
Abstract
Some individuals develop a rare form of coronary heart disease called coronary artery ectasia (CAE). It is characterized by a dilation of more than one-third of the length of a coronary artery and a diameter that is 1.5 times that of the adjacent normal coronary artery. In the absence of significant coronary constriction, angina pectoris, positive stress tests, and acute coronary syndromes may all be indications of CAE. A distal embolization, vasospasm, or vascular rupture may cause thrombus formation in an ectatic artery. Antiplatelets, such as aspirin, are the cornerstone of treatment for people with CAE. Anticoagulants are used to prevent thrombus formation based on the presence of concurrent obstructive coronary artery disease and the patient’s risk of bleeding. As atherosclerosis is the most common cause of CAE, all patients are advised to take statins for primary prevention. Due to their anti-inflammatory properties, angiotensin-converting enzyme inhibitors may be prescribed to individuals with hypertension. If hypertension and coronary vasospasm occur simultaneously, beta-blockers and calcium channel blockers may be beneficial. Because they may aggravate symptoms, nitrates are normally not suggested. Other CAE treatment methods include the prevention of thromboembolic complications and percutaneous or surgical revascularization. CAE prognosis is determined on the severity of the associated coronary artery.
Introduction
Coronary artery ectasia (CAE) was originally described in 1761 by Morgagni. CAE is an extremely rare coronary angiographic finding, with a frequency ranging from 1.5% to 5% and varied by region.1-3
Ectasia describes widespread dilatation of a coronary artery, whereas aneurysm describes a more focal dilatation. When the diameter of a coronary artery is more than 1.5 times that of the largest diameter of a neighboring normal artery, this condition is known as coronary ectasia.3, 4
Despite the fact that various causes have been proposed, the pathophysiology of CAE is still poorly understood. Similarly, due to a lack of evidence, there is no agreement on the natural history and management of this syndrome. CAE is not only an anatomical variety of coronary artery disease (CAD) but also a clinical constellation of CAD, including myocardial ischemia and acute coronary syndromes.5, 6
The purpose of this review is to provide an overview and status report on CAE and its management.
Classification of Coronary Ectasia
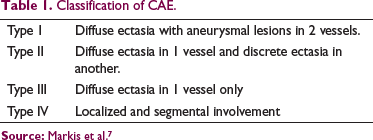
Markis et al 7 has classified CAE into 4 types which is based on the extent of involvement (Table 1).
Classification of CAE.
Epidemiology
Globally, the incidence of CAE has been the subject of substantial investigation. CAE has been detected in 3% to 8% of angiographic and 0.22% to 1.4% of autopsy datasets, respectively. It may be diffuse or localized and can affect the full length of a coronary artery.8, 9 According to the studies from South India, the incidence of angiographic CAE is roughly 4.5%, 10 while the frequency of pure CAE without CAD is 1.9%. 11 In a post hoc examination of a small sample from North India, the incidence of CAE in patients with ischemic heart disease was shown to be about 10%. An angiographic prevalence of CAE was determined to be around 5.45% in recent Northeast Indian research, while isolated coronary ectasia was found to be 1.05%. 12 In a prospective research from North India, 4.1% of 3,014 consecutive coronary angiographies revealed the presence of CAE in angiography. 2
Etiology
CAE's etiology is a little hazy. Atherosclerosis is the most prominent etiologic cause in adults, accounting for more than half of all cases, while Kawasaki disease is the most prevalent etiologic cause in children and adolescents.13-15 Males are more likely to get CAE. 16 Genetic factors have also been connected to the development of CAE. The DD genotype variation of angiotensin converting enzyme seems to be a significant risk factor for the development of CAE.17, 18 By activating matrix metalloproteinase (MMP) 2 and boosting serine proteinase activity in arterial smooth muscle cells, homocysteine levels may contribute to the disintegration of the medial arterial layer.19, 20 CAE is linked to high blood pressure. 21 According to a meta-analysis, people with DM had a low risk of CAE. This might be related to MMP downregulation and negative remodeling as a result of atherosclerosis. 22 Patients with CAE appear to smoke more frequently than individuals with CAD. 23
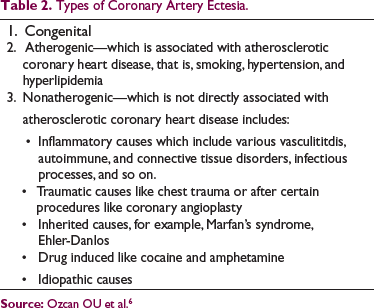
Cocaine use was also identified as an independent predictor of CAE, regardless of whether the individual smoked or not. 24 Particularly, low endothelial shear stress (ESS) predisposes coronary arteries to atherosclerosis, vulnerable plaque growth, and aneurysm formation. 25 Table 2 shows various reasons related with coronary ectasia.
