identifying advanced and flow-limiting epicardial CAD lesions, PET’s ability to noninvasively quantify absolute MBF also allows for the early detection of atherosclerosis, multivessel disease, and microvascular dysfunction. 7 A reduction in radiotracer uptake on standard single-photon emission computed tomography (SPECT) or PET MPI during stress-induced hyperemic flows is related to the flow-limiting effects of CAD. The visual and semiquantitative evaluation of regional radiotracer uptake is in “relative” terms. In patients with multivessel CAD, the assigned normal reference region on uptake images may be, in fact, abnormal as well. However, it is the least hypoperfused myocardial region relative to the remaining vascular territories. 8 In such circumstances, MBF and MFR may unmask the most advanced or “culprit” lesion and the flow-limiting effect of other less severe CAD lesions. 9 In a study by Fiechter et al, the sensitivity and specificity of MPI for detecting significant CAD were 79% and 80%. The positive predictive value (PPV), negative predictive value (NPV), and accuracy were 91%, 59%, and 79%, respectively (Table 1). At a cut-off of <2.0 for MFR, diagnostic performance was improved to 96% (p = .005), 80%, 93%, 89% (p = .005), and 92% (p = .005), respectively. 10
Diagnostic Performance of Cardiac PET in Various Indications.
Diagnostic Performance of Cardiac PET in Various Indications.
Dorbala et al demonstrated that PET MPI had sensitivity and specificity of 91% and 89% for more than 50% luminal narrowing. 11 In epicardial stenosis ≥ 70%, an MFR of <1.7 is related to increases in epicardial resistance. 7 A normal MFR carries a very high NPV (97%) for excluding high-risk CAD. It includes multivessel disease (double and triple vessel disease), proximal LAD, or left main CAD (50% stenosis). Being functional imaging, it does not reliably distinguish between diffuse atherosclerosis, epicardial stenosis from nonobstructive CAD, or microvascular dysfunction. 12 In a meta-analysis (12,000 patients), for detection of >50% epicardial stenosis, PET was found to be more sensitive than SPECT (92.6% vs 88.3%, p = .035) with near-identical specificity. 13
PET has superior diagnostic value and improved risk stratification compared to SPECT due to its ability to assess MBF. 14 Studies have shown that PET-MPI is superior to SPECT in image quality, reliability of interpretation, and diagnostic accuracy. Bateman et al found excellent diagnostic accuracy of PET at stenosis severity of 70% (89% vs 79%, p = .03) and 50% (87% vs 71%, p = .003). 15 A study comparing PET with computed tomography angiography (CTA) has shown a poor PPV of CT angiography to identify functionally significant coronary stenoses as defined by PET. However, CTA is an excellent modality to exclude CAD. However, it has a modest performance in assessing the physiological significance of the degree of luminal narrowing. 16
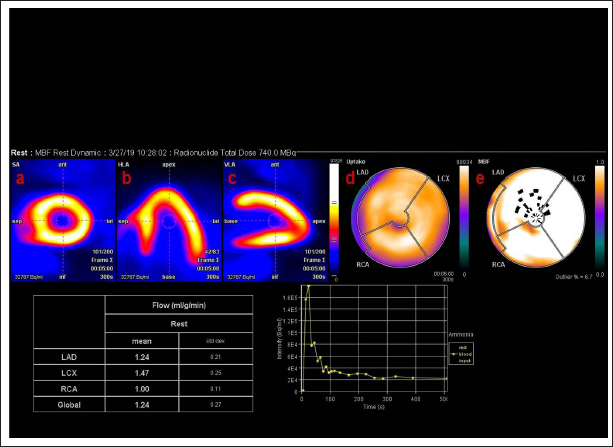
The uniform perfusion deficit in all major vascular territories caused by diffuse myocardial ischemia in significant LMCAD or TVD may lead to false-negative results and go undetected with the routine SPECT MPI. 17 In a study, patients with left main vessel CAD underwent SPECT MPI. Perfusion defects in more than 10% of myocardium were noted in 56% of patients and 59% quantitatively. No perfusion defect (> or = 5% myocardium) was noted in 13% only. 18 Assessing hyperemic MBF and MFR could help prevent a false negative semiquantitative MPI caused by the uniform perfusion deficit in all coronaries. MFR was discovered to be independently predictive of TVD and globally reduced (<2) in 88% of the patients. 8 This incremental value of flow quantification has been supported by another comprehensive study by Naya et al (Figure 2). 12
N-Ammonia PET/CT rest myocardial perfusion imaging of a 71-year-old male. He had severe triple vessel disease with mild left ventricular dysfunction. Myocardial blood flow in the short axis (a), horizontal-long axis (b), and vertical long axis (c) suggest homogenous perfusion in all walls of the left ventricular myocardium. Polar maps (d, f) suggest homogenous uptake and reduced myocardial blood flow pattern in all 3 main coronary arteries.
