
Abstract
Objective
To conduct risk assessment and assess the choice of statins with regard to cardiovascular diseases (CVDs).
Methodology
This is a cross-sectional observation study conducted on 500 patients visiting a teaching hospital. Medical records were used to obtain patient characteristics and type, dose, and regimen of prescribed statin. Prescribed statin dose was evaluated using standard prescribing guidelines by American College of Cardiology/American Heart Association.
Result
Out of the 500 patients studied, 70% (350) of patients were prescribed statin therapy for a CVD and 30% had at least 1 CVD risk factor. Proportion of males was higher. Mean age of patients with statin therapy for coexisting CVD was 61.16 ± 12.87. Among those with at least 1 cardiovascular risk factor but without CVD, 66% had risk score more than 7.5 out of 10 suggestive of high risk for CVDs within 10 years. Atorvastatin and rosuvastatin were the preferred choice of statin therapy, with higher preference for atorvastatin. Dosing criteria were well-met for secondary prevention; whereas, underdosing was prevalent among users of fixed-dose combinations and among patients prescribed a statin for primary prevention of CVDs.
Conclusion
Lack of use of risk scores may lead to underdosing and underutilization of statins.
Introduction
The rising burden of cardiovascular diseases (CVDs) and projected mortality of about 4 million people by 2030 have posed a big public health threat.1, 2 The Framingham Heart Study has demonstrated a direct relationship between the serum cholesterol levels and CVD such as coronary heart disease (CHD) and stroke.3, 4 As per an estimate by the Public Health Foundation of India in 2011, there were 30 million patients with CHD in India. 5 According to a 2014 study by the Indian Council of Medical Research, more than three-quarters (79%) of the general population exhibited abnormalities in at least 1 of the lipid parameters, with no difference between urban and rural areas. 6 Given the burden of CVD and lipid-lowering benefits of statins, their use is high. A statin utilization study published by Choudhry et al analyzed prescription data in India, during the period 2006 to 2009 and found that 8,000 per 1,00,000 patients with CHD were receiving statins. 7
Results of a survey including 358 physicians in India suggest that rosuvastatin is the most preferred statin for primary prevention (50.6%) and secondary prevention (49.4%) followed by atorvastatin. 8 The findings are controversial to those of another survey including 404 physicians where atorvastatin was the preferred choice for primary (72.9%) and secondary prevention (78.3%) followed by rosuvastatin. 9 However, less is known about the granularities in utilization trends such as dosing, the rationale of dosing, and patient characteristics. This study aims to address these gaps in the existing literature. Along with assessing the utilization pattern, we have further attempted to evaluate the rationale of dosing by referring to the standard dosing guidelines for statins by the American Heart Association/American College of Cardiology (AHA/ACC). 10
Methodology
This was a cross-sectional observational study conducted using medical records in Bharati Hospital and Research Center at Pune, for 2 years. The study was approved by the Institutional Ethics Board of Bharati Hospital and Research Center, Pune. Patient consent was obtained prior to data collection and confidentiality of patient information is maintained. The study population comprised of individuals ≥21 years with one or more CVD risk factors (hypertension, diabetes, dyslipidemia, and smoking) and/or a comorbid cardiovascular condition. The “American Heart Association/American College of Cardiology’s (AHA/ACC) updated guidelines on cholesterol management, 2018” were used as the standard of care for evaluating the rationale of statin use. 9 The study evaluated patient characteristics, utilization of statins by indication (primary vs secondary prevention, disease type), product type, and dosage form (unit-dose or fixed-dose combinations). Patient demographics, diagnoses, clinical findings, laboratory values, prescribed statin, its dose, and regimen were collected using in-hospital medical records. As per ACC/AHA recommendation, every patient in the study was assessed for 10-year cardiovascular risk using a risk score calculated by “Pooled Cohort Equations.” Individuals were stratified by their risk scores as ≥7.5% (high-risk individuals), 5% to 7.5% (moderate-risk individuals), and <5% (low-risk individuals).