Types of Coronary Artery Ectesia.
Pathogenesis
Following theories were proposed to explain the pathogenesis of ectasia.
Hemodynamic theory: Focal ectasia is caused by the conversion of kinetic energy to potential energy, as well as pressure irregularities above the stenosis threshold. It has also been proposed that high blood flow velocity causes endothelial damage and poststenotic vasodilation because of higher shear stress at the stenosis level. Low ESS has also been shown to have an important effect as a trigger for the transformation of early atherosclerotic plaque to expansive remodeling (positive remodeling ectasia), this has been confirmed in a in vivo study.8, 26, 27 Vascular remodeling theory: Coronary ectasia is a kind of excessive positive remodeling (expansive remodeling) of the artery wall that occurs during the early stages of plaque formation and after a plaque rupture event. This expansion may cause low shear stress which perpetuates the vicious cycle.26, 27 Inflammatory hypothesis: Atherosclerosis is an inflammatory condition which affects the arteries. Ectasia is caused by inflammatory cells from the intima spilling over into the tunica media layer and being destroyed. Inflammation is thought to be the primary pathogenic connection between atherosclerosis and CAE, with hemodynamic variables. The underlying cause for CAE is cytokine-induced widespread inflammation encompassing all the 3 layers of the artery wall. Inflammatory indicators such as plasma interleukin-6 and C-reactive protein (CRP) are higher in CAE patients than in individuals with normal coronaries.
24
Furthermore, cell adhesion molecules (vascular cell adhesion molecule, intercellular adhesion molecules) that aid in the transmigration of inflammatory cells increased in the sera of ectasia patients. To back up the inflammatory theory, the neutrophil-to-lymphocyte ratio, a marker of inflammation, is considerably greater in patients with isolated ectasia than in persons with normal coronaries, suggesting that neutrophils play a role.26, 28, 29 Excessive vasodilator mechanism (nitric oxide [NO] mediated): Excessive vasodilation mediated by NO is the most prevalent mechanism in patients with nonatherosclerotic CAE. NO levels and other toxins alter the extracellular matrix, causing artery wall weakening and ectasia. Ectasia has been shown to be more common in those who have been exposed to a herbicide spray that includes an acetylcholine esterase inhibitor. This substance boosts NO generation mediated by acetyl choline.26, 30 Genetic theory: The disruption of the MMP-3 gene (MMP-3 5A allele),
33
a polymorphism of the angiotensin-converting enzyme (ACE), has been linked to ectasia. The HLA-DR B1 13, DR16, DQ2, and DQ5 genes were used to establish HLA linkage.26, 31 Generalized vascular disorder: CAE may be part of a broader arterial wall problem (deficiency), as indicated by its links to aneurysms of the ascending aorta and abdominal aorta. CAE has also been linked to venous illnesses such as coronary vein varicosities, leg vein varicosities, and pampiniform plexus.26, 32
Clinical Features
