Abstract
Coronary artery calcification (CAC) is a well-known entity, with a high incidence amounting to a third of the total coronary artery disease (CAD) patients. It is also associated with a high complication rate during percutaneous transluminal coronary angioplasty, such as stent non-trackability, stent non-apposition, and underexpansion. The recent technological advances have helped to perform percutaneous coronary intervention in the calcified coronaries with better results. The management of calcified lesion was mainly concentrated on interventional techniques, this article gives a comprehensive review of CAC pathophysiology, its morphology, various diagnostic modalities, newer diagnostic tools, upcoming medical therapies, and interventional techniques. Newer therapies which include vitamin K and myoinositol hexaphosphate, their role in pathogenesis of CAC, and its future role in preventing and treating CAC are covered in this article.
Introduction
The process of calcification of arteries has been known to mankind since a century and half. 1 Almost a third of coronary artery disease (CAD) patients found to have calcification, therefore with such high incidence it becomes an important factor while deciding its therapeutic management. Earlier thought to be inoperable lesions by interventional cardiologists, such patients were invariably referred for coronary artery bypass grafting procedure. Coronary artery calcification (CAC) was considered as an adversary of interventional cardiologist due to complications associated with percutaneous coronary intervention (PCI), such as non-trackability of stent, malapposition, and underexpansion of stent, or due to high rates of stent thrombosis and restenosis. The technological advances in last 2 decades have ensured safe and efficient optimization of CAC and have improved PCI outcomes.
The process of early atherosclerotic calcification similar to fatty streak formation begins in second decade of life. 2 This was followed by CAC, which is a process which leads to the build-up of calcium in the coronary arteries over a period of time.
Incidence
Multiple studies over the years have shown a wide range of CAC incidence ranging from 12% (C-SIRIUS) to 38.5% (COMPARE).3, 4 A pooled analysis of 12 such studies has shown incidence of 29%. Studies have shown 37.7% of all ST-segment elevation myocardial infarction (MI) patients and 26.7% of all non-ST-elevation acute coronary syndrome (ACS) patients have moderate to severe calcification of coronaries.5, 6
Prevalence of CAC is age, gender, and race dependent. South Indian men have age adjusted incidence of CAC of 11.1% per 100 person-years, similar to Caucasians and twice the incidence among Chinese (5.7%). 7 One of the major risk factors promoting CAC is age, >90% men and >67% of women develop CAC at 70 years of age. 8 The calcium-phosphate regulating mechanism affects CAC.
Risk Factors
CAC is divided in intimal and medial vascular calcification. Intimal calcification is influenced by advanced age, diabetes, hypertension, dyslipidemia, and smoking. Similarly, medial calcification is mainly influenced by chronic renal issues (low-glomerular filtration rate, hyperphosphatemia, abnormal parathyroid hormone, hemodialysis). 9
Prognostic Implication
Adverse Outcomes of Vascular Calcification. 11
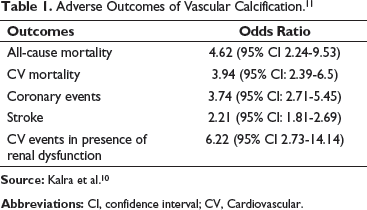
Source: Kalra et al. 10
Abbreviations: CI, confidence interval; CV, Cardiovascular.
Phenotypic Types of CAC
Phenotypically, CAC can be divided into eccentric and concentric lesions. Eccentric calcium is defined as calcium plaque covering <3 quadrants (<2700) of the vessel lumen circumference, whereas concentric calcium is cross-section lesion of >3 quadrants (>2700) of the vessel circumference. The balloon dilatation of such eccentric lesion leads to some luminal gain by stretching and disruption of noncalcified vessel wall; sometimes this might cause dissections at the shoulder of the calcium plaque. In concentric calcium, balloon dilatation causes fracture in thinner, weaker areas of calcium. The stent underexpansion, malapposed stent, and perforation in CAC plaque are problematic for which proper PCI optimization is absolute necessary.
