
Abstract
Takotsubo cardiomyopathy (TC) is a unique heart disease which mimics the clinical symptoms and features of acute coronary syndrome (ACS) and is seen more commonly in postmenopausal females. In this condition, abnormal electrocardiographic findings like ST-segment elevation/depression, T wave inversion, and an abnormal/absence of Q wave, along with echocardiographic disturbances like regional wall motion abnormalities and a sudden decrease in the ejection fraction are observed. However, coronary angiography shows no coronary artery obstruction. Interestingly, the left ventricle in TC develops a characteristic appearance similar to that of a “Tako-tsubo” (Japanese pot). Such peculiar observations become important when diagnosing TC in a clinical setting. TC is often caused by a catecholamine surge due to mass sympathetic activation usually preceded by an emotional/physical trigger, however the exact etiology and mechanism of pathophysiology still remain unclear. With growing awareness and prevalence of TC, it becomes crucial for clinicians to differentially diagnose TC from other heart conditions with the help of well-known diagnostic tools. Moreover, amidst the ongoing pandemic, the cytokine storm associated with COVID-19 may be accompanied with a catecholamine surge in the body, which in turn might increase the risk and incidence of TC in patients.
Keywords
Introduction
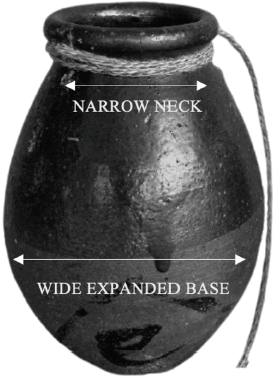
An increasing number of cases of TC have been reported in recent times which present with features imitating the cardinal signs and symptomatology of acute coronary syndrome (ACS). However, diagnostic tests and imaging techniques reveal no significant coronary artery disease (CAD). Moreover in TC, an abnormal shape of the heart is seen, resembling that of a “Tako-tsubo,” a traditional Japanese pot (Figure 1). Initially, identified as a case of reversible left ventricular wall motion impairment caused due to pheochromocytoma by Iga et al, 1 this cardiac disease was first described as “tako-tsubo-like left ventricular dysfunction” in Japanese population by Sato et al. 2 As of today, TC can be described as transient left ventricular apical ballooning and dysfunction without presence of obstructive CAD.3-5 It is also referred to as stress cardiomyopathy, apical ballooning syndrome, and, interestingly, broken heart syndrome in keeping with the etiology and clinical presentation. With increasing awareness, diagnoses, and importance of TC as a separate cardiac entity, it has been included in the fourth universal definition of myocardial infarction by the European Society of Cardiology (ESC). 6
Traditional Japanese “tako-tsubo” Octopus-Fishing Pot Depicting a Characteristic Shape and Appearance.
Prevalence and Epidemiology
The exact incidence of TC remains unknown due to paucity of data, a consensus definition, and/or universal diagnostic criteria(s). However, the prevalence of TC is estimated to be approximately 1% to 2% in all suspected cases of acute myocardial infarction (AMI).7, 8-10 It is reported that 79.1% patients with diagnosed TC are above 50 years of age, thus proving that age is a risk factor for this disease. 11 Moreover, TC accounts to a female-to-male ratio of 9:1, 12 indicating significant gender difference. Both prospective and retrospective studies have confidently shown that females are at a higher risk for developing TC,11, 13, 14 which is predominantly seen in the postmenopausal age group,15-17 possibly due to hormonal imbalances. Age-associated decline in estrogen levels seems to play a pivotal role here.18, 19 Furthermore, 89.8% of women affected with TC had a mean age of 66.8 years, 11 and it was also studied that women older than 55 years had a 4.8-fold higher risk of developing TC when compared with women younger than 55 years, 13 thereby showing the role of both age and gender as risk factors for TC.
