
Abstract
Background
Myocardial perfusion imaging (MPI) stress test is performed either using exercise as a stress modality or through the use of pharmacological vasodilator agents in those who cannot exercise. Regadenoson and dipyridamole are some of the most common vasodilator agents used. We aim to study the effect of these agents on the heart rate and the imaging results.
Methods
This was a retrospective study which included 187 patients with left bundle branch block. Patients received either dipyridamole or regadenoson during the myocardial perfusion imaging stress test. Charts were reviewed, and patient characteristics were recorded, as well as baseline heart rate, peak heart rate during stress, and angiographic data if available.
Results
Regadenoson increased peak, absolute and relative heart rates significantly more compared to dipyridamole. The peak heart rate for Regadenoson was 94.1 ± 17.36 and for dipyridamole it was 85.38 ± 16.48 BPM (P < 0.001). The relative and absolute heart rate increase in the regadenoson group were 40.75 ± 23.01% and 26.06 ± 13.44 BPM, respectively. The relative and absolute heart rate increase in the dipyridamole group were 24.61 ± 18.25% and 16.23 ± 10.97 BPM. The frequency of reversible septal defects was similar in both groups (54% for Regadenoson vs. 63% for Dipyridamole; P = 0.24).
Conclusions
There is a statistically significant increase in heart rate with the use of regadenoson for MPI compared to dipyridamole. However, the number of septal perfusion defects was similar between the two groups. The effect of this increase in heart rate, while statistically significant, is likely of no clinical significance.
Introduction
Myocardial perfusion imaging (MPI) using single photon emission computed tomography (SPECT) serves an important role as an imaging modality in cardiovascular medicine. It can provide necessary information regarding the diagnosis and prognosis of coronary artery disease (CAD). It also has utility in determining myocardial viability. MPI is not a perfect tool, however. Like other imaging modalities, it may be subject to numerous artifacts. Artifacts may arise from patient-related variables, imaging technique, equipment or image processing post acquisition. 1 It is important for the physician interpreting the images to be aware of the possible artifacts that may be present to improve the diagnostic accuracy of the test.
A left bundle branch block (LBBB) may produce a partially reversible or fixed septal defect on perfusion imaging. 2 This perfusion defect is usually tachycardia-induced. The proposed mechanism for this occurrence is not fully understood but it is thought to be due to reduced diastolic blood flow caused by delayed septal contraction. The blood flow is further compromised if the heart rate (HR) is increased since the duration of diastole is shortened. 3 For this reason, it is customary to select stress tests that do not promote tachycardia in patients with LBBB. Specifically, exercise and dobutamine stress MPI are not recommended in this population. 4
Adenosine, dipyridamole and regadenoson are common agents used in pharmacological stress MPI. Regadenoson increases HR more than adenosine and dipyridamole. 5 The mechanism for tachycardia is likely due to sympathoexcitation rather than a baroreflex since regadenoson increases serum norepinephrine and epinephrine levels. 6 The HR response is blunted in diabetic patients possibly due to sympathetic denervation, thus supporting the sympathoexcitation hypothesis. 7
Early studies comparing dipyridamole or adenosine to exercise stress MPI in patients with LBBB have confirmed that false positive septal defects are more common with exercise stress MPI due to tachycardia.8,9 As a result, the 2012 guidelines for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease provide a class I recommendation for pharmacological stress with either nuclear MPI or echocardiography for risk assessment in patients who have LBBB on ECG, regardless of ability to exercise to an adequate workload. 10 Considering regadenoson promotes tachycardia more so than dipyridamole or adenosine, physicians may be inclined to avoid its use in patients with LBBB to decrease its potential to create false positive perfusion defects.
We conducted a retrospective study in patients with LBBB to determine if there was a significant difference in the HR response between regadenoson and dipyridamole stress MPI and whether this led to more prevalent septal defects which, in turn, exaggerated the false positive rate of the studies.
Methods
We collected data retrospectively on a total of 187 patients with LBBB. All patients with LBBB who received regadenoson between 2010 and 2013 were included (total of 95). One patient was excluded due to unavailability of nuclear imaging data (total is now 94). We then included a similar number of patients from the period between 2013 and 2016 when our hospital switched from regadenoson to dipyridamole (total 93) Baseline characteristics including age at acquisition, gender, certain comorbidities and medications were collected. Information regarding their baseline HRs, peak HR, absolute increase in HR and relative difference in HR during stress testing were identified and calculated. MPI data were reviewed independently by two nuclear board-certified cardiologists. There was no disagreement between the two on all patients. A fixed defect was defined as a perfusion defect that was present with the same size and severity during rest and stress. A partially reversible defect was present if a perfusion defect was found at rest and noted to be worse during stress. This was evaluated using qualitative measures only. Semi-quantitative data such as summed stress score, summed rest score, and summed difference score were not gathered as we were interested in only one segment (the anteroseptal wall) which would be the one involved in false positive stress tests as explained above.