Pathophysiology
Vascular calcification can be intimal or medial in origin. The endothelial lining of intimal layer undergoes series of intrinsic changes which eventually leads to atheromatous plaque formation that can cause plaque rupture and subsequent thromboembolic events. The medial layer consists of smooth-muscle cells (SMC) and elastic fibers that regulate arterial flow and pressure. Calcification of the media is thought to cause arterial stiffening, reduce compliance, and limit distensibility, which increases risk for MI and heart failure (HF). 11
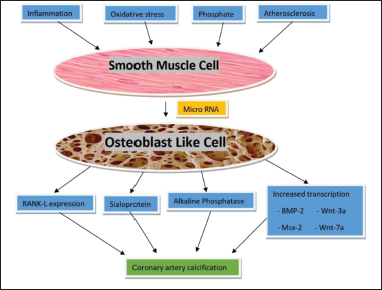
The differentiation of SMC to osteoblast-like cells (OLCs) is main crux behind intimal/medial CAC (regulated by microRNA). Causes for differentiation of SMC to OLC are inflammation, oxidative stress, inorganic phosphate, and atherosclerosis. These OLCs when stimulated by transcription factors like Msx2, Sox9, Runx2, and osterix lead to upregulation of differentiation of SMCs and increased production of bone, chondrocyte protein, and matrix vesicles, which are released into the interstitium of vascular tissue leading to CAC 12 (Figure 1).
The pathophysiology of coronary artery calcification (CAC); the basic pathology involves metamorphosis of smooth muscle cell (SMC) to osteoblast like cells (OIC). This metamorphosis is triggered by inflammation, oxidative stress, phosphates, and atherosclerosis. Intracellular processes inside OIC such as RANK-L expression, sialoprotein, alkaline phosphatase, and increased transcription factors are stimulated and this causes mineralization of vessel intima and thus leads to CAC.
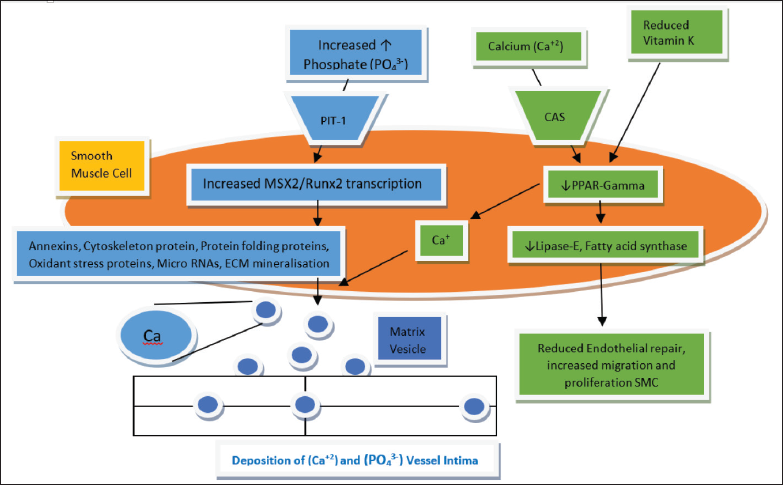
Another mechanism by which CAC occurs involves vitamin K and its effect on endothelial repair. Vitamin K can be divided into K1 (phylloquinone), K2 (menaquinone), K3 (menadione), K4 (menadione esters), and K5. Major source of Vitamin K1 includes green-leafy vegetables like kale, spinach, turnip, lettuce, broccoli, cabbage, cauliflower, and Brussels sprouts. Major sources of vitamin K2 are milk products, cheese, butter, and meat. 13 Vitamin K2 (MK-4, MK-7) has been studied extensively. The basic physiology involves conversion of hydroxyquinone to epoxide form of vitamin K, thus giving us γ-carboxylated protein (carboxylation of glutamic acid residue). This γ-carboxylated protein is the active form which has significant role on the blood clotting mechanism.14, 15 As shown in Figure 2, some animal studies have shown vitamin K deficiency leading to reduced γ-peroxisome proliferator-activated receptor (PPAR) (nuclear hormone receptor), thus reducing endothelial repair, inhibiting migration, and proliferation. 16 Rotterdam study clearly showed us that dietary intake of menaquinone is associated with reduced risk of calcific CAD. 17
The pathophysiology of coronary artery calcification (CAC); Various intracellular mechanism associated with causing mineralization of vessel intima. Inorganic phosphate after entering SMC stimulates transcription of MSX2 and Runx2 genes, which in turn leads to collagen and cytoskeleton protein production. This in turn will release calcium crystal vesicle formation which in turn is released in intima and is deposited causing CAC. Similarly, deficiency of vitamin K leads to reduced PPAR-gamma which in turn reduces endothelial repair and increased intracellular calcium.
