
Abstract
Tuberous sclerosis complex is an autosomal dominant condition with variable penetrance. It is characterized by tuberose deposits in various organ systems. Although clinical features predominate neurocutaneous manifestations, cardiac, kidney, and lung involvement are common. Cardiac involvement is marked by the presence of multiple rhabdomyomas and in some cases arrhythmias. In the absence of symptoms, rhabdomyomas require no specific treatment. However, cardiac arrhythmias are unpredictable and may be the cause of sudden cardiac death in some cases. Although treatment is mainly symptomatic, drugs like rapamycin have shown promise in the regression of astrocytomas and angiofibromas. Here, we are reporting two cases of tuberous sclerosis of which one succumbed to arrhythmias and the other to possible sudden cardiac death.
Introduction
Tuberous sclerosis was initially described by Von Recklinghausen in 1862. However Bournville is credited with having first characterized the disease in 1880, coining the name ‘tuberous sclerosis’ also called ‘tuberous sclerosis complex (TSC)’. TSC syndrome is a disorder of cellular differentiation and proliferation and has been referred to in the literature as Bourneville disease, Pringle disease, and Epiloia.1, 2 Tuberous sclerosis has an incidence of 1 in 6,000 to 12,000 live births. It is an autosomal dominant condition of varying penetrance and characterized by tuberose deposits in the brain but also in the heart, kidneys, eyes, and lungs, including various cutaneous manifestations. 3 The associated neurological problems of epilepsy, mental retardation, and occasional motor deficit are caused by the presence of tubers and other defects in cerebral development. The tubers become calcified and are detectable on computed tomography scanning of the head.
To aid the diagnosis of this highly variable disorder, a set of major and minor criteria have been proposed. A definitive diagnosis of TSC requires 2 major features or 1 major and 2 minor features and a probable diagnosis of TSC requires 1 major and 1 minor feature.4, 5 Cardiac manifestations of the disease include multiple rhabdomyomas with onset during fetal life, which if large enough may cause obstructive features or arrhythmias causing sudden cardiac death.6, 7 Multiple Rhabdomyomas could be the cause for intrauterine fetal demise, along with various cutaneous manifestations that can be associated with TSC. Hypomelanotic macules “ash leaf” or Fitzpatrick patches are ash leaf-shaped or polygonal white spots that are seen enhanced by a Wood lamp. These are the earliest cutaneous lesions and usually present at birth or infancy in 97.2% of TSC patients and forms a major criterion for diagnosis. 8 Besides the neurological and cutaneous manifestations, detection of cardiac rhabdomyomas by echocardiography in an infant is an important clue to the diagnosis of TSC.
We are reporting here 2 cases of TSC presenting in infancy with multiple rhabdomyoma along with neurocutaneous manifestations who succumbed to sudden cardiac death within a few months of diagnosis.
