
Abstract
A 9-year-old boy presented with breathing difficulty and episodic palpitation. Cardiac evaluation revealed features suggestive of left atrial myxoma intermittently obstructing the left ventricular inflow in the echocardiogram. The tumor was removed surgically. Histopathology confirmed the diagnosis. Cardiac myxoma is very rare in pediatric age group. High degree of suspicion is required for the diagnosis and management.
Keywords
Description
A 9-year-old boy weighing 19 kg presented with acute onset of breathing difficulty and episodic palpitation. His heart rate was 100/min and oxygen saturation 98% on room air. Chest auscultation showed bilaterally equal vesicular breath sound. Cardiac examination showed normal first and second heart sound. No significant murmurs were heard during evaluation. There was no neuro deficit or evidence of any rash. Chest X-ray showed cardiothoracic ratio of 0.5 and normal pulmonary blood flow. Electrocardiogram revealed sinus tachycardia PR interval of 100 ms and left ventricular dominance. Echocardiogram showed a large pedunculated mass (35 × 27 mm approximately) attached to the interatrial septum and moving to and fro across the mitral valve. The mass was creating inflow obstruction of the mitral valve with mean gradient of 5 mm hg. There was mild tricuspid regurgitation and ventricular systolic function was good (Figure 1A-G). The echocardiographic features were suggestive of left atrial myxoma. The patient was taken for surgical removal of the mass. The tumor was seen as a reddish jelly-like mass. It was attached to the interatrial septum. It came out after gentle anesthetic bagging. The whole tumor mass was excised and sent for histopathology examination. The histopathology examination showed paucicellular myxoid material containing polygonal to stellate cells with eosinophilic cytoplasm, bland nucleoli with frequent myxoma cells. No mitotic activity was seen. The edge had a fibrotic rim and was covered with endothelium (Figure 2A-D). The postoperative period was uneventful. There was no remnant of tumor mass in the left atrium or any obstruction to mitral inflow. In the follow-up of 6 months, the child is doing well.
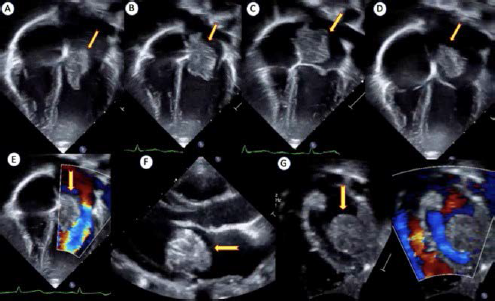
Echocardiogram in apical 4 chamber view (A-D) showing large pedunculated lobular myxoma attached to interatrial septum moving in different parts of the cardiac cycle partially obstructing the mitral inflow (E). Parasternal long axis (F) and subcostal short axis (G) view showing large tumor mass (arrow).
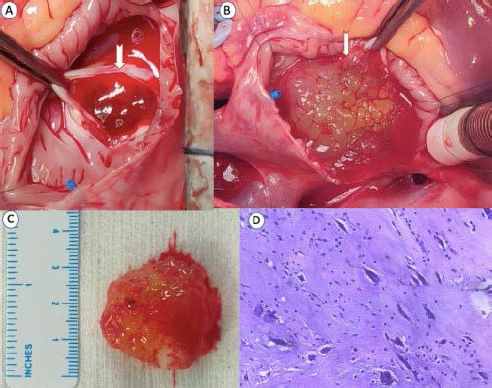
Operative image showing (A) jelly-like appearance of the tumor after atrial incision, (B) coming of the mass (arrow) after gentle anesthetic bagging, (C) the myxoma mass after complete excision, (D) histopathological appearance of paucicellular myxoid material containing polygonal to stellate cells with eosinophilic cytoplasm, bland nucleoli with frequent myxoma cell.
Primary cardiac tumors are rare in children, with an incidence ranging between 0.01% and 0.32%. Amongst the primary cardiac tumors, myxoma in the pediatric population is very rare, constituting up to 2% to 4% of the cardiac tumors unlike the adult population where it is more dominant. The classical triad of presentation is cardiac obstruction, embolism, and nonspecific systemic illness. Symptoms of intracardiac obstruction and heart failure followed by ischemic stroke dominate the presentation in children. Initial presentation with embolic symptoms mimicking collagen vascular disease is reported. Alert clinical suspicion about the possibility of cardiac tumors like myxoma in the pediatric age group specially for embolic stroke is very important. Echocardiography is the gold standard in the initial diagnosis which delineates the tumor mass. Complete surgical excision is usually curative with very less risk of recurrence.1-4
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical statement
Institutional ethical committee protocol of the organization allows publication of clinical case details of the patient where the details transmitted anonymously without any revelation of patient identity. Informed consent was taken from the parent.