Typical patterns (by radiography) of calcified coronaries can be divided into speckled (found in erosive plaque and thin-capped fibroatheroma [TCFA]), fragmented (found in ruptured plaque), and diffuse (found in healed rupture and fibrocalcific plaque). Microscopically speaking, the calcification can be divided into microcalcification, calcific nodules, and calcium sheets. The microcalcification can disrupt TCFA leading to thrombosis; similarly calcific nodules lead to plaque rupture. Diffuse CAC is associated with worse cardiovascular outcome like higher incidence of ACS and HF. 18
Pathophysiology behind chronic kidney disease (CKD) involves secondary hyperparathyroidism and overactivation of renin-angiotensin-aldosterone mechanism which promotes medial-artery calcification. 19 The advanced glycated end-products promote microvascular mineralization. 20
Diagnosis
Noninvasive Coronary Imaging
The extent of CAC is strongly associated with severity of atherosclerosis and rate of future cardiac events. 21 With the advent of digital radiography, there is significant progress made in thoracic imaging. Especially dual-energy subtraction (DES) imaging on video fluoroscopy is very useful, as calcium selectively attenuates lower-energy photons in an x-ray beam, as a result we get 2 sets of images. A soft tissue selective image and a bone selective image (where bones and ribs are eliminated). This technique described in detail by Gilkeson et al 22 provide us with detailed evaluation of CAD. 22
Coronary Artery Calcium Score and Associated Relative Risk of Major Adverse Cardiovascular Events (MACE).
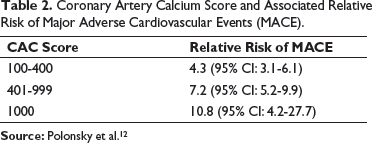
Source: Polonsky et al. 12
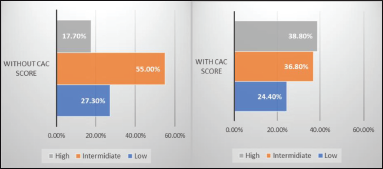
The graph “a” represents sum total of all cases being divided in high, intermediate, and low-risk group based on angiogram results. As it is very clear, the intermediate group percentage is high, thus confusing the best treatment modality. As graph “b” shows when we use CAC score along with angiogram report, the intermediate risk group reduces in number and percentage, thus helping in choosing best treatment modality.
Cardiac magnetic resonance angiography allows for a noninvasive assessment of the coronary anatomy without exposing patients to radiation, with excellent soft tissue resolution, and is superior to contrast-enhanced coronary CT angiography for the evaluation of luminal narrowing in heavily calcified coronary segments. 28 Due to relative absence of protons (H+1 atoms) in calcified vessel, the visualization in MRI sequences was difficult, partly because calcium is dimagnetic. With better technology now (prolonged acquisition time, bright, and black blood techniques), MRI can detect ACA with high degree of sensitivity and specificity. MRI studies show that it can underestimate amount of calcification; it is possible that microcalcification in CAC may be missed. 29
Intravascular MRI is partial invasive method which uses an intravascular MR detector coil to enhance characterization of the fine structure of deep small arteries, thus enhancing image quality. Initial studies have shown detection of accurate plaque composition and size. Some of the negative points about this method include the bulky detector coil and MR machinery in cathlab. 30
18 F-sodium fluoride ( 18 F-NaF) tracer is used to detect bone formation and calcium deposition in tissue. The process of atheroma/vascular calcification is similar to bone formation. Histopathologically, vessel has presence of OLC with deposition of hydroxyapatite. 31 This technique of hybrid scans using tracer with positron-emission tomography (PET) is employed along with CT/MRI scan in detection of CAC. 18 F-NaF tracer uptake happens where osteoblastic/osteoclastic activity is high, therefore microcalcifications are detected very well, whereas heavily calcified lesions may not show any 18 F-NaF uptake. Therefore, a combination of PET-CT scan imaging will reveal a calcific lesion and lesions with risk of plaque rupture in coronary arteries. In a study, among all the 93% of MI patients, the 18 F-NaF uptake was significantly higher in culprit artery (1.66 [interquartile range: 1.4-2.25]) vs nonculprit artery (1.24 [1.06-1.38]). Similarly, the study showed that it is possible to differentiate between different plaque composition (fibrous tissue, fibrofatty, necrotic core, dense calcium, microcalcium). In spite of some technical difficulties like myocardial uptake of 18 F-NaF, PET-CT can play an important role to detect vulnerable plaque in stable/unstable angina in vivo. 32 The PRE 18 FFIR trial revealed that hybrid scans PET-CT and PET-MR using 18 F-NaF tracer uptake fared equally in nonstented coronaries, whereas in stented PET-MR is limited by artifact in stented coronaries. 33 Other tracers like 18 F-fluorodeoxyglucose ( 18 F-FDG) 33 and 68 Ga-DOTATATE, 34 can localize to culprit coronary plaques.