Etiology
Most of the cases present with a history of stress, which may be either emotional or physical, and are identified as possible triggers of TC.7, 14 Emotional stressors are more potent causes of TC in women and may include negative life events such as death of a loved one, natural disasters, sudden bad news, financial loss, and others.3, 7, 12, 20 In contrast, physical stressors are seen to be the precipitating cause in men.3, 5, 7, 12 However, TC may also get precipitated as a result of positive events, and for this sake it has also been called as the “happy heart syndrome.” 21 It is seen that physical triggers were more common than the emotional ones (36.0% vs 27.7%). 11 Additionally, a recent study also showed that males were more prone to a trigger factor (92.6%) compared to females (81.9%, P < .001) wherein physical triggers were more common (67.3% overall, males 85.7%, females 63.5%, P < .001). 22 Also, females ≤50 years experienced more physical trigger factors (75.6%) as compared to females >50 years of age (59.3%, P < .01). 22 Studies have also revealed that TC may even occur in the absence of any sudden identifiable stressor.11, 14, 21 Even though the exact cause of TC remains uncertain, there is enough evidence to prove the role of excessive sympathetic activation and subsequent discharge leading to a catecholamine surge as the most obvious cause of this disease.7, 11, 23, 24
Pathophysiology
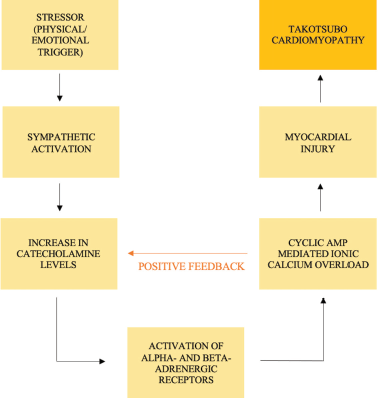
It has been observed that TC has a multifactorial pathophysiology which is contributed by excessive catecholamine surge, transient epicardial coronary artery spasm, endothelial dysfunction, microvascular impairment, oxidative stress, left ventricular outflow tract obstruction, and reversible myocardial stunning.9, 12, 23-27 A crucial factor playing a role in the pathophysiology of TC is sympathetic activation in response to a preceding trigger which leads to an excessive release of catecholamines through the hypothalamus-pituitary-adrenal axis.9, 11, 12, 23, 24, 26, 27 Catecholamines activate alpha- and beta-adrenoreceptors resulting in myocardial damage through increased ionic calcium, which, itself, in turn also leads to a catecholaminergic release,24, 26, 28, 29 thereby establishing a positive feedback cycle (Figure 2). Studies have also elaborated on the role played by cyclic AMP (cAMP)-mediated calcium overload in the myocytes as an important factor in the pathogenesis of catecholamine-toxicity and subsequent cardiac dysfunction.9, 28-30 Another study also showed that exposure to catecholamines and beta-receptor agonists can aggravate the onset of TC, 31 thus implying the primary role played by the same. Moreover, plasma levels of epinephrine and norepinephrine are found to be significantly elevated in the acute phase of TC, 30 and these levels were seen to be 2 to 3 times higher in comparison to those in AMI in Killip class III cases. 24 This knowledge may aid in differential diagnosis of TC. Finally, these levels decreased to about one-third of their initial spike levels in approximately 1 week, 24 indicating the possible reversible nature of TC.
Pathophysiology of Takotsubo Cardiomyopathy: Role Played by Catecholamines and Calcium Overload Mediated Positive Feedback Mechanism.
Clinical Presentation
Patients of TC present with chest pain (75.9%) and dyspnoea (46.9%) as the most common symptoms. 11 Other symptoms may include syncope, palpitations, cardiogenic shock, and less commonly nausea and vomiting, hypotension, pulmonary oedema, ventricular arrhythmias, and acute heart failure,4, 11, 12 thus often confusing TC with ACS. Although some patients may be completely asymptomatic earlier, 4 TC may be diagnosed later upon further investigations.
Diagnostic Criteria
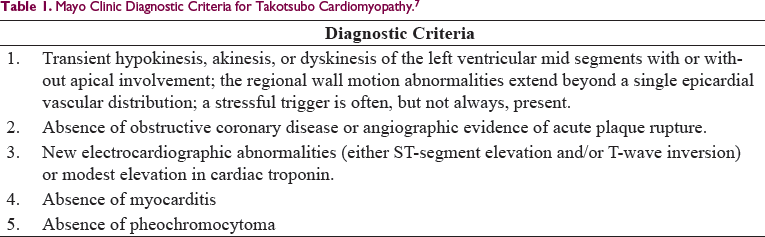
Mayo Clinic Diagnostic Criteria for Takotsubo Cardiomyopathy. 7
More recently in 2018, the ESC established the International takotsubo (InterTAK) diagnostic criteria which consists of an algorithm of variables assigned to specific scores to enable clear identification for diagnosis of TC. 32 However, being a newly recognized medical condition, there is no universally accepted criteria for efficiently diagnosing TC to date.
