
Abstract
Congenital pulmonary venolobar syndrome or infantile scimitar syndrome is a rare congenital cardiopulmonary anomaly and has variable presentation, especially in the neonatal period. It is characterized by partial or total anomalous pulmonary venous return from the right lung along with pulmonary hypoplasia. The infantile form is associated with significant mortality and has a worse prognosis due to severe respiratory insufficiency, cardiac failure, and pulmonary infections. We report an infantile scimitar syndrome diagnosed within few hours of life, which has been followed up for 4 years for the presence of intact survival and without neurodevelopmental disorder in the domains of motor, cognition, communication, personal-social, vision, and hearing.
Keywords
Introduction
In 1836, George Cooper and Raoul Chassinat individually reported single cases of rare congenital malformations that included venous drainage below the diaphragm. However, the word “scimitar” was not used. Almost a century later, EA Park in 1912 reported a similar case description of scimitar syndrome. It was Halasz et al in 1956 who was the first author that used the term “scimitar.” 1 Since then, several publications on infantile and adult forms of scimitar syndrome have been described.
Although the exact prevalence is unknown, it is estimated at between 1 and 3 out of 100,000 live births, with a 2:1 female predominance. 2 Scimitar syndrome is characterized by a combination of cardiopulmonary anomalies including partial anomalous pulmonary venous return connection of the right lung to the inferior vena cava (IVC) leading to a left-to-right shunt. 3 Without the presence of an abnormal pulmonary vein, that is, the scimitar vein, the pathology cannot be defined as scimitar syndrome. 4
The etiology is not completely understood. In several patients with total anomalous pulmonary venous return, the gene locus has been mapped to chromosome 4q12. 3 The pathogenesis of the syndrome is unclear, but it seems to originate from a basic developmental disorder of the entire lung bud early in embryogenesis. Two main forms of scimitar syndrome have been described. The infantile form is where signs and symptoms develop in the first year of life with tachypnoea, recurrent pneumonia, failure to thrive, and signs of heart failure. The childhood/adult form is where they become symptomatic beyond infancy. The diagnosis of scimitar syndrome is usually made based on characteristic features on chest x-ray films and further confirmation by chest computed tomography and angiography; however, it is now done mostly by transthoracic echocardiography or magnetic resonance angiography. 5
We conducted an extensive literature search, which included individual case reports and retrospective case studies on infantile scimitar describing their varied clinical presentation and the age at diagnosis. Few retrospective case studies focused on infantile scimitar syndrome and their related short-term outcomes.6, 7 However, their intact survival without neurodevelopmental disorder (NDD) has not been reported in medical literature. Hence, we highlight our case study as the first to report on the neurodevelopmental implications of an infantile scimitar.
Case Presentation
A 4-year-old girl was diagnosed to have scimitar syndrome within the first 24 h of life (day 1 of life). She was followed up closely with a keen interest regarding her neurodevelopmental and growth assessment.
Neonatal Period
A healthy term baby girl was born at 39 weeks of gestation by normal vaginal delivery after an uneventful antenatal course with birthweight at the 50th centile. Her parents were nonconsanguineous and family history was noncontributory. At 8 h of age, she developed tachypnea and chest retractions with frequent desaturations (88%-92% oxygen saturation) in the postnatal ward. She was subsequently admitted to the neonatal intensive care unit with a probable diagnosis of transient tachypnea of newborn. Her systemic examination was unremarkable except for heart sounds on the right side and a grade 2 ejection systolic murmur.
Diagnostic Assessment
Radiological
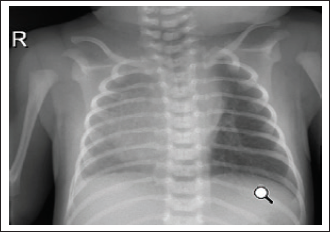
Chest x ray at the onset of respiratory distress showed dextroposition of the heart with low right lung volume (Figure 1).