In comparison, the radiation dose exposure for CT coronary angio is 3-5 mSv, whereas for 18 F-NaF PET-MR scan is 6.6 mSv and for 18 F-FDG scan is 7.8 mSv, which is higher than PET-CT scan where the average exposed dose is 13.7 mSv. 35
MR spectroscopy is mainly used for molecular imaging of the atheroma. There is lot of interest in this imaging as newer methods are being tested to know the plaque composition. Till now, calcified coronary detection is yet to be achieved. 36
Some selective studies involving use of intravascular thermography to detect high-risk vulnerable plaque have been partially successful. Here, the mechanism involved is to detect subtle changes in temperature of the plaque, which is the result of arterial inflammation. 37
Invasive Coronary Imaging
Coronary angiogram is an invasive method to determine CAC. It has low-moderate sensitivity with high specificity. It helps to determine whether further testing like intravascular ultrasound (IVUS) or optical coherence tomography (OCT) is required. 38 Radio-opacities on cardiac fluoroscopy (still image) suggest severe CAC; similarly, if the opacities are visible only during cardiac motion, it suggests intermediate CAC. 39
Most accurate method to determine the presence and extent of CAC is IVUS. With sensitivity and specificity reaching as high as 90% to 100% and 99% to 100%, respectively. 40 Conventional IVUS uses 20 to 40 MHz range ultrasound waves to detect echogenic structures, whereas newer systems use multifrequency IVUS imaging involving 80 to 150 MHz along with conventional frequencies. 41 In IVUS, the CAC appears hyperechogenic mass with acoustic shadow behind. Calcium has a characteristic acoustic signature of being echogenic/brighter than the reference adventitia, with shadowing of deeper arterial structures. 42 A large study (PROSPECT trial) involving 660 patients, IVUS data revealed that significantly high plaque burden has higher risk of MACE in nonculprit vessel (14.1%), arising from both calcified/nonclacified plaque (66% vs 56%). 43 An interesting study by van der Giessen et al 23 clearly shows that 53% of the calcifications seen on the IVUS images cannot be detected on contrast-enhanced 64-slice multislice CT angiography images because of their size. The IVUS minimum lumen area (MLA) is correlated with ischemia with cut-offs between 2.1 and 4.4 mm 2 in Western studies (median: 3.0 mm 2 ). Overall, IVUS trials have shown high negative predictive value (72%-96%) and a low positive predictive value (39%-73%), indicating that MLA is more reliable than IVUS in justifying an intervention. 45 .
OCT in coronary imaging is considered as optical analog of IVUS. It uses polarization of light, therefore has 10× higher resolution than IVUS (IVUS: 100-150 µm, OCT: 10-20 µm axial resolution). The technique involves replacement of column of blood in coronary artery by contrast which is injected during the process. In OCT, the CAC appears as well delineated, low-signal region with sharp borders. 46 Pre-intervention OCT imaging delineates plaque constituents and provides accurate measurements of the MLA, lesion length, and vessel diameters, as well as visualization of the projected stent landing zones. These parameters can be used for procedural planning, including proper lesion preparation and stent sizing. Knowledge of plaque characteristics can be used to select a plaque modification strategy prior to stent implantation and to minimize stent edge dissection at the stent landing zone. 47 Both IVUS and OCT help us to differentiate CAC as concentric/eccentric lesions. In spite of very high sensitivity of OCT when compared to IVUS, for detecting stent malapposition, this has not improved predictive value of the diagnostic tool for predicting early/late restenosis 48 (Figure 4).