Variant forms of TC exist, which have been broadly classified into typical and atypical forms.7, 9-11, 33 The most typical and common presentation is the classical “apical ballooning” of the left ventricle (LV) (81.7%), and less common atypical forms include the midventricular (14.6%), basal (2.2%), and focal (1.5%) variants. 11 “Reverse takotsubo” is an atypical presentation of TC wherein there is “apical sparing” of the LV and instead involvement of other parts of the myocardium depicting varied patterns involving mostly the mid and basal segments of the LV leading to certain regional wall motion abnormalities (RWMA) and contractile dysfunction.9-11 These variants of TC occur in a minority of patients and have a similar clinical presentation to the classical TC.7, 9, 11 Knowledge of these variants is important in accurate diagnosis and subsequent management of TC in different patients.
Differential Diagnosis
Proper knowledge and understanding of various well-known methods and investigations used on a routine-basis in a clinical setup can be employed to help in correctly diagnosing TC and clinically differentiating it from other cardiac diseases, the most important one being ACS.
Biomarkers
Biomarkers like troponins and creatine kinase-MB fraction often show increased serum levels in TC but less as compared to those in ACS.12, 30, 34 On the contrary, brain natriuretic peptides (BNP or NT-proBNP) are significantly elevated in most of the cases of TC, much more than in patients with ACS.7, 12, 30, 34, 35 Furthermore, biochemical ratios like hs-TnT/CKMB, proBNP/myoglobin, and NT-proBNP/troponin T also need to be closely examined as important factors for diagnosis of TC. 36
ECG Findings
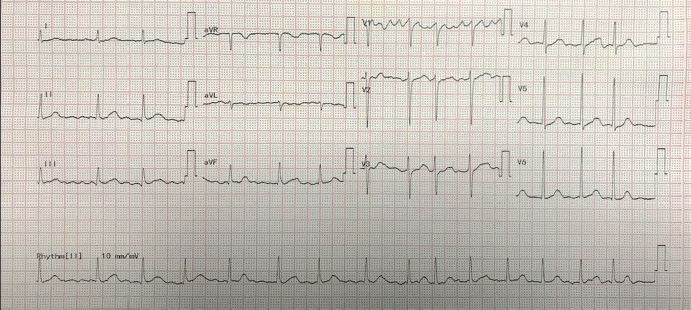
In the acute phase of TC, abnormal electrocardiogram (ECG) findings are recorded which are similar to that of ACS.11, 37 These mostly include ST-segment elevation or depression (uncommon), widespread and progressive T wave inversion (may be global), QT interval prolongation, and an abnormal/absence of Q wave.7, 11, 12, 24, 30, 37, 38 Different criteria have also been proposed to differentiate TC from STEMI/NSTEMI37, 39 alongside knowledge of the varied ECG abnormalities in different leads12, 30, 37, 39, 40 which also need to be considered for precise diagnosis. However, it is observed that in some cases the ECG findings do not show any kind of an abnormality which might be suggestive of AMI (Figure 3).