Echocardiography
Echocardiography on day 1 of life (within 24 h of age) showed dextroposition, levocardia, and a large atrial septal defect (ASD) measuring 12 to 14 mm with a bidirectional shunt mainly left to right, partial anomalous pulmonary venous drainage (1 vein drains infracardiac to the IVC with no obstruction and 3 veins drain normally into the left atrium). Small patent ductus arteriosus was seen. It had good left ventricular function. The pulmonary artery pressure was measured to be 12 mm. A follow-up echocardiography was performed at 6 months of age, which showed consistent findings except for closure of the patent ductus arteriosus. Repeat echocardiography at 3 years of age revealed a main pulmonary artery pressure of 30 to 40 mmHg.
Chest Computed Tomography (Chest CT)
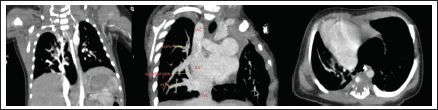
Chest CT with angiography was suggestive of scimitar syndrome (Figure 2). There was a hypoplastic right lung, mainly its upper lobe with right basal anomalous pulmonary venous return into the IVC and a slightly reduced size of right main pulmonary artery. There was no aortopulmonary collateral from abdominal aorta to the right lung.
Treatment
During the neonatal period, she required only oxygen via nasal cannula for 2 days to maintain a target saturation of more than 94%. The patient was hemodynamically stable all through the neonatal intensive care period and discharged at fifth day of life with multidisciplinary team follow-up appointments.
Outcome and Follow-up
Keeping in mind the natural course of neonatal scimitar as reported in the literature to have a high mortality and poor prognosis, we followed up our case to assess her neurodevelopmental status.
Following discharge from the neonatal intensive care unit, the patient has been under regular follow-up in the outpatient department. Her neurodevelopmental status was assessed by the treating physician using the age appropriate Ages and Stages Questionnaire (ASQ) at 18 months, 24 months, 36 months, and 48 months under the domains of gross motor, fine motor, communication, problem solving, and personal-social respectively. At 24 months of age, her ASQ score in the communication domain was found to be less than 2 standard deviation compared with the established cutoff points for that particular domain. Henceforth, she was subjected to a detailed hearing evaluation (brain stem-evoked response audiometry) and diagnosed to have mild-to-moderate sensorineural hearing loss. Currently, the child has hearing aids in both ears. Speech assessment done showed that child has speech delay but can identify the ling sounds. Her ASQ score assessed under gross motor, fine motor, problem solving, and personal-social were all within normal values for her age. Her length and head circumference were at 50th centile for her age expect her weight which was below third centile according to the World Health Organization growth chart. Currently, she is under regular follow-up with a pediatric cardiologist, Ear, Nose & Throat team, and speech therapist for continuation of care and further interventions.
Discussion
Infantile scimitar syndrome is usually severe and associated with complex congenital anomalies of the heart and lungs. 8 In the neonatal period, it presents with congestive cardiac failure, most commonly due to pulmonary hypertension and respiratory distress. The right lung is most frequently involved. Variable degrees of hypoplasia and malformations of the pulmonary arteries are found in the affected lung, as well as arterial supply from the aorta, which can also arise above or below the diaphragm. 5 Among the affected infants, 75% have associated cardiac malformations such as ASD, coarctation of the aorta, ventricular septal defect, and patent ductus arteriosus.9, 10 The diagnosis should be considered when there are signs of respiratory distress and/or heart failure present in association with radiological findings of cardiac dextroposition and haziness or suspicion of atelectasis of the right lung that does not improve. 11 The presence of “scimitar sign” may not always be seen in chest X-rays.