Images A, B, and C show a patient having calcified coronary pre-ROTA, post-ROTA, and post-stenting results. Similarly, images E, F, and G show concentric calcium deposition in vessel pre-ROTA, post-ROTA, and post-stenting results.

As CAC obstruct the detailed evaluation of a plaque by IVUS, newer methods in combination with IVUS such as near infrared spectroscopy (NIRS) imaging just before PCI helps in diagnosing necrotic-core and lipid-rich plaques, that is, lipid content in CAC can be detected easily. This also reduces periprocedural MI.49, 50
Medical Treatment
Medical management of the CAC is still in its infancy and includes use of statins, vitamin K2, SNF472, and some drugs used in conditions like CKD.
The statins forms the corner stone of the management of the CAD. It acts by reducing the low-density lipoprotein levels and thus slows down/reverses the atheroma formation and reduces CAC score. 51 But certain long-term studies such as Henein et al 52 have shown that statins can lead to an increase in CAC score. Whether this is paradoxical or statins promote CAC, stabilizing plaque is yet to be proven.
As mentioned above, menaquinone reduces CAC score as shown in Rotterdam study, 17 and reinforced with another study showing association of use of warfarin and increased number of patients with CAC score >400 in a cohort of low-risk AF patients. 53 In 1 double-blinded randomized clinical trial, where supplementation of menaquinone (180 mcg of MK-7) in 244 healthy post-menopausal women for a period of 3 years improved their arterial stiffness. 54 In CKD patients with vitamin K deficiency, it was noted that there is increased calcification of vascular SMC and demineralization of bone when calcium is supplemented. Whereas in vitamin K sufficient condition, the inverse in true. This vascular-bone axis is described in detail in many studies. 55
Schooling et al 56 published a study with the help of Mendelian randomization in Caucasians, where Vitamin K1 (phylloquinone) intake is associated with high risk of ischemic heart disease. In conclusion, vitamin K2 has properties of reducing the burden of CAC, whereas vitamin K1 increases risk ischemic heart disease. There is some evidence as to in vivo conversion of vitamin K1 to vitamin K2 in testes, pancreas, and arterial wall. 14
There are some experimental drugs like myo-inositol hexaphosphate (SNF472), which have shown to reduce development of cardiovascular calcification by up to 80% in preclinical study. 57 Further, randomized trials like CaLIPSo trial will further reveal effectiveness of SNF472 moelcule. 58
The CKD is a special condition where the vascular calcification is the cause for arterial stiffness, which in turn is caused by hyperparathyroidism, serum calcium-phosphate product (CPP), hypovitaminosis-D, and hypovitaminosis-K. 59 Therefore, vitamin D analogs, phosphate binders (to reduce hyperphosphatemia), and calcimimetics (to reduce PTH) are used in CKD condition to reduce CPP and thus reducing vascular calcification. The ADVANCE trial failed to demonstrate the effectiveness of cinacalcet (calcimimetic) in calcification in hemodialysis patient. 60 Similarly, noncalcium phosphate binders, like Sevelamer, have shown slow progression in cardiovascular calcification. These calcium-phosphate binders are associated with hypercalcemia and therefore might increase the risk of vascular caclification. 61
Interventional Treatment
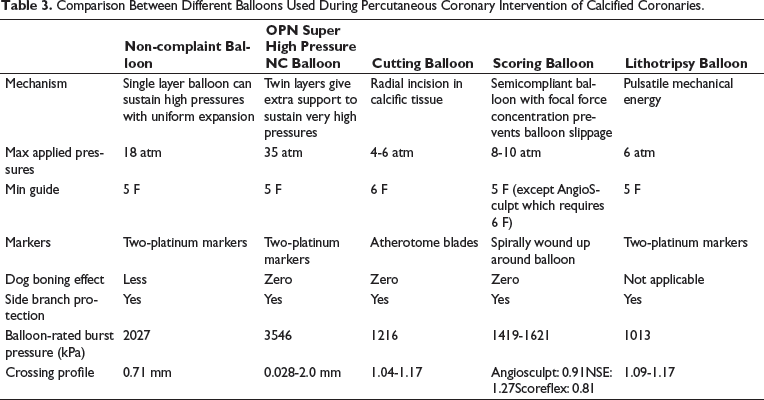
Comparison Between Different Balloons Used During Percutaneous Coronary Intervention of Calcified Coronaries.