Statistical Analysis
Nonprobabilistic convenience sampling was used for identifying the study participants. The study population was analyzed by type of prevention indicated for statin use, that is, primary prevention and secondary prevention. Primary prevention comprised of all those who were eligible for statin use for prevention of first CVD event, while secondary prevention comprised of all those who were eligible for statin use for a coexisting CVD comorbidity prior to entering the study. Descriptive statistics are reported as mean and standard deviation. Chi-square test and student-tests were applied to identify statistically significant differences, using 0.05 as a level of significance. MedCalC (version 12.7.0.0) software was used for statistical analysis.
Results
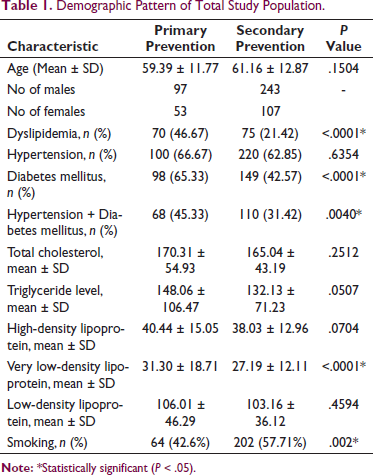
This study population consisted of 500 patients, of which 150 were statin eligible for primary prevention and 350 were statin eligible for secondary prevention. The proportion of males in the total study population (n = 500) was higher (68%), 70% of patients had a prior history of CVD. Hypertension and diabetes mellitus were the leading CVD risk factors observed in the study population. Table 1 provides an overview of the demographics and risk factors observed in the study population. Among those who were eligible for statin use for primary prevention (n = 150), 66% were at a high risk of acquiring CVD in 10 years.
Demographic Pattern of Total Study Population.
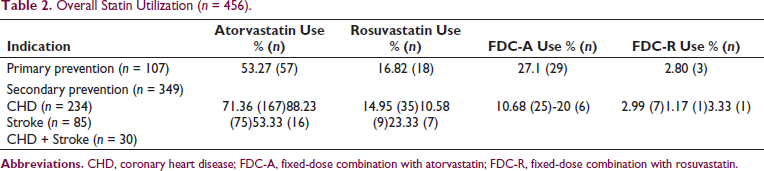
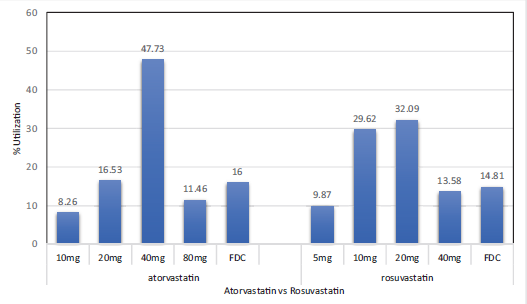
Statin use was observed for atorvastatin and rosuvastatin products either as single-dose formulations or fixed-dose formulations. Atorvastatin use was higher as compared to rosuvastatin (Table 2). Use of atorvastatin 40 mg and rosuvastatin 20 mg was found to be the highest (Figure 1). Use of low-intensity (10 mg) and moderate-intensity (20 mg) atorvastatin as single-dose therapy and the fixed-dose combination was significantly higher among primary prevention patients, whereas the use of high-intensity atorvastatin was significantly higher in secondary prevention patients (Table 3).
Overall Statin Utilization (n = 456).
Dose Utilization of Atorvastatin vs Rosuvastatin in Primary and Secondary Prevention Patients.
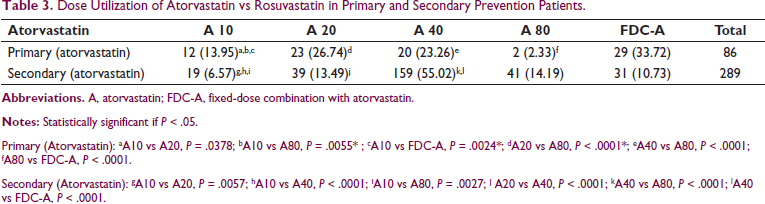
Primary (Atorvastatin): aA10 vs A20, P = .0378; bA10 vs A80, P = .0055* ; cA10 vs FDC-A, P = .0024*; dA20 vs A80, P < .0001*; eA40 vs A80, P < .0001; fA80 vs FDC-A, P < .0001.