Presentation
Case 1
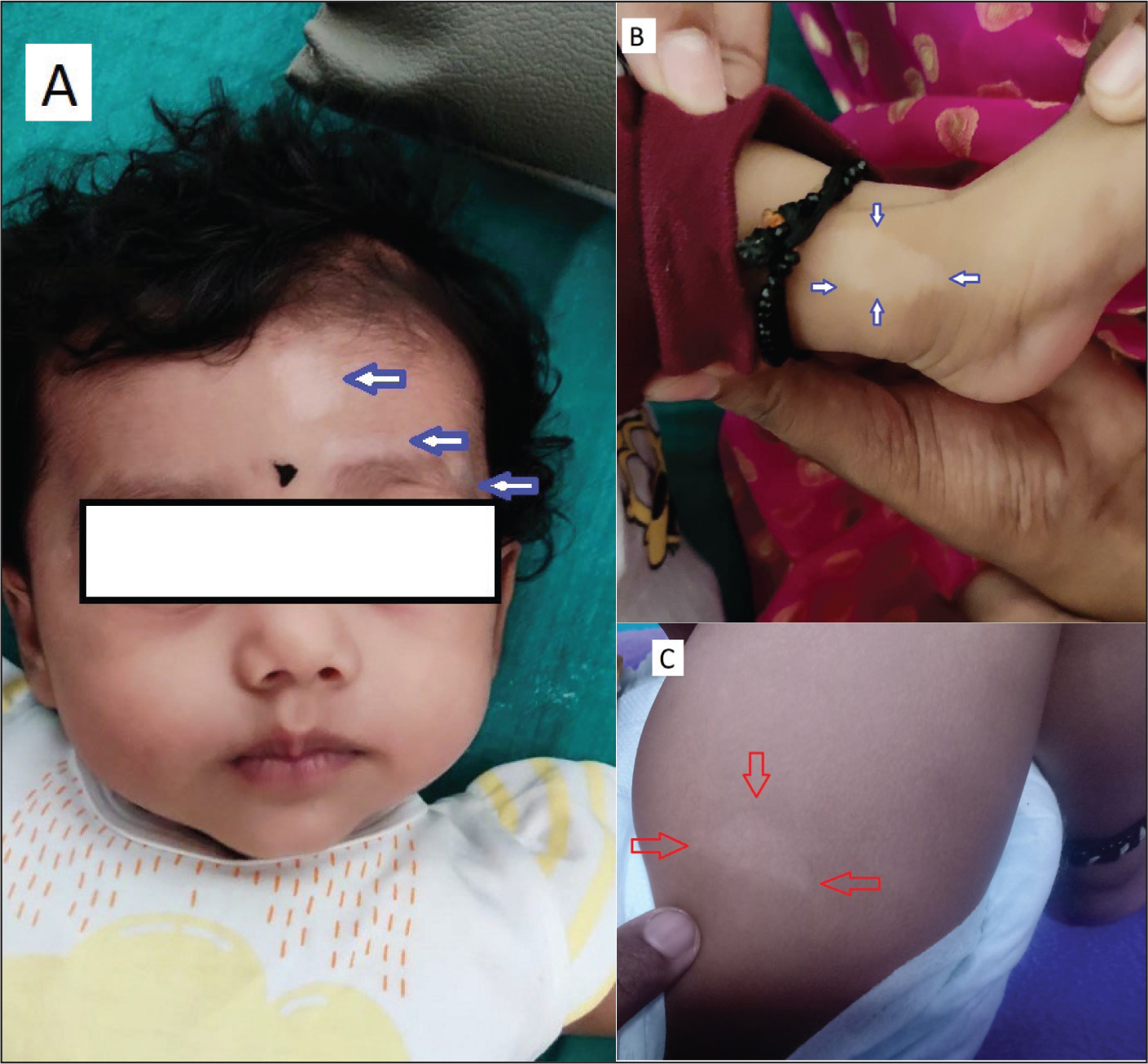
A 4-months old female child was brought to the emergency department by her parents with a history of recurring episodes of convulsions for 1 month and increasing frequency since morning on the day of presentation. On physical examination, the child had normal developmental milestones for the age with normal vital parameters. The child had multiple hypomelanotic macules over the face, hands, and legs (Figure 1A-C). Systemic examination was unremarkable.
Routine investigations revealed normal renal, liver, thyroid function tests, complete blood count, and serum electrolytes. Chest x-ray and electrocardiogram (ECG) were within normal limits. An ultrasonogram of the abdomen to rule out renal cysts was normal, the ophthalmic evaluation revealed right retinal astrocytic hamartoma in the superotemporal quadrant.
Serum calcium and magnesium were 10.9 and 2.3 mg/dL, respectively. Electroencephalogram was abnormal and showed high amplitude theta to delta activity, mixed with beta activity. There were recurrent bursts of sharp and spike-wave discharge seen predominantly on both centrotemporal regions and intermittently becoming generalized suggestive of focal seizures with secondary generalization.