Conventional coronary risk factors like obesity, hypertension, smoking, and stress are accompanied with CAE. CAE is often discovered incidentally during an angiography for another heart issue. The clinical characteristics of CAE remain unknown. In individuals with CAE and coronary narrowing, stable angina is the most prevalent symptom. Acute coronary syndrome and positive treadmill exercise tests are possible diagnoses. Atherogenic causes are more frequently associated with the CAE.33, 34
Angiographically, the most important predictors of ischemia during exercise testing in those with isolated CAE were the extent of the ectasia and the backflow phenomenon in an ectatic left anterior descending artery. 12 ST-elevation myocardial infarction (MI) 34 and non-ST elevation MI 35 may both result from altered blood flow due to distal embolization or thrombus occlusion of the ectatic segment. Thrombus development, distal embolization, shunt formation, and rupture are all possible complications, but the exact risk is unknown. CAE can also cause left-to-right shunts by breaking through into the right atrium, right ventricle, or coronary sinus.8, 36
Diagnosis
Coronary Artery Angiography
It is the gold standard for identifying CAE. By measuring the degree of ectasia, angiography identifies issues with blood flow filling and washout. Delay in antegrade dye filling, segmental reverse flow, and local dye deposition in the dilated coronary segment are all angiographic indicators of turbulent and stagnant flow, respectively.9, 37
Coronary Magnetic Resonance Angiography (MRA)
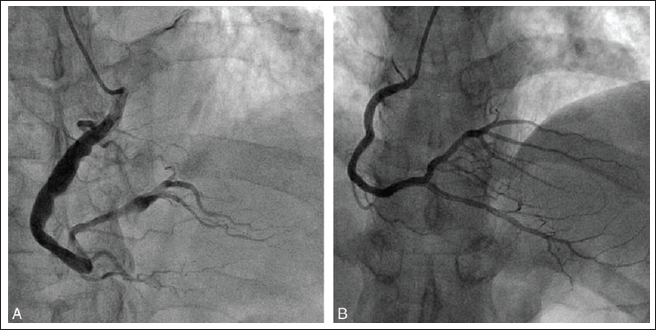
In addition to being noninvasive, MRA has been shown to be as effective as quantitative coronary angiography. When paired with coronary flow data, coronary MRA may give further insight into the danger of thrombotic obstruction of aneurysmal arteries. In addition, since MRA is a noninvasive, radiation-free technique, it may be used successfully for patient follow-up (Figure 1).9, 39
Coronary Artery Computed Tomography (CACT)
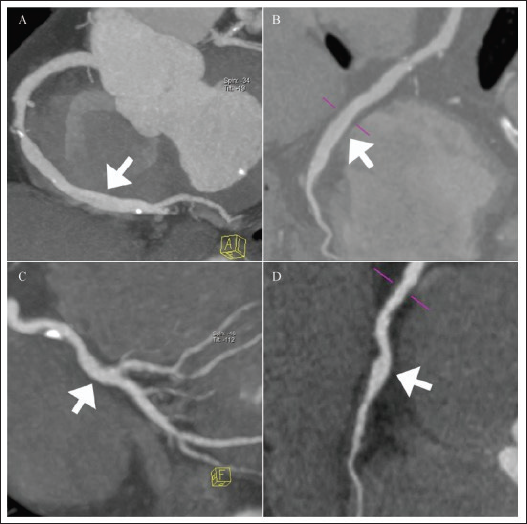
It's a noninvasive method of diagnosing CAE. CTCA measures of contrast attenuation correspond well with flow changes determined with traditional X-ray coronary angiography. However, due to radiation exposure, the function of CACT in patient follow-up is limited (Figure 2).9, 13
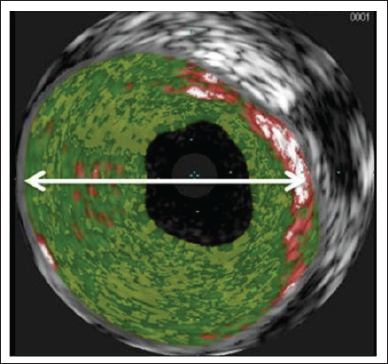
Intravascular Ultra Sound (IVUS)
It is an excellent instrument for evaluating luminal size and recognizing arterial wall changes. IVUS distinguishes true aneurysms caused by plaque rupture from fake aneurysms. Empty plaque cavities may appear as CAE on angiography, and the distinction is crucial in clinical practice since false aneurysms may induce acute coronary syndromes (Figure 3).8, 41
Inflammatory Markers
Cytokines (TNF-alpha, IL-6), proteolytic substances (cathepsin L, Cathepsin C, Matrix metalloprotein-3), cell adhesion molecules (E-selectin, P-selectin), and systemic inflammatory markers (CRP, homocysteine, neoprotein) are certain inflammatory markers which are elevated in the CAE and its association also depends on morphology of CAE.43, 44
Management
Despite the fact that the disease has been known for more than 50 years, there are no clear management guidelines due to its rarity. General measures, pharmaceutical treatment, percutaneous intervention, and surgery are currently viable care options. The treatment is determined by the cause and any potential or obvious consequences.