Rukban et al’s study was one of the largest reviews on infantile scimitar focused on the outcome of their study patients conducted over a period of 10.5 years. The study included 16 patients. The median age at presentation was 14 days with a median age at diagnosis of 55 days. A total of 81% of their study population had pulmonary hypertension, 43% had systemic collaterals which were treated by coil occlusion between the ages of 14 days and 2 years, and mortality was 18.8%. 6
Wang et al conducted a retrospective database analysis on 5 patients diagnosed over a period of 16 years with scimitar syndrome and had only 2 patients with infantile scimitar syndrome. The youngest age at diagnosis was 6 days old. 12 Their study concluded that infantile scimitar is a rare congenital anomaly of the heart and lungs that need a high degree of suspicion for early diagnosis and referral.
A similar retrospective analysis conducted by Najm et al on 32 patients with scimitar syndrome over a period of 20 years had only 6 children with infantile scimitar diagnosed in the first year of life. Their median age at diagnosis was 7 months with female preponderance. Their study was focused on the surgical follow-up of patients who underwent corrective surgery. Among the infantile group, they had 50% mortality. Pulmonary arterial hypertension with infantile-type scimitar syndrome has been recognized as a cause of severe symptoms and poor outcome. 7
Huddleston et al identified 23 patients with scimitar syndrome over a period of 25 years, and had 12 children with infantile scimitar with a mean age of 6 weeks (ranging from 2 days old to 4 months of age). 13 Similarly, Uthaman et al 14 looked into the surgical outcome of patients with infantile scimitar. In both studies, the authors focused on the clinical course, presence of cardiac and noncardiac anomalies, development of pulmonary arterial hypertension, and the related outcomes with surgical repair. In Huddleston et al, only 4 patients survived after surgical repair, but their intact survival status without NDD was not reported. 13
All the retrospective analyses published to date were focused only on related short-term outcomes, whereas they had not looked into the incidence of their study patient’s survival with or without NDD. Our case study was the only case report focused on the NDD of infantile scimitar syndrome that showed sensorineural hearing loss with normal motor and cognitive development. Contrary previous reviews, our neonate presented earlier at 8 h of life with desaturation, tachypnoea, and chest retractions. She was diagnosed to have scimitar syndrome within 24 h of life by transthoracic echocardiography, chest computed tomography, and angiography. The youngest age reported in the literature so far was 2 days old neonate. 6
The interesting fact with infantile scimitar is that high mortality and poor outcomes were seen in children with a high pulmonary artery pressure at diagnosis. However, our case did not have pulmonary arterial hypertension at the time of diagnosis. This could explain the child’s intact survival without NDD, although sensorineural hearing loss was present.
Current literature does not show any causal relationship or association between infantile scimitar and sensorineural hearing loss, although the presence of sensorineural hearing loss could be a coincidental finding in our case. The authors recommend that whole exome sequencing may be beneficial to identify the association of sensorineural hearing loss with infantile scimitar syndrome. However, other unusual presentations like congenital hydrocephalus, heart block, and imperforate anus associated with infantile scimitar have been reported in the literature.15, 16
Conclusion
This was the first case of infantile scimitar syndrome (congenital pulmonary venolobar syndrome) which was diagnosed within 24 h of age in a neonate and had a meticulous neurodevelopmental follow-up to assess the intact survival without NDD. The case was reported to encourage authors to report more cases of neonatal scimitar syndrome with and without associated complex congenital anomalies of the heart and lungs and to do neurodevelopmental follow-up of those cases to find their intact survival without NDD.
Endnotes
What the case study adds:
The triad of respiratory distress, right lung hypoplasia, and dextroposition of the heart should alert the clinician to think of scimitar syndrome in the neonatal period.
Recommended to report more cases of neonatal scimitar syndrome and to do neurodevelopmental follow-up to find intact survival without NDDs.
Future studies to focus on long-term outcome of neonatal scimitar.
Footnotes
Author Contributions
AA prepared the initial manuscript. JJ edited and wrote the final manuscript. SA and PS reviewed the manuscript. All authors approved the final manuscript.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed consent obtained from the parents.