Secondary (Atorvastatin): gA10 vs A20, P = .0057; hA10 vs A40, P < .0001; iA10 vs A80, P = .0027; j A20 vs A40, P < .0001; kA40 vs A80, P < .0001; lA40 vs FDC-A, P < .0001.
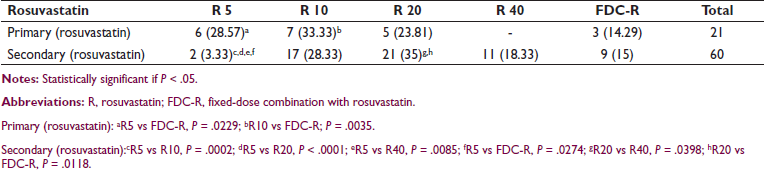
Primary (rosuvastatin): aR5 vs FDC-R, P = .0229; bR10 vs FDC-R; P = .0035.
Secondary (rosuvastatin):cR5 vs R10, P = .0002; dR5 vs R20, P < .0001; eR5 vs R40, P = .0085; fR5 vs FDC-R, P = .0274; gR20 vs R40, P = .0398; hR20 vs FDC-R, P = .0118.
Overall Dose Utilization of Statins.
Similar utilization pattern was observed for rosuvastatin, with significantly higher use observed for low-dose rosuvastatin among primary prevention patients and high dose for secondary prevention patients. The use of fixed-dose combination products was higher for atorvastatin products as compared to rosuvastatin products (Table 3).
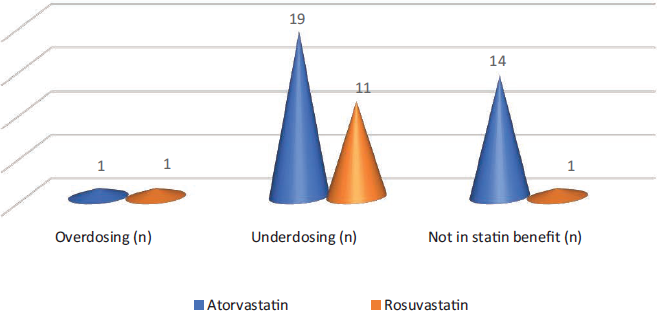
The prescribed dose of statin was assessed for dosing rationale using the prescribing guidelines by AHA/ACC. The findings suggest underdosing was predominant among statin-eligible users for primary prevention (Figure 2).
Deviation of Statin Use From ACC/AHA Recommendations in Primary Prevention Patients.
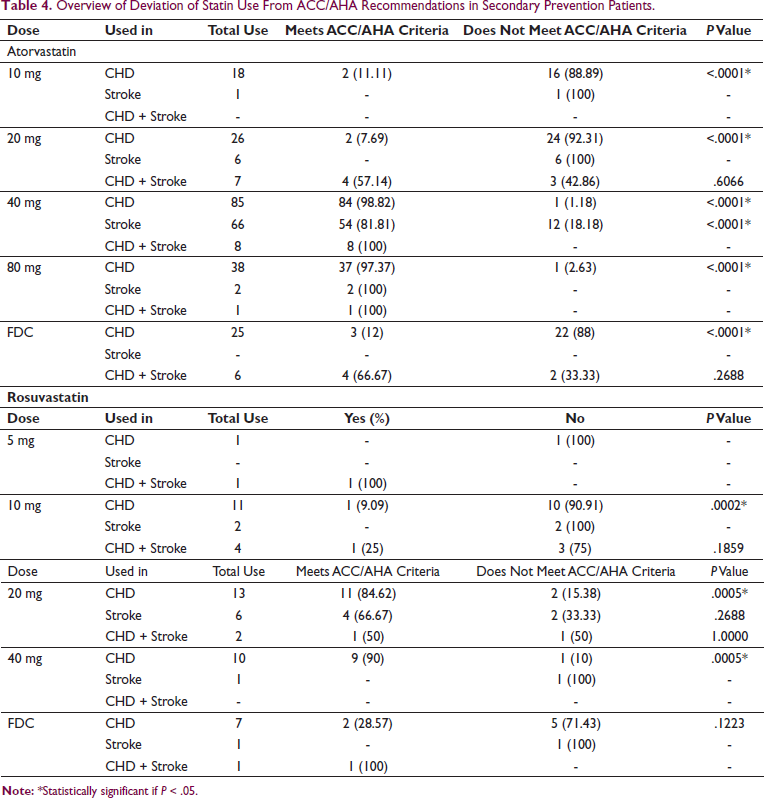
Use of low-intensity or moderate-intensity statins for secondary prevention suggests underdosing among these statin users as the ACC/AHA guidelines recommend the use of high-intensity statins for secondary prevention unless the patient requires dose reduction due to intolerable or life-threatening side-effects (Table 4).