For the studies that were reported to have positive septal defects, data regarding coronary angiography were collected if performed. The presence of angiographically severe stenosis (defined angiographically as a stenosis of 70% or more, or a lesion with a fractional flow reserve of <0.80 if performed) in the left anterior descending artery (LAD) territory was documented. Septal defects were deemed to be false positives if angiography revealed noncritical CAD.
Regadenoson or dipyridamole protocol
All of the patients had fasted at least 4 h prior to the study and had no caffeine for at least 12 hours. All patients were brought to the nuclear laboratory where surface electrocardiography (ECG) leads were placed and vitals were measured and monitored throughout the study. An intravenous line was established or was checked for patency if already present. All the patients received 12 millicurie (mCi) of technetium-sestamibi (99mTc) for rest imaging and 34 mCi for stress imaging. This was injected intravenously. Rest and stress images were both ECG gated. After rest imaging was completed, the patients undergoing regadenoson MPI received a standard 0.4 mg of regadenoson bolus followed by a 10 milliliter (mL) saline flush. The 99mTc injection for stress imaging was given approximately 20 seconds later. The stress images were then acquired. In patients undergoing dipyridamole MPI, 0.142 mg/kg/min of dipyridamole infusion was administered over 4 minutes but did not exceed 60 mg. This infusion was also followed by a 10 mL saline flush. The 99mTc injection was administered 3–5 minutes later. Aminophylline was used to reverse persistent side effects with either protocol. Patients who were taking beta-blockers regularly only discontinued their medication prior to stress if the ordering physician instructed them to do so.
Statistical analysis
Statistical analysis was performed using IBM SPSS version 23. Student’s t-test was used for continuous variables and Chi Square Fisher’s Exact test was used for discrete variables. A P value less than 0.05 was considered significant.
Results
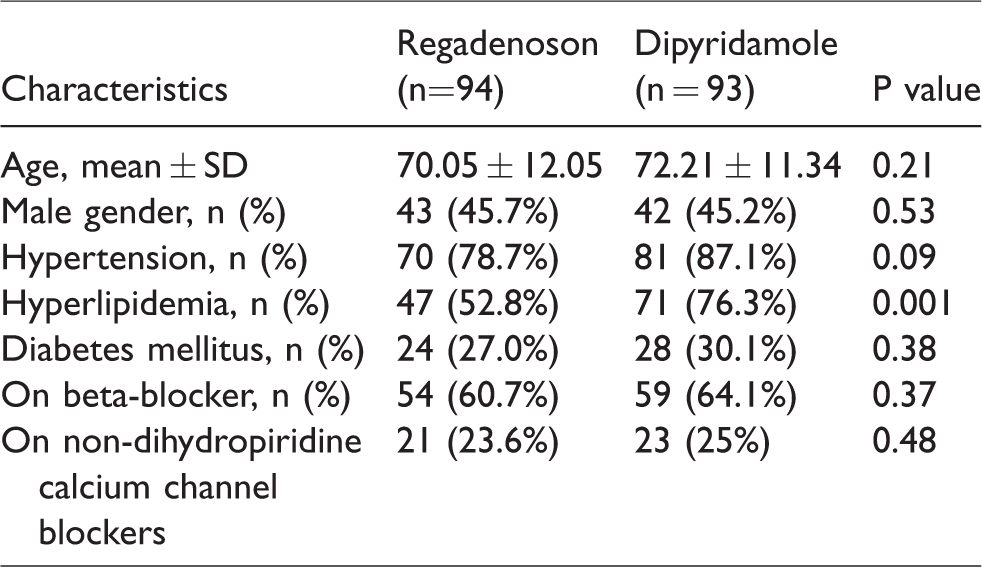
The baseline characteristics of each group are presented in Table 1. There was no statistically significant difference between groups when comparing age at acquisition, gender, comorbidities and medications (beta-blockers and calcium channel blockers (CCB)). Baseline characteristics including comorbidities and medications were unknown for five patients in the regadenoson group and one patient in the dipyridamole group. Baseline characteristics were similar in both groups except for the presence of hyperlipidemia (more patients in the dipyridamole group had baseline hyperlipidemia when compared to the regadenoson group, likely a chance effect).
Baseline characteristics.