Noncompliant Balloon
Unlike semicompliant balloon, NCB are transparent, 0% to 10% compliance and can tolerate high-inflation pressures. They are ultra high-strength, thin-walled balloons, generally fabricated from PET and used for coronary/peripheral angioplasty, stent delivery, and CAC dilatation procedure. These high-inflation pressures allow uniform balloon expansion, which can be applied on focal segment too. This avoids dog-bone deformation with exertion of high pressures at the edges, thus reducing chances of dissections and perforations. This is considered an effective and safe strategy in mild-moderate CAC. 62
A variant of NCB is OPN, which is super high-pressure percutaneous transluminal coronary angioplasty balloon which has double-layer balloon construct which helps in achieving zero dog-bone effect. 63
Cutting Balloon
During a regular balloon dilatation of calcified lesion, there is risk of uncontrolled vessel stretch and vessel injury, leading to unrestrained atherosclerotic plaque disruption. This is avoided by a cutting balloon as it delivers a controlled fault line during dilatation, ensuring orderly crack propagation. Balloon inflation is at a much lower inflation pressure (4-8 atmospheres). Cutting balloon (Boston Scientific Inc, Marlborough, MA, USA) features 4 atherotomes (microsurgical blades), which are 3 to 5 times sharper than conventional surgical blades. The outer surface of the NCB has longitudinally fixed blades which expand radially and provide longitudinal incisions in the plaque-relieving hoop stress. 64 The Cutting Balloon Global Randomized Trial was the largest randomized trial (n = 1238), comparing cutting balloon atherectomy (CBA) with plain old balloon angioplasty (POBA) for the prevention of restenosis in de novo lesions. Procedural success was similar between groups. CBA had higher rate of perforation (0.8% vs 0%, P = .03). The primary endpoints of binary restenosis at the end of 6 months were similar between CBA and POBA (31% vs 30%, P = .75). 65 An IVUS-based study indicated that CBA achieves larger luminal gain than POBA in calcified lesions. 66
Scoring Balloon
The higher rate of perforation and difficulty with delivery of cutting balloon led to the development of alternative balloon-based atherectomy devices, such as scoring balloons. Scoring balloons are semicompliant nylon balloons encircled by external spiraling scoring elements. These scoring elements allow focal concentration of the force during inflation and decrease balloon slippage. Scoring balloons have similar indications to cutting balloons, but scoring balloons are more flexible, have a better profile, and can achieve a full expansion with a low inflation pressure, with consequently less trauma to vessel walls and a minor risk of coronary dissections. 67
A study of 184 lesions treated with POBA vs AngioSculpt for lesion preparation prior to bioresorbable vascular scaffold implantation showed despite using AngioSculpt in a higher proportion of type B2/C, restenotic, and calcified lesions, the scoring balloon group demonstrated better procedural IVUS outcomes with regard to both scaffold expansion and eccentricity. The 1-year target lesion revascularization rate was similar between groups (conventional balloon 6% vs AngioSculpt 7%; P = .87). 68
In the PREPARE Severely CALCified Coronary Lesions Trial (PREPARECALC) study, 200 patients were randomized 1:1 to PCI treatment with either RA or modified balloons (both cutting and scoring balloons). Both strategies of RA and myocardial band (MB) are associated with excellent clinical outcome at 9 months, but high crossover from MB group to RA was reported in the study (16% of lesions were untreatable with modified balloons). 69
Intravascular Lithotripsy
Periprocedural complications of atherectomy procedures include slow-flow, periprocedural MI, complex dissection, and perforation. 70 IVL is the latest technology where multiple lithotripsy emitters are mounted on a conventional catheter platform which delivers focussed pulsatile sonic pressure waves to circumferentially modify vascular calcium. In the Disrupt CAD I study (Disrupt CAD), it was demonstrated for the first time the feasibility of IVL to modify vascular compliance in coronary calcific plaque. 71 In the ORBIT II study treated with OA, clinical success was achieved in 88.9% of patients with in-hospital MACE being 9.8%. Whereas IVL had clinical success rate of 94.2% and in-hospital MACE rate of 5.8% in Disrupt CAD II.72, 73 Therefore, IVL can be safely performed with high degree of procedural success with minimal complications and resulted in substantial calcific plaque fracture in majority of lesions.