Overview of Deviation of Statin Use From ACC/AHA Recommendations in Secondary Prevention Patients.
Discussion
This study evaluates statin use by patient characteristics, dosing, and rationale of statin dosing. High prevalence of diabetes and hypertension in the study population suggests the rising burden of these CVD comorbidities and the expected surge in statin use. According to several studies, the prevalence of hypercholesterolemia, hypertriglyceridemia, low HDL-C, and high LDL-C is 13.9, 29.5, 72.3, and 11.8%, respectively, in representative samples from all areas and ages. 6 Recent studies have reported that high cholesterol is present in 25% to 30% of urban and 15% to 20% rural subjects. 7 Statins have lipid lowering and number of pleiotropic effects such as improving endothelial functioning by upregulating endothelial nitric oxide synthesis, stabilization of plaque, and inhibition of endothelial injury caused by macrophage migration, phagocytosis, and foam cell formation. Given the therapeutic benefits and high prevalence of comorbidities contributing to CVDs, utilization of statins is expected to be high. 5 Atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin, and pitavastatin are the different types of statins marketed for clinical use. The utilization pattern of statin use in this study suggests atorvastatin and rosuvastatin are the commonly used statin products, with higher use of atorvastatin among the 2 commonly used statins. 11 This is supported by a recent study done using survey of prescribing physicians suggesting maximum utilization of rosuvastatin and atorvastatin. Similar findings were observed in this study. Wide market availability of atorvastatin products with affordable pricing of the drug and well-known lipid-lowering benefits may be associated with higher use or prescriber preference for atorvastatin.5, 12 Also in many studies, atorvastatin was found to be more effective in lowering serum LDL levels and preventing major adverse cardiac events and also in controlling the inflammatory process and relatively better tolerated when compared to other statins. 13
High use of fixed-dose combination products may suggest the prescriber’s preference to improve patient adherence. These findings are well-supported with previously published statin utilization studies in India.5, 9, 12, 14, 15 Also, in a study by Lolwa Barakat et al 16 in patients with hypertension and diabetes, atorvastatin and rosuvastatin were the preferred statins for primary and secondary prevention. Similar results were seen by Wander et al 9 where atorvastatin was preferred over rosuvastatin (72.9%, 54.6% vs 32.4%, 46.7%) for primary and secondary prevention, respectively. This may be due to the influence of cost, proven effectiveness, 5 easy availability, and large-scale production of atorvastatin in Indian markets. 12
For primary prevention, atorvastatin 20 mg was preferred while atorvastatin 80 mg was the least prescribed, whereas rosuvastatin 5 mg and 10 mg were the most prescribed.