The baseline HR was similar between the two study groups (P = 0.69). The baseline HR in the regadenoson group was 68.35 ± 14.42 beats per minute (BPM) whereas the baseline HR in the dipyridamole group was 69.15 ± 12.13 BPM. Regadenoson increased absolute, peak and relative HRs significantly more in comparison to dipyridamole. The peak HR for the two groups, regadenoson and dipyridamole, were 94.1 ± 17.36 and 85.38 ± 16.48 BPM, respectively (P < 0.001). The relative and absolute HR increase in the regadenoson group were 40.75 ± 23.01% and 26.06 ± 13.44 BPM, respectively. The relative and absolute HR increase in the dipyridamole group were 24.61 ± 18.25% and 16.23 ± 10.97 BPM, respectively. These findings are demonstrated in Table 2.
HR increase.

HR: heart rate.
The dipyridamole group had more partially reversible septal defects (63.4%) than the regadenoson group (54.3%). This did not achieve statistical significance, however (P = 0.24). Of the patients who underwent coronary angiography for the partially reversible septal defect, there was a trend towards more false positive septal defects in the regadenoson group (93.8%) than the dipyridamole group (72.2%). This finding also did not achieve statistical significance (P = 0.18). These results are displayed in Table 3.
Partially reversible septal defects.
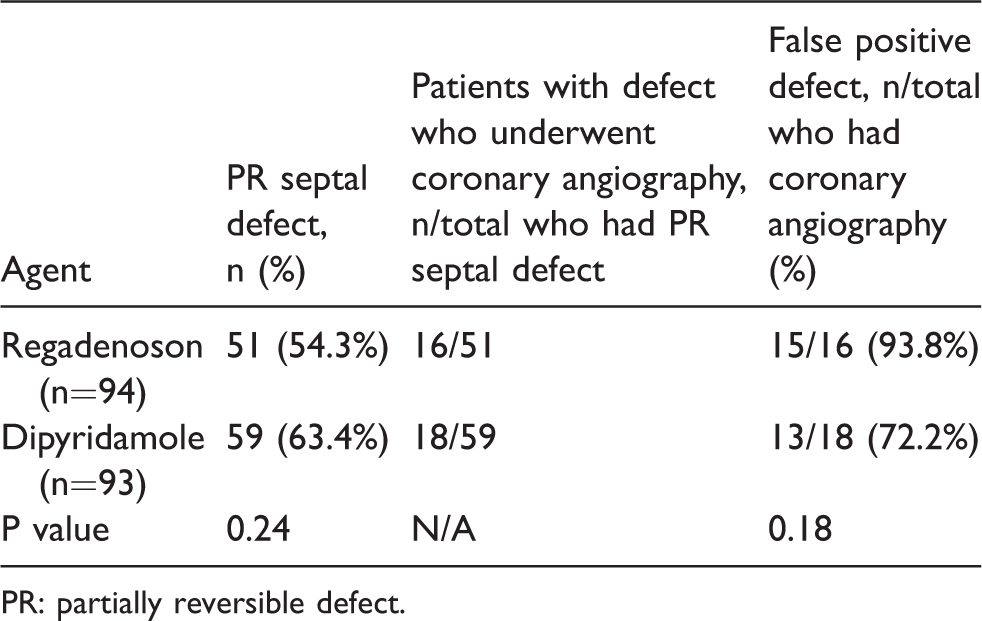
PR: partially reversible defect.
Discussion
In this study comparing regadenoson and dipyridamole use in MPI in patients with LBBB, regadenoson significantly increased the HR compared to dipyridamole. Although septal defects were encountered in both groups, only a limited number of patients further underwent coronary angiography. Of those who did, there were more patients with normal coronaries in the regadenoson group. However, due to the small number of these patients, it is difficult to draw any meaningful conclusion. We believe there was significant referral bias by the patients’ physicians who believed the perfusion defects were due to the existing LBBB and as such decided not to perform coronary angiography.
