
Abstract
Background:
High altitude is associated with altered cardiovascular, pulmonary, and blood physiology which can lead to various cardiovascular complications. The world is now facing grave pandemic of COVID-19, which has affected all regions of the world including high-altitude regions. Management of COVID-19 infection along with a medical emergency like acute coronary syndrome at high altitude is extremely challenging.
Case Presentation:
We present a 57-year-old paramilitary officer, acclimatized to high altitude who developed sore throat, fever, and cough while he was posted at an altitude of 3,500 m. Evaluation revealed positive reverse transcriptase polymerase chain reaction (RT-PCR) test for COVID-19; hence, he was managed in isolation ward with symptomatic therapy. During the hospital stay, he developed anterior wall ST-elevation myocardial infarction (STEMI) for which he underwent thrombolysis with Tenecteplase. He underwent air evacuation to a tertiary care center located at an altitude of 320 m. Three days later, his repeat RT-PCR was negative. However, he complained of angina at rest; hence, he underwent coronary angiography which revealed significant mid-left anterior descending artery disease for which percutaneous coronary intervention was done successfully. Patient was discharged on optimal medical management, and on follow-up at 1 month he remained asymptomatic.
Conclusion:
This case highlights the deleterious effects of high altitude on cardiovascular system which can get worsened by COVID-19 infection. In patients suffering triple whammy of high-altitude exposure, COVID-19 infection and STEMI, multipronged approach involving timely medical management, rapid evacuation, and necessary intervention can provide optimal clinical outcomes.
Background