Magnetic resonance imaging of the brain showed focal areas of cortical thickening with altered signal intensity noted in bilateral frontal, parietotemporal, and left occipital areas. Few subcentimeters, subependymal nodules were noted in the body and atria of bilateral lateral ventricles, the largest measuring 6 × 3 mm in the frontal horn of the left lateral ventricle. These cortical tubers and subependymal nodules were showing imaging evidence of definite TSC, shown in Figure 2A-D.
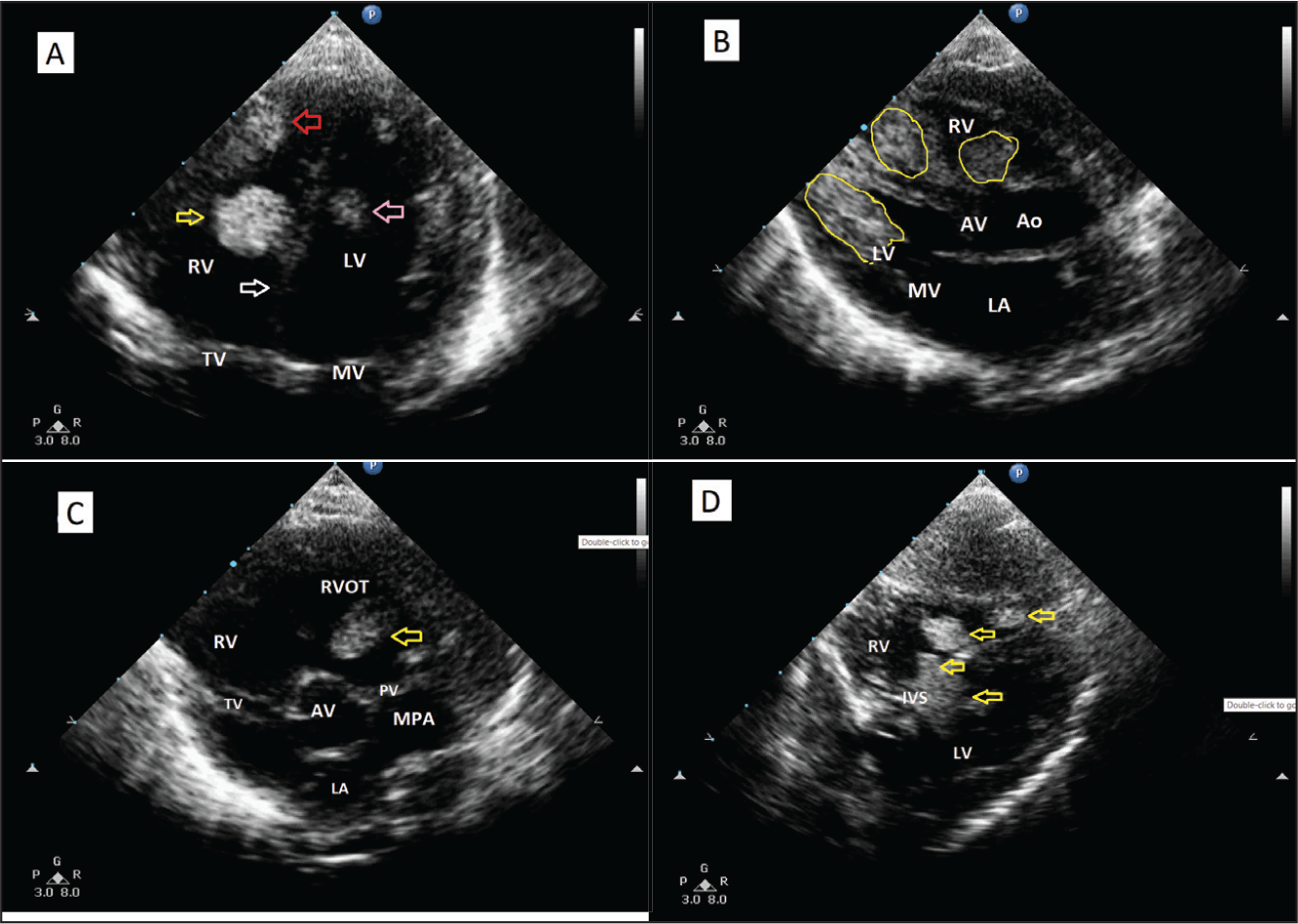
Two-dimensional echocardiography (2D ECHO) showed multiple rhabdomyoma arising from both the ventricles and attached to both interventricular septum (IVS) and free wall of both right ventricle (RV) and left ventricle (LV) as shown in Figure 3A-D and the Supplementary ECHO Video Clips of Case 1.