13
N-Ammonia PET/CT rest myocardial perfusion imaging of a 71-year-old male. He had severe triple vessel disease with mild left ventricular dysfunction. Myocardial blood flow in the short axis (a), horizontal-long axis (b), and vertical long axis (c) suggest homogenous perfusion in all walls of the left ventricular myocardium. Polar maps (d, f) suggest homogenous uptake and reduced myocardial blood flow pattern in all 3 main coronary arteries. 13
Identifying endothelial dysfunction or preclinical CAD in patients with various risk factors for developing CAD could become clinically relevant.19–22 PET MPI is evolving in identifying and monitoring the effects of pharmacologic interventions and lifestyle modification in these patients. In patients with risk factors, coronary dysfunction starts at the endothelium. This leads to impaired endothelium-dependent or flow-mediated coronary vasodilation with preserved smooth muscle cell function. 7 Early coronary artery dysfunction can be detected by assessing MBF and MFR, which provide notable diagnostic and prognostic information.
MBF measurement with the pharmacologically induced hyperemic flow is maintained in asymptomatic insulin-resistant patients with normal stress-rest PET MPI. However, endothelium-related MBF response to cold pressor test (CPT) is impaired. 19 These observations reinforce that the early stages of CAD affect endothelium and could be picked by PET.20,21 Worsening of CPT MBF response is associated with long-term risk for cardiovascular events. 22 As the cardiovascular risk factors and disease progress, oxidative stress burden also increases. This leads to impaired smooth muscle cell vasodilator function in coronary arterioles and arteries. 23
PET MPI to guide decisions for coronary angiography and revascularization
As large prospective clinical trial data on the role of PET MPI in guiding coronary angiography and revascularization are lacking, expert opinion and data from observational studies are used for decision-making. Depending upon the extent and severity of reversible perfusion defects, the MPI results are classified as low risk (defect involving <5% of the myocardium), intermediate risk (5–10% of the myocardium), or high risk (>10% of the myocardium). 24 Invasive coronary angiography is deemed appropriate for patients with high-risk MPI (>10% ischemic myocardium). Other high-risk markers include transient ischemic dilatation of the left ventricle, significant stress-induced left ventricular dysfunction, discordant and ongoing symptoms, or significant ECG changes during stress. However, it is not considered appropriate in patients with low-risk PET findings (<5% ischemic myocardium). 24
Monitoring therapy and reductions in cardiovascular risk
Measurements of MBF may be used to monitor the effects of pharmacologic interventions or lifestyle modification in patients with and without manifested CAD. 7 PET flow studies have verified improved endothelial dysfunction in patients with various cardiovascular risks through regular exercise, preventive medical care, cholesterol-lowering, and antidiabetic medications.25–28
CAD patients were randomly assigned to receive aggressive risk factor adjustment (low-fat vegetarian diet, exercise, and stress management) or standard medical therapy (primarily anti-anginal medications) by Gould et al. After 5 years, the severity and size of the stress-induced PET perfusion defects improved in the experimental patients and worsened in the control group. In contrast, changes in quantitative coronary angiography were much less apparent. 29 PET MPI has also been used to assess the effectiveness of various medical therapies in cardiovascular disease. In diabetic patients, the effect of antidiabetic medications (glyburide and/or metformin) on coronary circulatory function and coronary artery calcifications (CAC) has been studied. There was a lower progression of CAC and increases in endothelium-related MBF responses to CPT with treatment. 30 Hormone replacement therapy using estrogen and/or progesterone has been shown to preserve the CPT MBF response and its standard preventive effect on traditional cardiovascular risk factors. 31