High altitude is associated with altered cardiovascular, pulmonary, and blood physiology which can lead to various cardiovascular complications. ST-elevation myocardial infarction (STEMI) is a medical emergency associated with significant morbidity and mortality. However, there are very few reports of STEMI at very high altitude.1-3 STEMI occurring at high altitude poses challenges not only related to pathophysiology of cardiovascular system at high altitude but also related to lack of rapid transportation and nonavailability of adequate medical resources leading to delay in optimal treatment. Any patient of STEMI with additional illness can drastically reduce the advantages of standard treatment offered to the patient. In this era of COVID-19 pandemic, our knowledge about viral illness effecting cardiovascular system has magnified due to widespread research. COVID-19 infection is associated with adverse cardiovascular events. 4 Thrombosis is the common pathophysiology which binds both high altitude 5 as well as COVID-19. 6 We report a patient who endured triple whammy of high-altitude exposure, COVID-19 infection, and STEMI.
Case Report
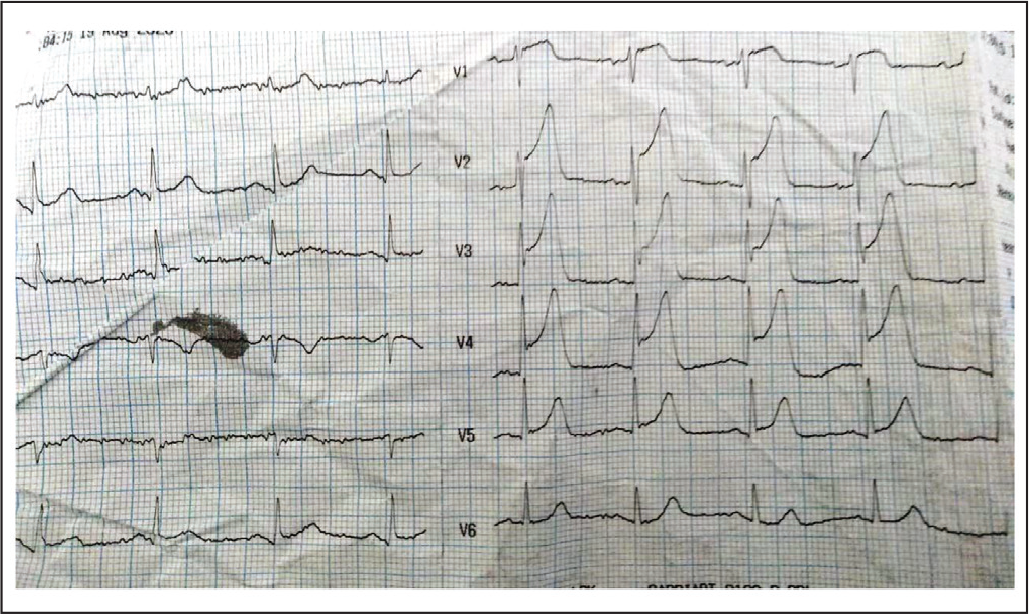
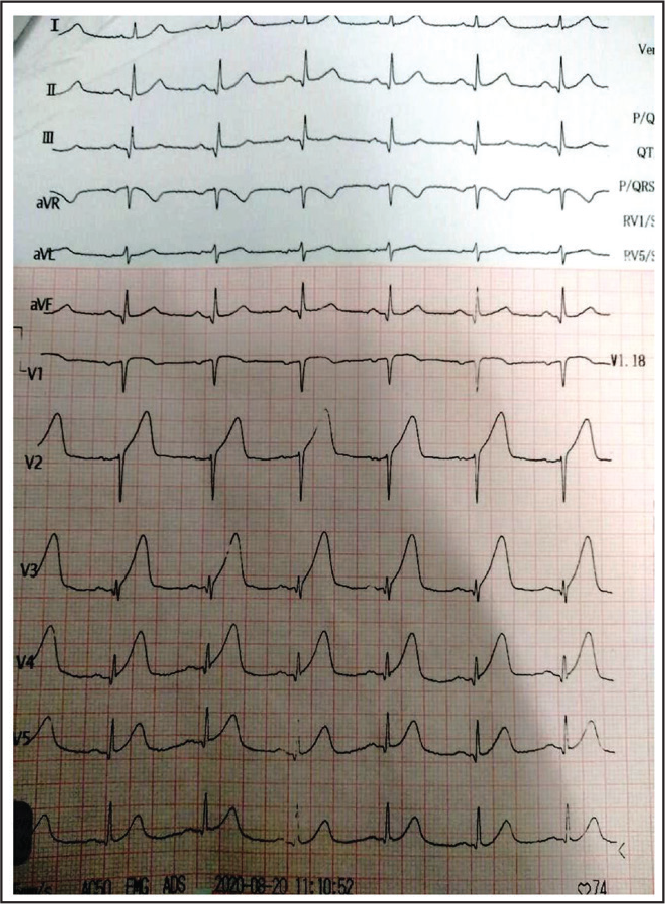
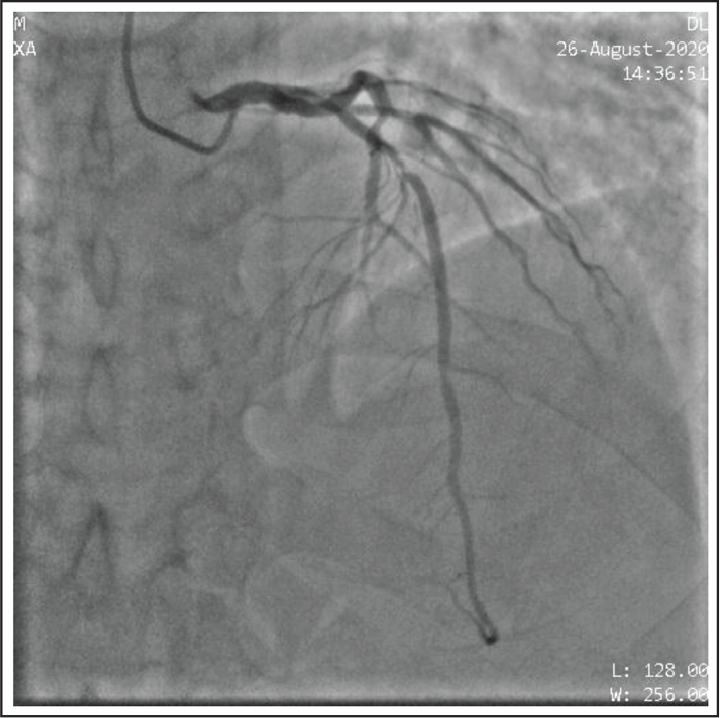
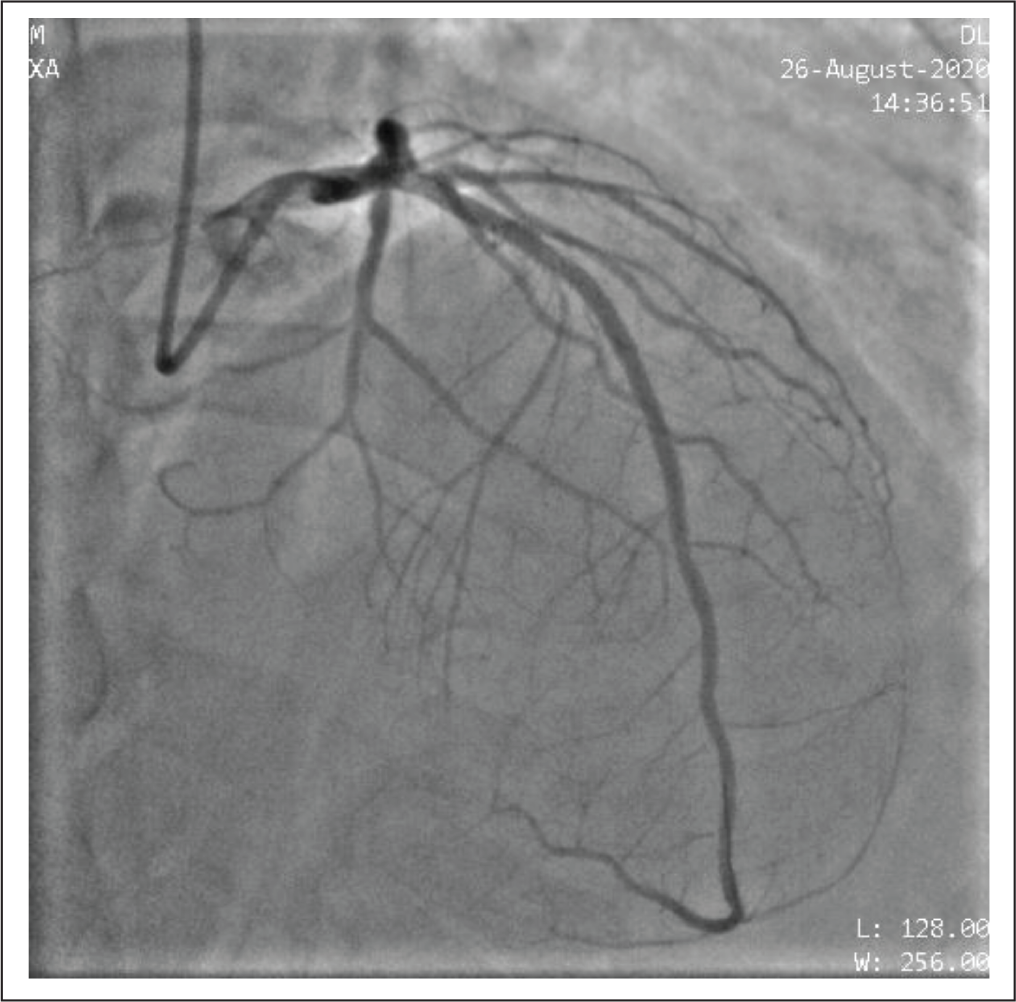
A 57-year-old healthy male was staying at a military facility located at an altitude of 3,500 m after due acclimatization protocol. He had no past history of diabetes, hypertension, or coronary artery disease. He developed low-grade fever, sore throat, and cough. He was placed in quarantine on day 2 of illness and underwent reverse transcriptase polymerase chain (RT-PCR) for COVID-19, which came out positive. He was managed with paracetamol. On day 3, he developed acute onset chest pain. Clinically, he was hemodynamically stable with pulse of 70 per min, blood pressure of 126/74 mm of Hg, and SpO2 of 96% at room air. His electrocardiogram (ECG) revealed ST elevation in leads V1 to V5 (Figure 1). He was diagnosed as a case of anterior wall STEMI and started on aspirin, clopidogrel, statins, and low-molecular weight