With four major criteria (hypomelanotic patches, retinal astrocytic hamartoma, cortical tubers with subependymal nodules, and multiple cardiac rhabdomyomas), the child met the criteria for the diagnosis of tuberous sclerosis.
Case 2
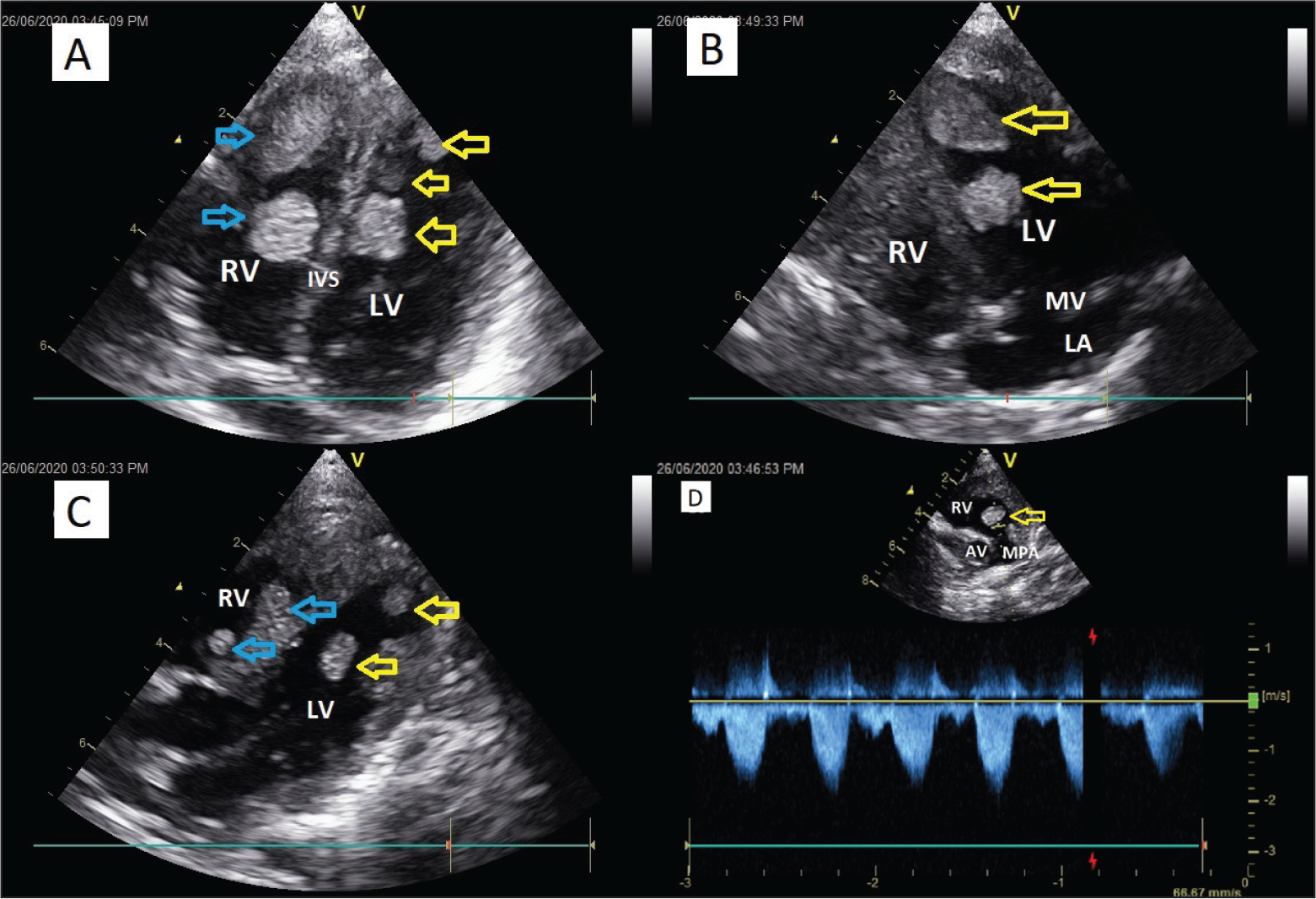
A 6-months old female child with recurrent episodes of seizures was evaluated and diagnosed to be having TSC based on major and minor criteria elsewhere (had 3 major criteria, hypomelanotic patches, cortical tubers, multiple cardiac rhabdomyomas, and 1 minor criterion, multiple intraoral fibromas), was referred for a 2D ECHO and cardiac evaluation. 2D ECHO revealed multiple rhabdomyoma in both RV and LV, and the right ventricular outflow tract (RVOT). As the child did not have any features of outflow obstruction or congestive heart failure, she was managed symptomatically. However, despite meticulous treatment for seizures, the child succumbed to a possible sudden cardiac death or sudden unexpected death in epilepsy 3 months later while in sleep. The ECHO images and video clips are shown in Figure 4A-D and Supplementary ECHO Video Clips of Case 2.
Management
Given the age of presentation, central nervous system symptoms and cutaneous markers, fulfilling the major and or minor criteria, both the described cases were diagnosed as TSC and managed symptomatically. Both children were treated with sodium valproate dose adjusted to body weight, and the seizures were controlled. However, a few months