Prognostic Implications
Coronary artery disease
Prognostic data on the clinical utility of SPECT is robust in comparison to PET MPI. Absolute quantification of coronary blood flow using PET MPI allows for accurate prognostication in CAD. PET holistically measures ischemic heart disease (IHD) burden from significant CAD, nonobstructive CAD, diffuse atherosclerosis, and microvascular disease. This allows PET to prognosticate over and above SPECT MPI. In a study including 1432 subjects, Rb-82 PET-CT scan showed a low annualized event rate of 0.7% in patients without ischemia. Patients with a large area (>20% of the myocardium) of ischemia had a high event rate of 11%. 32
Ziadi et al. evaluated the MFR as a prognostic marker for ischemia. Based on summed stress scores (SSS) and MFR, patients were divided into 4 groups. Group I included patients with normal SSS (<4) and MFR (>2), whereas group II-IV had normal SSS with MFR <2, abnormal SSS ≥4 with normal MFR ≥2, and abnormal SSS ≥4 with reduced MFR <2, respectively. Patients with decreased MFR (<2) had higher cardiac death and myocardial infarction rates than those with MFR ≥2 (I: 1.3% vs II: 2% [p = .029]; III: 1.1% vs IV: 11.4% [p = .05]). Thus MFR was an independent predictor of cardiac events irrespective of the SSS and other clinical parameters. 33 Murthy et al reported comparable observations in a large cohort (2783 patients). In comparison to the normal MFR (>2), low MFR (< 1.5) was associated with a 16-fold increased risk of CD. At the same time, the intermediate MFR group (1.5-2.0) had a 5.7-fold increased risk for CD. MFR reclassified 35 % of the intermediate-risk patients (CD: 1%-3% per year) into either low or high risk. 34
In a normal MPI result, a preserved coronary flow reserve (CFR) > 2.0 strongly predicts event-free survival over 3 years, and an adverse prognosis is seen with reduced CFR. 32 Novel parameters such as net reclassification improvement (NRI) and integrated discrimination improvement have better prognostic values than conventional metrics. 35 NRI with PET MPI has been demonstrated in a study by Dorbala et al. The author studied PET MPI in patients with risk factors such as age, female sex, body mass index, hypertension, diabetes, dyslipidemia, smoking, angina, beta-blocker use, prior revascularization, and resting heart rate. Even after accounting for risk factors, patients with a grossly abnormal stress PET MPI had a 5-fold higher CD hazard than patients with a normal MPI. This consolidates that PET MPI provided incremental CD risk compared to traditional coronary risk factors. 36 It is imperative to emphasize that the incremental clinical value of PET MPI is attained at a lower estimated effective radiation dose in comparison to Technetium-99m MPI. 37
PET MPI to predict recovery of function after revascularization
Myocardial viability assessment helps to identify patients who may benefit from coronary revascularization. Percent peak perfusion by N-13 Ammonia (> 50%) is considered a viable myocardium and has a high NPV (>86%) to predict improvement in regional wall motion after revascularization. 38 An earlier study demonstrated a relationship between cell membrane integrity (by Rb-82 PET) and myocardial glucose utilization as a viability marker. Hypoperfused regions show different Rb-82 kinetics in compromised but metabolically active and irreversibly injured myocardium. 39 PET MPI provides incremental prognostic value to clinical variables predicting all-cause mortality and CD in Coronary artery bypass grafting patients. 40