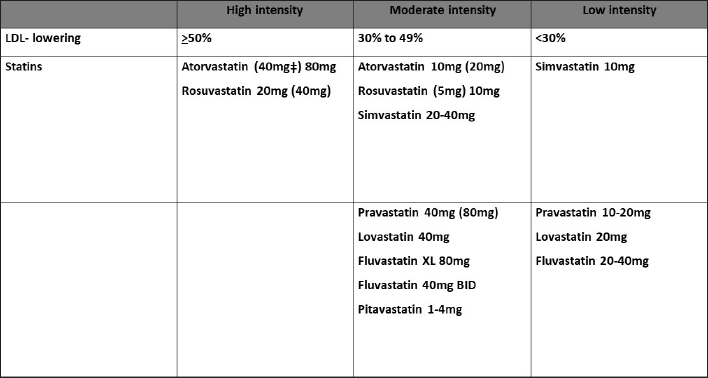
These dosing patterns observed for primary prevention are in agreement with the AHA/ACC guideline which is shown in Figure 3. Among secondary prevention, patients using atorvastatin 40 mg and rosuvastatin 20 mg were observed to be highest. These dosing patterns meet the standard prescribing guidelines; however, underdosing was observed among statin users. While lower dosing for secondary prevention was justified in some patients due to intolerable side-effects such as muscle pain or elevated liver enzymes, approximately 89% of atorvastatin 10 mg used for secondary prevention was not justified indicating substantial underdosing. This may lead to inadequate effectiveness and risk for CVD. Indians as compared to Caucasians may achieve higher blood levels of statins; however, the effect of these higher levels on the effectiveness of the drug, especially at lower than recommended doses, is not known. 5
High-, Moderate-, and Low-Intensity Statin Therapy Use.
Lower than recommended dose was a predominant prescribing error observed in this study (Figure 3). This could indicate a lack of evidence-based prescribing and inadequate utilization of risk scores. High risk for CVD and underdosing of statin therapy are suggestive of targeted interventions such as enhancing the use of standard prescribing guidelines, promoting evidence-based prescribing among prescribers which include use of risk-assessment scores, dosing, and treatment monitoring for safety and effectiveness.
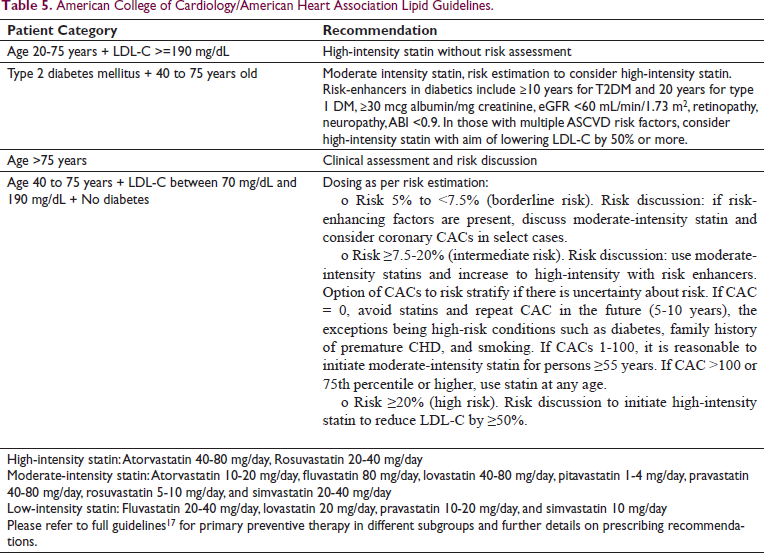
This study highlights the areas in clinical practice that can be intervened for better prescribing of statins. Increase in use of risk scores and adherence to dosing as per patient’s needs may improve the overall statin utilization. While the guidelines continue to recommend use of high-intensity statins for secondary prevention, the updated 2019 guidelines on statin dosing for primary prevention emphasize patient-physician shared decisions and provide additional guidance on dosing within subgroups such as those with severe hypercholesterolemia, diabetes, hypertension, chronic kidney disease, and so on (Table 5, Figure 3). 17
American College of Cardiology/American Heart Association Lipid Guidelines.
Conclusion
Although several types of statin products are marketed, atorvastatin and rosuvastatin are the preferred choices among prescribers. The use of fixed-dose combinations is highly suggestive of the prescriber’s preference to improve patient adherence; however, the prescribers should be cautioned about the hazards of underdosing that come with the use of fixed-dose combination therapies. Dosing criteria were well-achieved among secondary prevention as compared to primary prevention patients. Lack of use of risk-assessment tools is suggestive of underdosing or no use of statins among primary prevention patients. Promoting evidence-based prescribing may help to rationalize the use of statins and improve treatment outcomes and may help to reduce the rising burden of CVD in India.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.