later Case 1 had a documented refractory ventricular tachycardia/ventricular fibrillation (VT/VF) and was treated in another center for the same, and succumbed to the arrhythmia. One of the ECGs (monitor strip) is shown in Figure 5, which was recorded just after defibrillation for sustained VT/VF. However, this reversion to sinus rhythm was transient, and the child succumbed to refractory VF despite appropriate therapy. The second child was found dead in sleep by parents and the exact cause for death could not be ascertained.


Discussion
Diagnosis of tuberous sclerosis is usually clinical, and further genetic testing looking for TSC1 and TSC2 gene mutations is confirmatory. In 2012, the International Tuberous Sclerosis Consensus Conference reviewed the prevalence and specificity of TSC-associated clinical manifestations and updated the TSC diagnostic criteria from 1998. The new clinical and genetic diagnostic criteria of 2012 are summarized as follows.
Definite Diagnosis: A definite diagnosis of tuberous sclerosis will be made when an individual has either 2 major features or 1 major feature with 2 minor features. A combination of the two major clinical features lymphangioleiomyomatosis and angiomyolipomas without other features does not meet the criteria for a definite diagnosis. Possible Diagnosis: A possible diagnosis of tuberous sclerosis will be made when an individual has either 1 major feature, or 1 major and 1 minor feature, or more than 2 minor features.
