
Abstract
Hemoptysis from ruptured Rasmussen’s aneurysms is a not an uncommon source of bleeding (5-10%) in patients with active or previous tuberculosis. Previous reports describe the use of coils, glue, covered stents, and detachable balloons as part of the endovascular management of Rassmusen’s aneurysms. Although vascular plugs have been used in the management of other pulmonary aneurysms and pulmonary arteriovenous malformations, its use within the inflammatory milieu as well as architectural lung parenchymal changes of tuberculosis has not been reported. We report and describe, to our knowledge, the first case of successful management of a Rasmussen’s aneurysm with a vascular plug with good success.
Introduction
Hemoptysis in the setting of patients with both active as well as treated tuberculosis may be of varying aetiopathology. Hemoptysis from ruptured Rasmussen’s aneurysms is a not uncommon source of bleeding (5-10%) in this group of patients. 1 The advent of multidetector computed tomographic angiography (MDCTA) allows for enhanced detection of the source of bleeding as well as differentiating bronchial arterial vs pulmonary arterial sources of bleeding. 1 Emergency endovascular techniques are the preferred treatment modality in patients with life-threatening hemoptysis.
Previous reports describe the use of coils, glue, covered stents, and detachable balloons as part of the endovascular management of Rassmusen’s aneurysms.2, 3 Although vascular plugs have been used in the management of other pulmonary aneurysms and pulmonary arteriovenous malformations, its use within the inflammatory milieu as well as architectural lung parenchymal changes of tuberculosis has not been reported. 4 We report and describe, to our knowledge, the first case of successful management of a Rasmussen’s aneurysm with a vascular plug.
Case
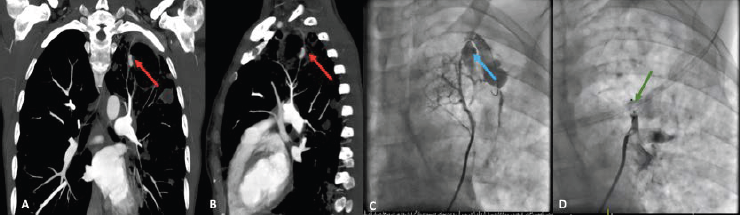
A 40-year-old female, HIV positive patient (CD4 count: 288 cells/µL) not currently on treatment and with confirmed active tuberculosis (tuberculosis polymerase chain reaction positive: rifampicin and isoniazid sensitive) presented with a single episode of massive hemoptysis (600 mL). MDCTA confirmed a large left upper lobe cavity with evidence of a Rasmussen’s aneurysm at the medial border of upper lobe cavity (Figure 1A). The aneurysm was noted to be originating from a left posterior subsegmental branch better seen on a sagittal view (Figure 1B).
Right femoral venous access was obtained and a 6 French sheath inserted under local anesthetic. Left main pulmonary artery injection using a pigtail diagnostic catheter (inserted over a 0.035 inch J-tip wire) revealed the culprit aneurysm. Selective engagement of the culprit feeding vessel (left posterior subsegmental pulmonary arterial branch) was achieved using a multipurpose guide catheter over a 0.018 inch Terumo® guidewire. Selective injection of the feeding artery of the aneurysm identified bleeding from the ruptured aneurysm (Figure 1C; Supplemental Video 1). A 4-mm Amplatzer® vascular plug 2 (based on sizing of the feeder artery) was then emergently deployed (Supplemental Video 2) within the feeding subsegmental branch with contrast injection into the offending feeding artery confirming cessation of anterograde flow prior to unscrewing the vascular plug from the delivery device (Figure 1D; Supplemental Video 3). Complete resolution of hemoptysis occurred and the patient was discharged on day 2 post procedure in a stable condition with no further requirements for intervention or blood transfusion during her stay.
Discussion
Rassmussen’s aneurysms can present with recurrent episodes of minor hemoptysis or life-threatening major hemoptysis. If not managed in a timely manner, mortality rates in the setting of major hemoptysis can exceed 50%. 1 Endovascular therapies in the management of Rassmussen’s aneurysms allow for rapid control of bleeding in these patients that are considered to be at high surgical risk.
The use of vascular plugs allows for rapid deployment and control of bleeding. Vascular plugs can be deployed using small caliber catheters (5-6 French) and the procedure can be performed under local anesthetic. Moreover, vascular plugs can be deployed in a controlled manner with precision in order to occlude proximal arteries which may be feeding the aneurysm.
The Amplatzer® vascular plug consists of a self-expanding nitinol mesh attached to a delivery wire with a micro screw. The vascular plug is delivered through the catheter which subselects the vessel one wishes to occlude. On release of the plug by unscrewing the microscrew, flow turbulence as well as the nitinol mesh promotes clot formation and rapid vessel occlusion. Our policy is to upsize the vascular plug by 20% in comparison to the feeder vessel. The delivery system of vascular plugs also allows an individual to retrieve and reposition the plug until final deployment of the vascular plug. In addition, the outward radial force offered by the Amplatzer® vascular plugs also reduces the chance of device migration.
We propose that the use of vascular plugs in the acute management of Rasmussen’s aneurysms should form part of the armamentarium available to interventional radiologists. Further research looking at the long-term success of such interventions will need to be carried out.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material sj-vid-1-occ-10.1177_26324636221118422 for Vascular Plugs—Novel Therapeutic Management of Hemoptysis Secondary to Ruptured Rasmussen’s Aneurysm? by Thadathilankal-Jess John, Michelle da Silva, Hellmuth Weich, in Indian Journal of Clinical Cardiology
Footnotes
Author Contributions
All authors were equally involved in the preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.