Balloon for Light Therapy
Laser therapy can be delivered with polyethylene-terephthalate (PET) balloons. These balloons are well suited for Laser balloon angioplasty as they are optically clear and transmit light over a broad spectrum. The laser therapy that includes simultaneous application of heat and pressure on coronary arteries will reduce arterial recoil, remodel thrombus into a nonobstructive film, eliminate vasospasm, and may seal dissections induced during initial conventional PCI. As the balloon is transparent, the light emitting devices mounted inside emit light through the wall of the balloon. Not many large studies have been done, 1 small study showed high rate of restenosis of 60%, 2 to 6 months after procedure. 74 Therefore, the use of laser balloon angioplasty is limited.
Atherectomy
The concept of atherectomy includes debulking and modifying atherosclerotic plaques. It was introduced more than 30 decades ago as a means of physical removal of plaque. There are 4 types of atherectomy, which include RA, OA, directional atherectomy, and laser atherectomy.
Rotational Atherectomy
In initial stages after introducing RA in 1988, 75 the interest and enthusiasm dampened due to high rates of stent restenosis.76, 77 Later on during post-DES era, multiple studies revealed that introduction of drug eluting stent reduced the restenosis rates to minimum. The prevalence of RA use in Europe and USA varies from 1% to 3% of all PCI. 78 The mechanism of RA involves drilling process using a hard burr. The rotating burr will specifically ablate hardened calcific atheroma, but spares elastic vascular tissue. During the drilling process, it generates a lot of microparticles/plaque debris (sized 5-10 µm) that flows distally in the coronary artery leading to vascular plugging, slow flow, or no-flow and thus may increase myocardial-specific enzymes. 79 Both IVUS and OCT analysis after RA have shown smoothening and enlargement of lumen with cracks in the calcific plaque.80-82
The PREPARE-CALC done in 2018, with 200 patients randomized to treatment with either RA or cutting or scoring balloons. In that study, a greater success rate was achieved with RA than with modified balloons (98% vs 81%, respectively). 69
The Rotablator System (Boston Scientific, Watertown, MA, USA) is made up of 3 components: a burr (microscopic diamond crystals coated elliptic burr), an advancer (that transmits rotational speed to the burr), and a control console (foot pedal/connecting handle in recent models). The nickel-plated burr comes with different sizes ranging from 1.25 to 2.50 mm diameter for transfemoral route; and 1.25, 1.50, or 1.75 mm burr for transradial approach. 83 An ultrathin (0.009 inch) steerable dedicated guidewire (RotaWire) of length 330 mm is used to cross the calcified lesion. These dedicated wires are less torque responsive and more steerable; furthermore, a regular 0.014-inch guidewire can be used to cross the stenosis and the RotaWire can then be inserted through a microcatheter. Once burr is placed in proximal lesion, rotablator is started at speeds (135,000-180,000 rpm), and with drilling action the plaque optimization is carried out. The RA has become gold standard for optimization of heavily calcified lesions before stent deployment.
Orbital Atherectomy
Comparison Between Rotational and Orbital Atherectomy.
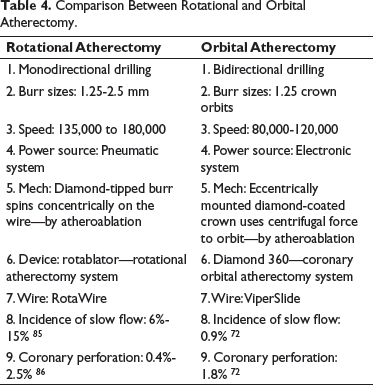
OA modified calcified plaques more than RA, with consequently better stent apposition and expansion. 81 A mean ablation area of 0.55 ± 0.41 mm 2 and an ablation volume of 2.68 ± 2.80 mm 3 were measured with OCT in a case series of 18 patients, with 18% of intimal dissections reported. 87 The OA system in treating de novo calcified coronary lesions (ORBIT I) study was the first-in-human trial to evaluate the safety and performance of OA in 50 patients at 2 Indian centers, showing a procedural success rate of 94% and a MACE rate of 8% at 30 days. The ORBIT II study is a nonrandomized trial, enrolling 443 patients with severe calcified lesion in 49 US hospitals. ORBIT II showed high procedural success (98.6% of patients with <50% residual stenosis) with low periprocedural complications (slow flow <1%, coronary dissections 5.9%) and good outcomes, like 4.4% cardiac deaths at 2 years and 8.1% target lesion revascularization at 2 years. 72
Excimer Laser Coronary Atherectomy
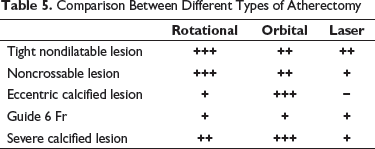
Comparison Between Different Types of Atherectomy
Major Learning Points
Calcified lesions in coronaries can be divided into mild, moderate, and severe.