Imaging Techniques
Coronary Angiography
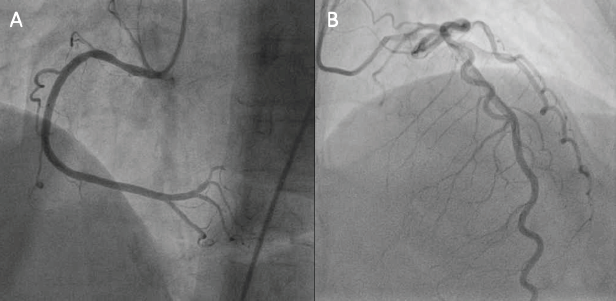
Suspected cases of TC should undergo angiography to distinguish it from ACS and CAD, as it is the gold standard.3, 23, 41 Obstructive CAD can only be ruled out if luminal stenosis is less than 50%. 23 In most cases of TC, the coronary arteries appear normal 11 (Figure 4); however, it has been found that in 10% of the cases, mild or moderate CAD may be detected. 23 Additionally, cardiac ventriculography helps in detection of RWMA extending beyond single branch distribution of epicardial coronary arteries, which is known to be an important hallmark feature differentiating TC from ACS. 42 Moreover, biplane left ventriculography is found to be more advantageous in comparison to single plane due to a more enhanced field of vision. 42
Echocardiography
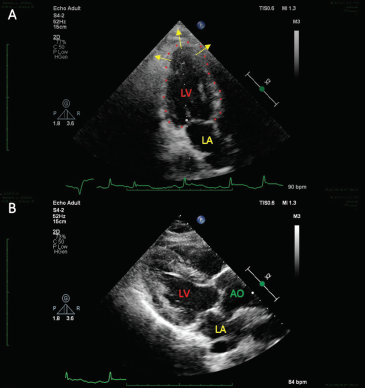
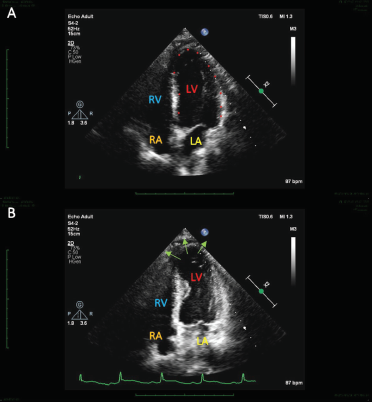
Echocardiography is a valuable investigation for in-depth analysis of TC, also being a good predictor for assessment of its adverse complications.41, 43, 44 This technique helps in differentiating TC (86.5%) from ACS (54.2%) on the basis of the magnitude of decreased left ventricular ejection fraction (mean value, 40.7 ± 11.2%). 11 More importantly, characteristic ventricular wall motion abnormalities like circumferential wall motion deformity, apical hypokinesia and basal hyperkinesia, and other RWMA are also observed.4, 41, 43 Thus, echocardiography proves to be useful in differentiating between distinct variants of TC, while also appreciating the characteristic apical ballooning/“Pot-like” shape of LV in various different views (Figures 5 and 6).
Cardiac Magnetic Resonance (CMR) Imaging
CMR needs to be performed in the subacute phase of TC (usually in the first 24-48 h), because anatomical and functional abnormalities of TC may revert back in 4 to 8 weeks.45, 46 Myocardial oedema is often seen in apical and mid ventricular planes which indicate LV dysfunction 46 and favor TC diagnosis. Due to its higher resolution and finer visualization, CMR helps in discerning the distinct forms of TC as well as differentiating it from other cardiac problems like ACS and myocarditis.30, 46, 47
Associations
An increased risk and prevalence of TC is found in subarachnoid hemorrhage and certain neurological and psychiatric disorders.16, 48 It was also shown that stress- and depression-related mRNAs were found to be upregulated in patients with TC, indicating possible neuropsychiatric associations. 49 In addition, certain comorbidities exacerbate the onset of TC which includes pulmonary and kidney diseases, sepsis, acute pancreatitis, hypothyroidism, and malignancies.3, 50
Complications and Outcomes
In-hospital complications include acute heart failure with/without pulmonary oedema, atrial and ventricular arrhythmias, acute mitral regurgitation, stroke, cardiogenic shock, and free-wall rupture, which occur as a result of either electrical or hemodynamic homeostatic disturbances.11, 23, 51-53 The neurohormonal network consisting of various parts of the autonomic nervous system are seen to be affected in TC.54, 55 This may possibly increase the risk for developing cerebrovascular diseases.