heparin. Since primary percutaneous intervention (PCI) facility was not available in near vicinity, patient underwent successful fibrinolysis with Tenecteplase within 2 h of onset of chest pain successfully. Post fibrinolysis, patient had symptomatic relief as well as significant resolution of ST elevation on ECG (Figure 2). His oxygen saturation as well as chest X-ray (CXR) were normal. Due to inclement weather condition, he could not be immediately shifted to a PCI-capable hospital. He remained asymptomatic and on day 5, he was shifted to a dedicated COVID-19 center at a tertiary care hospital located at 320 m altitude by air evacuation. All precautions required to transport a COVID-19 patient were followed. His repeat RT-PCR was still positive for COVID-19. On day 8, his repeat RT-PCR came out negative. Laboratory investigation involving hematological and biochemical parameters was normal. His CXR was also normal. However, on day 9, he developed rest angina without any fresh ECG changes. Patient was hemodynamically stable; however, biomarkers were elevated (Troponin I-5.26 ng/mL and BNP-247 pg/mL). His echocardiography revealed regional wall motion abnormalities in left anterior descending artery (LAD) territory with ejection fraction of 40%. He underwent coronary angiography via radial artery access which revealed thrombotic lesion extending from proximal to mid LAD (Type 3 LAD) causing maximum 85% occlusion (Figure 3). All the cardiac catheterization protocols were followed as per COVID-19 positive patient. After informed written consent, drug-eluting stent (XIENCE Xpedition 3 mm × 48 mm) was deployed successfully with thrombolysis in myocardial infarction (TIMI) III flow (Figure 4). Patient was kept under cardiac monitoring for 24 h, during which he remained asymptomatic. He was discharged on day 11 with advice for dual antiplatelet, statin, ramipril, and beta blockers. On follow-up at 30 days after discharge, patient remained asymptomatic.