Calcified lesions can lead to many issues like incomplete dilatation, high dissection rates, incomplete stent expansion, stent malapposition, and high rates of restenosis.
Severe calcified coronaries are associated with high rate of MACE.
Mild to moderate calcified coronaries can be dealt with high pressure inflation with short NC balloon, cutting flextome balloon, or AngioSculpt balloon.
Severe calcified coronaries are ideally managed with RA and OA.
Smaller vessels, bifurcation vessels, ostial side braches, fibrotic lesions, and in-stent restenosis lesions are ideal for use of cutting balloon/Flextome for better results.
Rotablator or OA should have burr:artery ratio of 0.4 to 0.6, advancement of burr should be slow, maintain <5000 rpm of baseline rpm, each ablation time lasting 20 s with intermittent pull back should be performed for better coronary perfusion.
Limitations of rotablation includes slow flow/no-flow, perforation, CK-MB release, wire bias, platelet activation with aggregation, debris emboliam, microcavitation, neurohumeral reflex, and dissections
Mild calcified lesions with nonobstructive coronary lesions can be started on medical management such as vitamin K2 supplements.
Vitamin D analogs, phosphate binders (to reduce hyperphosphatemia), and calcimimetics (to reduce PTH) can be used in CKD condition to reduce CPP and thus reducing coronary calcification.
Conclusion
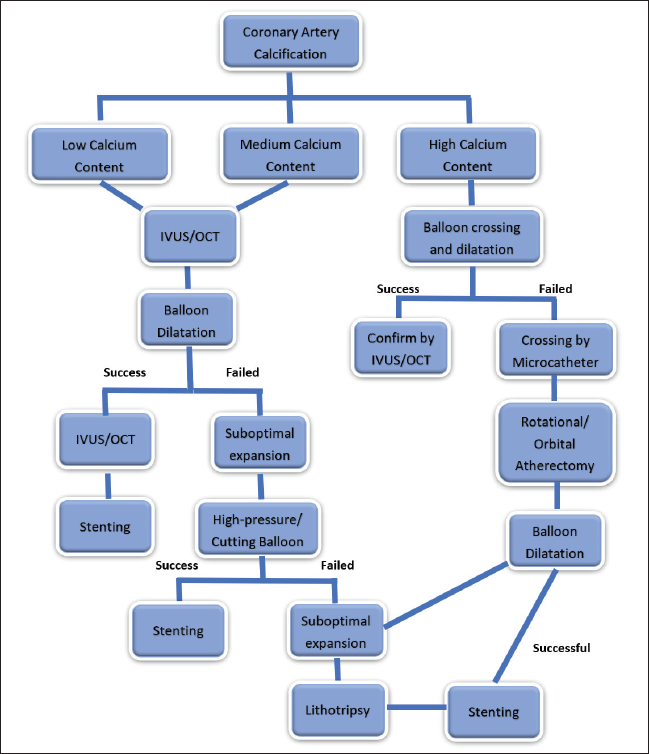
The calcification of coronaries possess significant challenges to the PCI operator while performing intervention. Therefore, it requires increased resources, longer training duration, and managing higher complication rates while performing coronary interventions on calcified coronaries. The medical management is still in the rudimentary state and requires lot of research and bigger trials to bring about any perceptible changes in management protocols for calcified coronaries (Figure 5).
The Algorithm for Management of Calcified Coronaries.