According to a meta-analysis, the in-hospital mortality rate among TC patients was found to be 4.5%, out of which 38% of deaths occurred as a direct consequence of TC-induced complications. 56 However, the long-term mortality data seems to be insufficient and needs to be studied further. It was also seen that male patients have a threefold higher death rate 51 in comparison to females, who instead seem to be more prone to TC recurrence. 57 Cases of recurrence may occur as early as 3 weeks or as late as several years after the initial presentation. 51 A retrospective study of TC cases (n = 100) showed that the recurrence of TC was 11.4% over a time period of 4 years. 58
Relation With COVID-19
Amidst the unprecedented outbreak of the novel SARS-CoV-2 virus worldwide, it has been found that the cardiovascular system is also affected.59-61 Harmful effects of the virus leading to cardiac dysfunction include myocardial injury, microvascular damage, stress leading to inflammation, vascular endothelial dysfunction, thromboembolism, and elevated biomarkers,59-63 which may possibly increase the predisposition of TC in patients. It is well known that a cytokine storm is triggered in patients with COVID-19 which might be accompanied with a catecholamine surge, and this may potentiate the onset of TC.62, 64, 65 Accordingly, an increasing prevalence of TC has been reported since the beginning of this outbreak.62, 64-66 Moreover in a study including 1,914 patients of ACS, a dramatic increase in the incidence of TC during the SARS-CoV-2 pandemic was found from an initial prepandemic range of 1.5-1.8% to 7.8% during the pandemic. 65 The psychosocial impact of this pandemic has been tremendous in adversely affecting the mental well-being of the community leading to cultivation of emotional and physical stress,67, 68 which are potential triggers of TC. Emerging literature also reports that severe cardiovascular-induced morbidity and mortality rates have also escalated during the COVID pandemic.61, 63
Management and Prognosis
Management strategy of TC in patients still remains debatable, however primary care should include supportive treatment which should aim at stabilizing the patient and preventing fatal complications.11, 69 Being an “ACS mimicker”, the standard line of treatment should include administration of beta-blockers, inotropes, angiotensin converting enzyme inhibitors, antiplatelets unless contraindicated, diuretics with continuous ECG monitoring, and in cases of cardiogenic shock an intra-aortic balloon pump may also be used.3, 4, 11, 51, 69, 70 The use of beta-blockers however remains controversial in the acute phase of TC9, 71 and also in preventing the recurrence of TC,72, 73 but still beta-blockers are a primary choice of physicians in this condition. Considering estrogen plays a key role in TC, supplementation may help in this problem, especially in postmenopausal women, though there are no clinical trials proving the same in humans till date.9, 18 Apart from the above mentioned measures, efforts should be made to ameliorate any emotional/physical trigger that may continue to persist, hence psychological counselling and therapy is an option. Prognosis is generally favorable in most cases of TC,69, 74 with some exceptions wherein adverse outcomes may occur,74-76 hence continuous monitoring and regular follow-up becomes essential.
Conclusion
Despite having immense clinical importance, TC, a recently diagnosed cardiac disease, still remains a much under-recognized clinical condition in today’s medical scenario due to its close resemblance to ACS. The most familiar cause of TC is an emotional/physical stressor leading to a catecholamine surge, however the exact pathophysiology of TC remains inconclusive. With increasing knowledge and a growing prevalence in a community where state-of-the-art technologies may be available, it becomes imperative to correctly diagnose TC as a separate entity and also distinguish it from other cardiac conditions. Amidst the ongoing COVID pandemic, an association of TC with this virus has been found, however further medical research is needed to correctly establish this relationship, while justifying the existing data. Appropriate efforts will reflect positively on patient management and also help physicians in developing future treatment modalities for TC.
Limitations of Current Literature
There is no consensual definition, universal diagnostic criteria, and methods of assessment established for TC till date.
Due to lack of knowledge and paucity of data, the prevalence of TC still remains under-reported and the information regarding its clinical features and complications is incomplete.
Even though literature suggests that a catecholamine surge is the primary cause of TC, there still exists a need for correctly investigating catecholamine’s role in its causation.
There is little awareness of TC as a rare cardiac condition among clinicians. Hence, there is an even greater requirement for overcoming this problem to aid in the differential diagnosis of TC.
Associations of TC with other diseases and its relation with long-term mortality is not very clear as studies done in this field are performed in highly selective and varied populations.
Finally, there is no standard line of treatment and set guidelines to be followed for managing TC in a clinical setting.
Footnotes
Authors’ Contributions
RK: Conceptual idea, contributed integral subject-related details, accuracy and integrity of collected data, analysis and interpretation of results, topic-related clinical contribution, editing and review of manuscript; ASW: Conceptual idea, data collection, draft compilation, analysis and interpretation of results, technical details and editing, manuscript preparation and submission; ASB: Data collection, draft compilation, analysis and interpretation of results, technical details and editing, manuscript preparation and submission; VPS: Accuracy and integrity of collected data, topic-related clinical contribution, editing and review of manuscript; MKP: Draft compilation, topic-related clinical contribution, planning, supervision, coordination, editing and review of manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.