Heart failure (HF)
Approximately two-thirds of HF cases are ischemic, and the rest are nonischemic. However, there is an overlap between these 2. Radionuclide Imaging can differentiate them. 41 Ischemic HF is suggested by a history of MI, revascularization, significant left-main CAD (>75% stenosis), or multiple vessel disease. 42
PET helps to detect multivessel CAD.8,43 It identifies high-risk patients with normal perfusion images.33,34 Abnormal CFR identifies patients at risk of developing HF. 44 Many nonischemic HF or cardiomyopathy patients have CFR abnormalities due to microvasculature involvement. 45 Neglia et al have demonstrated that patients with nonischemic dilated cardiomyopathy and a low MBF (≤ 1.36 mL/min/g is) had an increased risk of CD and 3.5 times progression of HF over other standard clinical and functional variables. 46
Role of PET MPI in special population
Risk factors such as smoking, hypertension, diabetes, hypercholesterolemia, obesity, menopause, or family history, have been associated with attenuated endothelium-dependent vasodilation. 4 The incremental predictive value of MFR for predicting cardiac death has been reported in patients with diabetes mellitus, chronic kidney disease, and ischemic or idiopathic cardiomyopathy.46–48
A recent study evaluated the change in MBF in morbidly obese individuals (BMI ≥ 40 kg/m2) after surgical bypass-induced weight loss. The patients did not have other traditional cardiovascular risk. After a median follow-up of 22 months, BMI decreased from a median of 44.8 to 30.8 kg/m2. There were changes in lipid profile, reduced plasma markers of the insulin resistance syndrome, chronic inflammatory markers, hyperemic flow reserve, and endothelium-related MBF responses to CPT. 49 The diagnostic evaluation of women presenting with suspected cardiac symptoms is challenging, with reported lower accuracy, attenuation artifact, and concerns regarding radiation safety. Stress Rb-82 PET provides clinically significant risk stratification in both women and men. It is beneficial in identifying high risk older women. 50
Risk Stratification—PET MPI Imaging Risk Factors
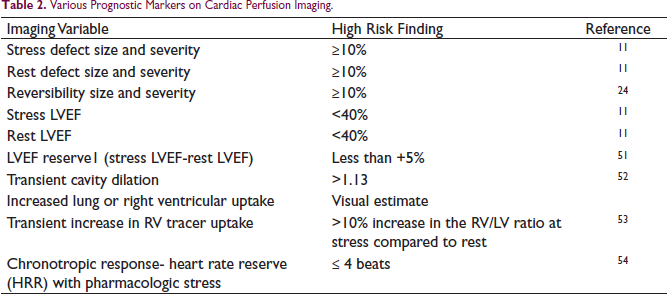
Imaging and clinical findings on PET MPI stratify patients into low and high risk groups. A few of them are summarized in Table 2.
Various Prognostic Markers on Cardiac Perfusion Imaging.
Limitation
In comparison to SPECT, PET perfusion has a few limitations. The main shortcomings of PET are the availability of PET CT scanners, cost, and the need for an on-site cyclotron or generator system. Prognostic data on the clinical utility of SPECT is robust and extensively investigated. Evidence supporting the clinical utility of PET MPI is still limited but rapidly evolving.
Conclusion
PET MPI enables the noninvasive assessment of myocardial perfusion by measuring functional parameters like regional MBF and MFR. The sensitivity of PET is more than SPECT for the identification of CAD, and a normal PET scan effectively rules out CAD with excellent NPV. Understanding MBF and its response to various vasomotor stress has significantly advanced our understanding of CAD pathogenesis. It may detect endothelial dysfunction or preclinical CAD in patients with various CAD risk factors and helps to monitor the effects of lifestyle modification and/or pharmacologic interventions. In short, PET has an “in vivo” holistic capability to image and quantify IHD rather than CAD alone. This capability of PET MPI imaging, if combined with diagnostic CT, may lead to identifying both functional and structural abnormalities in coronary arteries before progression to clinically manifest CAD. Overall cardiac PET/CT may be the next step in the “precision medicine” era.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.