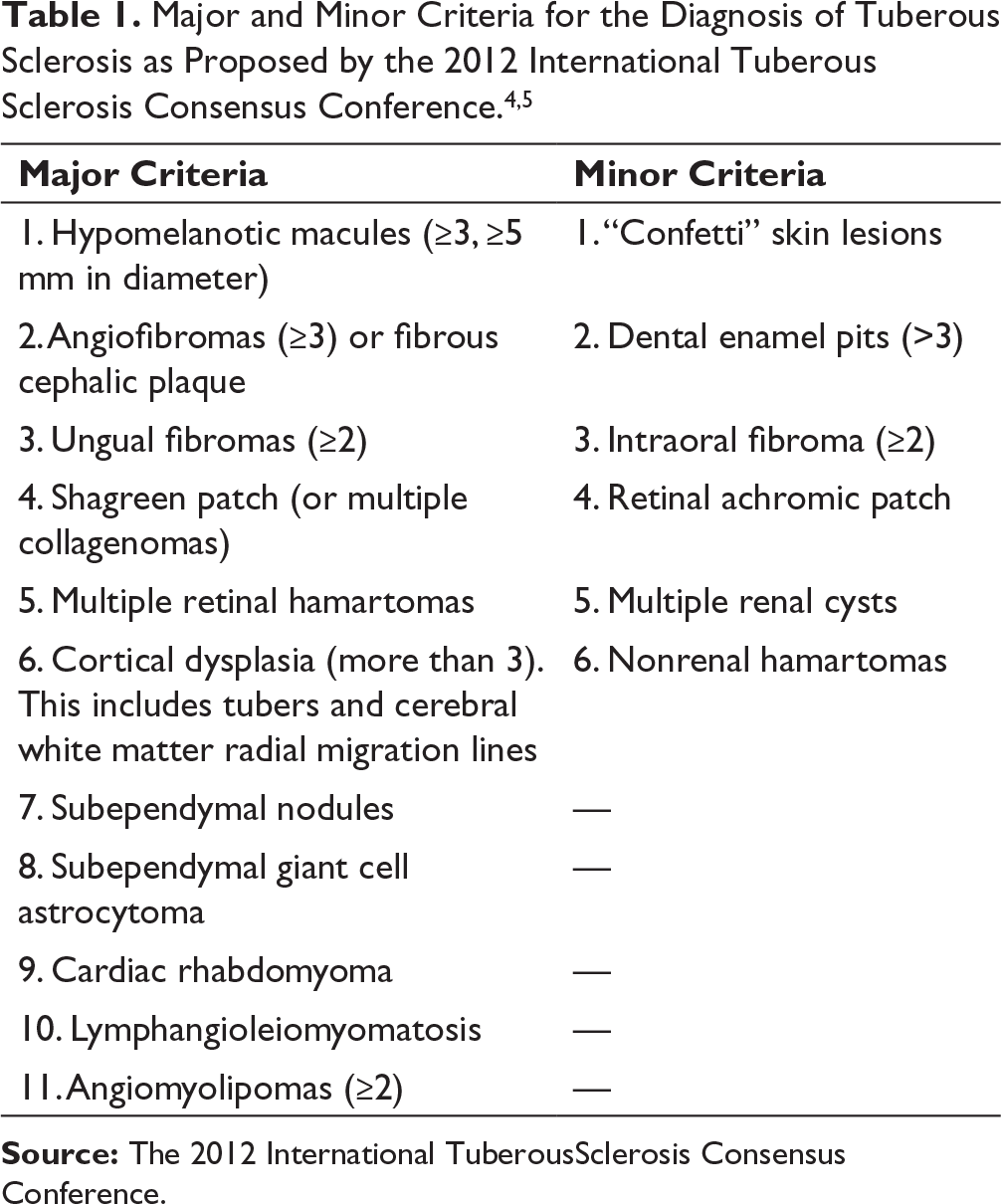
Source: The 2012 International TuberousSclerosis Consensus Conference.
Either a TSC1 or TSC2 pathogenic mutation is sufficient to make a definite diagnosis of TSC.
A pathogenic mutation is defined as a sequence variant that prevents TSC1 or TSC2 protein production.