The conduction system of a normal heart originates at the sinoatrial (SA) node and then travels through the right atrium to the atrioventricular (AV) node. From there, the impulse proceeds through the septum along the right and left bundle branches to the right and left ventricles. If there is an LBBB, the impulse cannot pass through the left bundle. The left ventricle then receives conduction from the right ventricle resulting in signal delay. This produces a paradoxical septal motion where the septum moves toward the right ventricle during systole prior to moving leftward and contracting. Diastolic blood flow is presumed to be compromised due to delayed septal contraction. 3 This produces a septal defect on exercise MPI which can resemble a myocardial infarction or ischemia since the defect may be fixed or partially reversible. 2 The blood flow is further diminished if the HR increases since this leads to a shorter duration of diastole. The septal defect is then more likely to be detected. This phenomenon can also be present in patients with ventricular pacing because they exhibit a similar delay in septal contraction. 11
Consequently, it is recommended to avoid significantly increasing the HR in patients with LBBB undergoing MPI such as in exercise or dobutamine stress MPI to minimize the likelihood of false positive septal defects. Instead, other pharmacological agents that cause coronary vasodilation are used to minimize tachycardia. Studies in the past have confirmed that adenosine and dipyridamole are superior to exercise stress in patients with LBBB for this reason.8,9 The evidence has been adapted into the guidelines for stress testing.4,10 Adenosine activates all four adenosine receptors. Dipyridamole inhibits the uptake and metabolism of adenosine. Both of these agents serve as non-selective adenosine receptor agonists. Therefore, while they increase coronary vasodilation and blood flow via the A2A receptors, they also may cause bronchoconstriction through the A2B and A3 receptors and negative chronotropic, inotropic and dromotropic effects via the A1 receptor. Regadenoson is the only food and drug administration (FDA)-approved selective A2A receptor agonist which causes both coronary vasodilation and sympathoexcitation. This increase in sympathetic activity makes tachycardia a more common side effect of regadenoson than adenosine or dipyridamole. 6 However, it has been shown to have similar diagnostic accuracy for coronary artery disease as adenosine. 12
There is no contraindication for the use of regadenoson for MPI in patients with LBBB per the package insert. 13 While our study revealed that the increase in HR was more statistically significant in the regadenoson group than the dipyridamole group, this did not, however, translate into higher septal perfusion defects in that group. Two studies comparing regadenoson to adenosine in patients with LBBB or pacemakers that were undergoing MPI were reported. In those studies, the patients served as their own control as they underwent an initial adenosine MPI followed by a subsequent regadenoson study. One study revealed that patients with LBBB who received regadenoson had a statistically significant increase in HR compared to those who received adenosine. 14 That study however showed no significant difference in the number of septal perfusion defects between the two groups. The second study showed no significant difference between regadenoson and adenosine in inducing tachycardia, and similar to the first study, they concluded there were no differences in the perfusion patterns between those receiving Adenosine vs. Regadenoson. 15 Our study adds evidence in regards to the difference in increase in HR between dipyridamole (and indirectly, adenosine) and Regadenoson, however, it also confirms that this finding does not translate into a significant difference in perfusion patterns that pertain to LBBB.
In our study, the number of patients who subsequently had angiography after testing were limited. While there was a trend towards more false positive septal defects in the regadenoson group, this did not reach statistical significance. This is likely due to the small sample size of the study, making it potentially underpowered to show such difference. Larger studies with greater sample sizes are necessary to determine if regadenoson indeed produces more false positive septal defects in patients with LBBB.
Conclusion
Our study revealed a statistically significant increase in HR with the use of regadenoson for MPI in comparison to dipyridamole. The number of partially reversible septal perfusion defects was similar however between the two groups. A limited number of these patients underwent angiography and in that small number, the rates of false positive findings was higher in the regadenoson group. This did not reach statistical significance however.
We believe that despite the concern with increased HR with the use of regadenoson, there appears to be no clinical implications, reflected by similar perfusion profiles to dipyridamole. Referral to angiography was low in both groups, likely due to referral bias from physicians who judged these defects to be due to LBBB and did not pursue further testing. We believe regadenoson can be safely used in patients with LBBB, and the increase in HR, while it can be statistically significant, is not a source of higher perfusion defects compared to dipyridamole.
Study limitations
The study is likely underpowered since less than 20 patients from each group underwent coronary angiography to determine whether their septal perfusion defects were true or false positives. An ideal study would be prospective and would aim at performing angiography on all patients with perfusion defects to further determine if it was false positive or not.
Footnotes
Authors’ note
Waiver of informed consent was approved by the Ascension Providence Hospital Institutional Review Board, because this waiver will not adversely affect the rights and welfare of the subjects; the research could not be practicably carried out without the waiver; and whenever appropriate subjects will be provided additional pertinent information. Waiver of HIPAA was approved. The protected health information involves no more than minimal risk to the subjects. The PHI will be stored and transmitted with password protected, encrypted drives and will be kept in locked cabinets. The PHI will not be reused or disclosed to any other person or entity, except as required by law, for authorized oversight of the research study, or for other research for which the use or disclosure of PHI would be permitted. The physical data will be shredded and/or electronic data will be deleted at the end of the research. The waiver of authorization will not adversely affect the rights and welfare of the subjects. The research could not practicably be carried out without the waiver of authorization.
Acknowledgements
We acknowledge the contribution and help from Nancy M. Jackson, PhD Medical Researcher, Medical Education
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ascension Providence Hospital Institutional Review Board, Southfield, MI. IRB Study # 1041292–1.
Guarantor
None.
Contributorship
None.