
Abstract
Case of wide QRS tachycardia discussing differentiation of supra ventricular tachycardia with aberrancy from ventricular tachyarrhythmia.
Case
47-year-old female with left ventricular (LV) dysfunction and history of shortness of breath class 3 was referred for CRTP implantation. Her resting electrocardiogram (ECG) at presentation and on follow up showed short RP wide QRS left bundle branch block morphology (LBBB) tachycardia with ventriculo atrial and atrioventricular (VA/AV) association and negative P waves in inferior leads. Echo showed dilated left ventricle global hypokinesia with moderate LV dysfunction. We considered possible differential diagnosis of AVNRT with aberrancy, orthodromic AVRT with aberrancy, antidromic AVRT, ectopic atrial tachycardia with 1st degree atrioventricular (AV) block, intraventricular conduction defect (IVCD) type LBBB, and slow ventricular tachycardia with retrograde ventricular atrial (VA) conduction. she was further evaluated after informed consent (no ethical committee consent taken as it is essential diagnostic maneuver). Coronary angiogram and diagnostic electrophysiological study was performed. Coronary angiogram revealed normal coronaries. Diagnostic electrophysiological study revealed ventricular tachycardia with 1:1 retrograde VA conduction. She is planned cardiac MRI to rule out any structural abnormality followed by radio frequency ablation in view of incessant arrhythmia causing tachycardiomyopathy.
Discussion
All patients with wide QRS tachycardia with LV dysfunction need to be analyzed critically and need to confirm diagnosis to avoid mismanagement. Here patient presented with wide QRS tachycardia with LV dysfunction. ECG of all patients needs to be analyzed critically following Brugada algorithm 1 / Vereckei algorithm 2 to accurately diagnose SVT with aberrancy/VT.
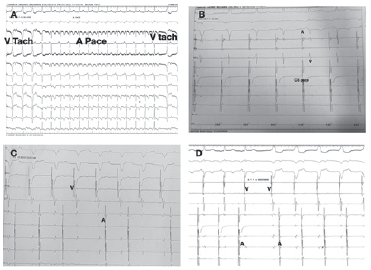
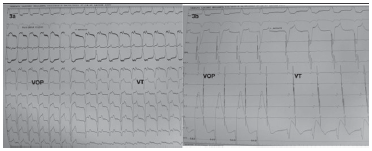
Here the only rhythm seen outside electrophysiology lab is wide QRS tachycardia suggestive of either SVT with aberrancy (AVNRT with aberrancy, orthodromic AVRT with aberrancy, antidromic atrioventricular reentrant tachycardia (AAVRT), atrial tachycardia with 1st degree AV block with aberrant conduction) or Ventricular tachycardia. Though there is no AV dissociation and QRS complexes are looking like LBBB morphology, systematic analysis of ECG following Brugada algorithm and Vereckei algorithm is suggestive of ventricular tachycardia which was confirmed by electrophysiological study. Atrial override pacing revealed AVVA response with continuation of tachycardia which is suggestive ventricular tachycardia (Figure 1A). ECG showed narrow QRS by ventricular activation through His-Purkinje system during atrial overdrive pacing with reversal to ventricularcular tachycardia immediately after pacing. Ventricular overdrive pacing revealed VAV response with continuation of tachycardia (Figure 2).
(A) Overdrive atrial pacing from CS 9,10 revealed narrow QRS rhythm in 12 lead suggestive of recruitment of conduction system and AVVA response. (B) Intracardiac egg showing overdrive pacing from CS 7,8 revealed narrow QRS due to ventricular activation through His-Purkinje system. (C) Overdrive ventricular pacing showing VA dissociation. (D) RA entrainment showing AVVA response confirming ventricular rhythm/tachycardia.
Ventricular overdrive pacing of VT with continuation of tachycardia post entrainment.
AVNRT/OAVRT with aberrancy, AAVRT, and Atrial tachycardia with aberrancy were ruled out and ventricular tachycardia was confirmed during EP study.
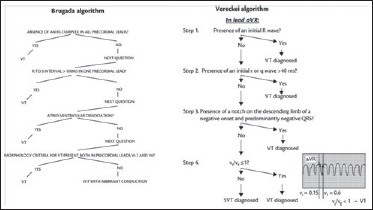
As per Brugada algorithm (Figures 3 and 4), absence of RS complexes in precordial leads even with precordial leads lowered by 1 ICS to V5, V6 is suggestive of ventricular tachycardia. Pseudo delta wave in V3 (atypical of LBBB) and R to S interval>100 msec suggest ventricular tachycardia though there is VA association. Lead V6 showing QS complex favors slow ventricular tachycardia than SVT with abberrancy as per last step of Brugada algorithm.
Brugada and Vereckei algorithms showing discrimination of SVT and VT in wide complex tachycardia.
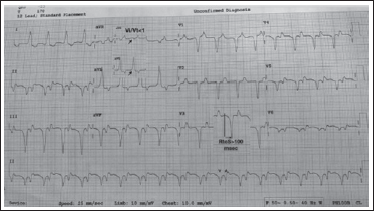
ECG showing wide QRS short RP LBBB morphology rhythm with negative P waves in inferior leads suggesting ventricular rhythm with retrograde VA conduction and VA association.
Even by application of Vereckei algorithm, notching on descending limb of QS in aVR and Vi/Vt<1 (Figure 3) is suggestive of ventricular tachycardia.
Though VA dissociation is commonly seen and suggest ventricular tachycardia, VA association is seen in slow VT with preserved VA conduction.
QRS complexes during tachycardia showing QS complexes from V1-V6 with small R in V2 and Qs in inferior leads with pseudo delta in inferior leads are suggestive of localization to apical crux / LV apical septum. Presence of LBBB with early transition in V2 followed by late transition RS or QS in V6 suggests apical crux origin. In this ECG, V1 showed QS with small r in V2 followed by QS from V3-V6 favoring localization to apical crux.
As echocardiography is showing global hypokinesia with moderate LV dysfunction, we planned contrast enhanced cardiac MRI to rule out any structural abnormality and consider RF ablation. Idiopathic apical crux VT can be mapped and ablated either from middle cardiac vein or epicardial approach. LV apical septum can be mapped and ablated through antegrade or retrograde approach in left ventricle.
Hence ECG needs to be analyzed using various algorithms to confirm diagnosis in such scenarios to avoid mismanagement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.