General Measures
Lifestyle modifications like balanced diet, cessation of smoking and tobacco, regular physical activity, stress management, and so on. Control of other cardiovascular morbidities like prevention and treatment of obesity, hypertension, diabetes mellitus, dyslipidemia, and so on.
Pharmacological Management
Antiplatelets
A comprehensive review and meta-analysis by Moghadam et al 45 revealed that patients with CAE had a significantly higher mean platelet volume than healthy individuals, indicating that platelet thrombotic effects may play a role in the genesis of CAE. As a result, antiplatelet drugs like aspirin may be useful in the treatment of this condition. Platelet inhibitors are utilized to prevent ischemia syndromes caused by fibrin thrombus development, and micro emboli washing is important in all types of CAE. When compared to a reference group with normal coronary arteries, individuals with isolated CAE without accompanying coronary artery stenosis showed substantially greater levels of betathromboglobulin, P-selectin, and platelet factor 4, suggesting enhanced platelet activation. 46 CAE is linked to inflammation and platelet activation, according to a study conducted by Wei et al. 47 Antiplatelet treatment, such as aspirin, appears to be beneficial to the patients. 47 The combining role of antiplatelet and adenosine diphosphate receptor inhibitors has yet to be determined. However, Pranata et al 48 found that dual antiplatelet medication is less beneficial than anticoagulants in avoiding ACS recurrence in the context of CAE in a comprehensive analysis of case reports. In individuals with Kawasaki illness, aspirin and intravenous gamma globulin treatment minimizes the development of coronary ectasias. 49
Anticoagulants
Due to the susceptibility of ectatic coronary arteries to thrombosis, dissection, and spasm, anticoagulants such as Warfarin have been recommended as a treatment. If there are no contraindications, individuals with atherosclerotic CAD who have had MI with thrombosis should be evaluated for lifelong systemic anticoagulation medication for secondary prevention. The risk of bleeding must be carefully evaluated in individuals over the age of 65 and in those who are currently using single or dual antiplatelet therapy.50, 51 CAE-related infarct is frequently accompanied with high-burden thrombus development, according to a case study by Li et al. 52 Long-term warfarin combined with antiplatelet treatment may be a viable option for reducing thrombus load and improving blood flow. Patients with CAE who used anticoagulants had a decreased risk of ACS recurrence (P = .035), according to Pranata et al. 48 Treatment with anticoagulants in patients with isolated CAE is still up for discussion. Willner et al 53 tracked 161 individuals with CAE for 10 years and found that the risk of unfavorable clinical outcomes was decreased in patients with isolated CAE compared to those with CAE and associated atherosclerotic coronary heart disease (P = .05). As a result, they advised avoiding anticoagulant treatment in individuals with isolated CAE. Grigoro 54 performed an observational study in which 75% of 20 patients with CAE types I, II, and III were treated with warfarin plus aspirin 160 mg per day. After 4.2 years of observation, there was neither mortality nor side-effects.
Novel anticoagulants has been also tried for the management of CAE. Case reports for the efficacy of novel anticoagulants like rivaroxaban, dabigatran, and apixaban are also published which shows efficacy of novel oral anticoagulants (NOAC) in the treatment of the thrombosed ectatic coronary arteries.55-57
ACE Inhibitors
Because of their antihypertensive properties, ACE inhibitors have been considered for the treatment of CAE. By lowering intramural pressure, systemic hypertension can assist and halt the process of coronary dilatation. ACE medications reduce systemic blood pressure by blocking the vasoconstrictive effects of angiotensin in the renin-angiotensin-aldosterone pathway. The ACE DD genotype polymorphism is linked to IICAE. MMP and hs-CRP levels were observed to be high in CAE patients. ACE inhibitors and angiotensin receptor blockers are efficient at counteracting this impact, as well as lowering systemic hypertension.51, 58 Ranin-angiotensin system blocker (RASB) treatment is related with a decrease in all-cause mortality and nonfatal infarction, according to Wang et al’s 59 retrospective investigation of 595 CAE patients.