Electrocardiogram (ECG) Showing ST Elevation in Leads V1 to V5 Suggestive of Anterior Wall ST-Elevation Myocardial Infarction (STEMI).
Post-Fibrinolysis Electrocardiogram (ECG) Showing Significant Resolution of ST Elevation.
Coronary Angiographic Image Showing Proximal to Mid LAD Thrombotic Lesion Causing Maximum 85% Occlusion.
Coronary Angiographic Image After Percutaneous Coronary Intervention (PCI) Showing Resolution of Occlusion in LAD.
Discussion
Though exact definition of high altitude is controversial, many researchers have used ranges from 1,500 m to 3,000 m. 7 Altitude above 3,500 m is usually considered as very high altitude. Patient travelling to high altitude is at the risk of high altitude illness like acute mountain sickness, acute pulmonary edema, and so on. Few studies have shown that extreme stress caused by high altitude on the human cardiovascular system leads to various adaptation measures which may offer protection from myocardial ischemia and myocardial infarction. 8 It has been seen that in healthy subjects, epicardial coronary blood flow can increase secondary to vasodilation after acute high-altitude exposure, at least up to 4,500 m. 9 On the contrary, a study by Corante et al 10 on Andean highlanders showed that excessive erythrocytosis associated with high altitude can lead to increased cardiovascular risk in the population. Despite extensive research, there are scanty reports of STEMI at very high altitude.1-3 In a study by Al-Huthi et al, 11 high altitude (1,500-3,500 m) was associated with increased risk of acute coronary syndrome (ACS), which was associated with more adverse outcomes to those compared with presentation at low altitude. Basavarajaiah and O’Sullivan 12 have reported 2 cases of stent thrombosis; however, no causal relationship with high altitude could be established. Our patient in the case report had no other traditional risk factor for acute myocardial infarction (AMI) apart from age and male sex.
COVID-19-affected patients can develop various cardiovascular complications like myocardial injury, myocarditis, AMI, heart failure, dysrhythmias, and venous thromboembolic events. Due to extensive inflammation and hypercoagulability, the risk of AMI is high in patients with COVID-19. Though venous thrombosis is much more common in COVID-19, arterial thrombosis including STEMI has also been reported. 13 In addition to direct relation with pathophysiology of STEMI, this viral pandemic has adversely affected many other aspects of STEMI care, including timely access to the cardiac catheterization laboratory for primary PCI. 14 Though timely primary PCI has become gold standard treatment for STEMI, fibrinolysis can provide immense clinical benefits especially during this pandemic when access to catheterization laboratory is associated with considerable delay. In fact, in Strategic Reperfusion Early after Myocardial Infarction (STREAM) study, the composite outcome of death, shock, congestive heart failure, or reinfarction up to 30 days was similar between patients who presented within 3 h of STEMI and underwent fibrinolysis versus primary PCI. 15 The patient in our case report underwent successful fibrinolysis within 2 h of onset of symptoms. The causal association between COVID-19 and STEMI in our case could not be conclusively proven.
We postulate that both high altitude and COVID-19 infection were predisposing factors for STEMI in this patient. He encountered adverse pathophysiology associated with high altitude and STEMI, coupled with delays in management due to environmental conditions and COVID-19 infection. Fortunately, he did not develop any COVID-19-related acute lung injury, which allowed good clinical outcomes despite triple whammy of high-altitude exposure, COVID-19 infection, and STEMI.
Learning Point
This case highlights the fact that effective clinical protocols, rapid evacuation, and meticulous intervention can provide optimal outcomes in medical emergencies even in adverse circumstances.
Conclusion
Very high-altitude exposes human cardiovascular system to extreme stress. In such adverse environmental condition, ACS such as STEMI is difficult to manage due to clinical factors, environmental factors, and associated logistics. COVID-19 virus makes pulmonary and cardiovascular system vulnerable; hence, any such patient living in high altitude is susceptible for additional risk of cardiovascular compromise. Patient at high altitude having concurrent COVID-19 infection as well as ACS faces triple whammy which can create adverse clinical outcomes. Fortunately, our patient was able to survive triple whammy of high altitude, COVID-19, and STEMI.
Author Contributions
All co-authors have reviewed and approved of the manuscript prior to submission. RC: Collected the data and wrote the paper. KP: Collected the data and wrote the paper. KSV: Wrote the paper. RMK: Conceived the case and wrote the paper.