Additionally, some mutations compatible with protein production (e.g., some missense changes) are well established as disease-causing and as sufficient to make a definite diagnosis of TSC.
Other variants should be considered with caution.
Genes responsible for TSC1 are located on chromosome 9q34 (hamartin) and TSC2 on 16p13.3 (tuberin).9, 10 Cardiac rhabdomyoma is the most common pediatric heart tumor, mostly occurring before the age of 1 year. Anatomically, they are considered hamartomas. Tuberous sclerosis is commonly associated with cardiac rhabdomyomas in 50 to 65% of patients and they may appear in the ventricular myocardium, the atria, the cavoatrial junction, or the epicardial surface. 11 Rhabdomyomas have a typical echocardiographic appearance. They are well-demarcated, round homogeneously hyperechoic masses, or discrete foci of thickened myocardium, most frequently located in the ventricles, 80% of cases in the LV, and 15% arising in the RV. They frequently occur in multiples and have not been reported to arise on cardiac valves. 12
Rhabdomyomas carry a relatively good prognosis and pursue a course of spontaneous regression partially or completely, with time. 12 Surgical resection is not advisable unless the patient is symptomatic. Definitive indications for surgery include cardiac outflow obstruction, valve dysfunction, persistent arrhythmias, cardiac failure, and cardiogenic emboli. 13 The symptoms may develop as a result of the obstruction of blood inflow or outflow, resulting in congestive heart failure necessitating pharmacotherapy with angiotensin-converting enzyme inhibitors, digitalis, and diuretics as required. Prostaglandin E can be used to manage hemodynamic instability in a critically ill newborn. Follow-up ECHO assessment at 6 to 12 months interval is advisable to ascertain involution of rhabdomyomas. 14
Arrhythmias can also occur ranging from bradycardia secondary to sinus or atrioventricular node (AVN) dysfunction to atrial tachycardia or VT, AVN re-entrant tachycardia, or ventricular pre-excitation. Antiarrhythmics are useful when there is atrial or ventricular arrhythmia. 15 These arrhythmias are unpredictable and can be the cause of sudden cardiac death rarely.
Although currently there is no cure for TSC, due to very slow progression, the prognosis is not as grim as has been typically thought. Prognosis depends on the extent of organ involvement, the number of tubers, the onset of seizures, and response to treatment, and the presence of infantile spasms. Children with infantile spasms and refractory seizures carry a greater risk of intellectual deficit. Rhabdomyomas and arrhythmias can rarely cause features of congestive heart failure and sudden cardiac death, as noted in one of our cases. Of the diagnosed TSC cases, 30% die before the age of 5 years, and 50% to 75% will attain adult age. 16 The general principle of treatment in TSC is symptomatic and very rarely operative for excision of obstructing rhabdomyoma or astrocytomas. Drugs that may be useful are antiepileptics, topiramate, and adrenocorticotropic hormone. 16 Oral and topical rapamycin has been shown to cause regression of astrocytomas and angiofibromas associated with TSC, and may eventually be an alternative to operative therapy.17, 18
Learning Points
In children less than 1 year, cardiac rhabdomyomas are the most common hamartomatous tumors.
Tuberous sclerosis is commonly associated with cardiac rhabdomyomas which require no specific therapy in the absence of symptoms.
Arrhythmias may be responsible for sudden cardiac death, especially in infants. In the absence of recommendations, prophylactic use of antiarrhythmic agents is debatable.
Conclusion
Tuberous sclerosis is a multisystem genetic disorder, with a significant number of patients showing cardiac involvement. Cardiac involvement is mostly in the form of rhabdomyomas and various arrhythmias. Patients with cardiac manifestations need close follow-up for features of obstruction to blood flow due to rhabdomyomas and for possible fatal arrhythmias which are unpredictable and rare. Whether TSC patients with rhabdomyoma need to be put on prophylactic antiarrhythmic therapy, is not clear at this point.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.