Statins
Because MMP-3 levels are thought to have a role in the formation of coronary aneurysms, this matrix-degrading enzyme might be a promising therapeutic target. Statins may help by reducing MMP-3 activity, corticosteroids, and IL-4 production, as well as lowering MMP expression. 51 Fan et al 60 treated 217 individuals with CAE with oral rosuvastatin in a prospective trial. After 6 months of rosuvastatin medication, hs-CRP and IL-6 levels were found to be considerably lower. They came to the conclusion that rosuvastatin-based anti-inflammatory medication was more beneficial in younger CAE patients.
Antianginal Drugs
Trimetazidine increases intracellular adenosine triphosphate and adenosine, prevents oxygen-free radical-induced ischemia damage, and changes cardiac energy generation from fatty acid oxidation to glucose consumption. Adenosine increases myocardial preconditioning and ischemia tolerance. Trimetazidine has anti-ischemic actions without changing heart rate, blood pressure. It doesn't change coronary blood flow or oxygen consumption. 58
Dogan et al 61 evaluated the effects of trimetazidine on exercise performance in CAE patients. In individuals with a positive exercise stress test, trimetazidine dramatically reduced ST-segment depressions. It increased cardiac workload and exercise duration.
Ranolazine, a new antianginal drug, reduces myocardial sodium and calcium (Ca) overload by inhibiting the late sodium current (I(Na)) of the ventricular action potential. Phase-III studies in individuals with chronic angina show that ranolazine improves exercise tolerance and lowers ischemia symptoms. Therefore, these drugs might be used to boost exercise tolerance in CAE patients. 62
Other Medications
Nitrates, which induce the steal syndrome and worsen anginal symptoms via dilation of epicardial coronary arteries, are not indicated in CAE. 63 Because of their antihypertensive and anti-ischemic properties, beta-blockers may be prescribed.58, 64 Ca channel blockers, which have an antihypertensive effect, can be used to avoid coronary vasospasm.64, 65
Colchicine also showed promising results in the treatment of acute coronary syndrome with normal coronary arteries, however trials needed to explore its use in CAE and aneurysms.
Novel biomarker targeted therapies-molecules targeting damage associated molecular pattern/micro RNAs may be the future for the treatment of CAE but the trials are yet to confirm.
Interventional Management
Patients with CAE who have concomitant obstructive lesions or who have symptoms or indications of myocardial ischemia despite adequate pharmacologic treatment often need invasive options. Two options are percutaneous coronary intervention (PCI) and coronary artery bypass graft.8, 58 Individuals who have concurrent obstructive lesions and symptoms or indications of significant ischemia despite medical therapy are candidates for percutaneous transluminal coronary angioplasty. It has been determined that a polytetrafluoroethylene-coated, balloon-expandable stent is an effective device for the percutaneous treatment and exclusion of coronary aneurysms. 67 Surgery is seldom performed, but in individuals with recurrent issues it may be necessary. The ectatic vessel’s proximal and distal segments are ligated and replaced with a bypass graft during surgery. Coronary artery bypass grafting is an effective therapy for obstructive CAE.8, 68 PCI has some complications like injury to coronary arteries, bleeding, infection, allergic reaction to dye or contrast used, and so on. Ectatic vessels are also more prone to rupture and coronary artery perforation is a rare and serious complication of PCI so this fat should be kept in mind. 69
Prognosis
The prognosis of CAE is directly related to the degree of the accompanying CAD. For individuals with obstructive CAD, CAE is a serious problem since it increases the risk of a wide variety of adverse cardiac events. Isolated ectasia still presents a risk of myocardial ischemia and infarction, even though there was no difference in mortality between those with and without CAE. 70 According to Markis’ categorization, type I and II coronary ectasias have a worse prognosis than type III and IV. The death rate at 2 years is claimed to be 15%. There is no relationship between the width of ectasia and survival. 71 CAE that is isolated has a better prognosis, and antiplatelet medications are used to treat it.70, 71
Conclusion
CAE is a kind of atherosclerosis that occurs in 3% to 8% of coronary angiography operations for diagnostic purposes. When it comes to CAE, there is currently no agreed-upon treatment plan. All of the existing research has flaws, including a lack of randomization, no control group, and a small sample size. Large randomized clinical trials are challenging to do because of the rarity of this illness. Treatment options include anti-ischemic drugs, antithrombotic management, and percutaneous or surgical revascularization. Additional testing is needed to determine the best approach to CAE management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.