
Abstract
Aims and objectives:
To investigate reflections on wishes and needs of adults living with the life-threatening disease Duchenne muscular dystrophy (DMD) to target future rehabilitation.
Background:
Adults with DMD have a short life expectancy with a mean age of death at 26.8 years. Despite this, palliative rehabilitation is sparsely mentioned in standards of care. Relatives and healthcare professionals seem to find it difficult to talk about the future and future care with people living with a life-threatening disease.
Design:
The design of the study was qualitative using the Interpretive Description Methodology and the salutogenic theory of Sense of Coherence (SOC) as the theoretical framework.
Methods:
The method was individual semi-structured interviews with 13 adult men with DMD. The interviews were conducted from February to March 2025.
Results:
Navigating life with DMD was considered a condition of life, and being able to accept and adapt to uncertainties were effective coping mechanisms affecting the participants’ overall SOC. Furthermore, living with a life-threatening disease was managed by living one day at a time, finding solutions, taking life as it comes, and getting the best out of it. Also, having dreams like everybody else, despite the uncertain future, was important. Finally, talking about future care felt strange to the participants, but it was easier if someone dared to ask directly. Timing and addressing individual needs were essential.
Conclusion:
Adults living with DMD appreciated the opportunity to talk about their wishes and needs for the future. Healthcare professionals are recommended to initiate conversations about biopsychosocial and existential issues, and palliative rehabilitation is recommended throughout the DMD lifespan with attention to individual needs, timing, and state of the disease.
Plain language summary
This study investigated how adults living with Duchenne Muscular dystrophy (DMD) in Denmark reflected on their wishes and needs for the future. Although life expectancy with DMD is short, palliative rehabilitation is sparesly mentioned in care programs and rarely talked about with health care professionals. The design of the study was qualitative, and 13 adults were interviewed from February to March 2025. The study emphasized that adults living with DMD were good at coping with their disease and adapting to uncertainties. They took one day at a time, found solutions, took life as it came and got the best out of it. They had dreams about the future like everybody else even though it was uncertain. They were unfamiliar with talking about future care but found it easy when asked directly. The participants in this study appreciated the opportunity to talk about future wishes and needs. We recommend that healthcare professionals start conversations about thoughts, wishes and needs for future care with patients who live with a life-threatening disease. We recommend that people with DMD receive palliative rehabilitation throughout their lifespan which is adjusted to individual needs, timing, and state of the disease.
Keywords
Introduction
Duchenne muscular dystrophy (DMD) is a severe and progressive neuromuscular disease (NMD) caused by a mutation in the dystrophin gene.1,2 The absent and insufficient functional protein causes muscular damage and degeneration, resulting in muscular weakness, motor delay, loss of ambulation, respiratory impairment, and cardiomyopathy. 1 DMD has a dominant X-linked maternal inheritance and almost always affects males, but ultra-rare female cases have also been reported in the literature.1,2 The prevalence of DMD is 1 in 3600–6000 male births. 3 The earliest symptoms are seen at 2–3 years of age with motor delays such as waddling, difficulties climbing stairs, and getting up from the floor. 4 Treatment with corticosteroids, revised standards of care, and improvement of respiratory and cardiac care has postponed loss of ambulation until around 13–14 years of age.2,4 The improvement of respiratory support has resulted in a shift in causes of death from respiratory failure to acute cardiac events, and the mean age of survival has increased. 4 In Denmark, most adults living with DMD will eventually use an invasive ventilator and live independent lives. 5 Mean age of death in a Danish population was 26.8 years (interquartile range 19–34 years). 3 Living with a progressive disability and shortened life expectancy should increase attention to palliative care; however, there is a need to educate health professionals and perform more research related to palliative care in NMDs. 6
Palliative and end-of-life (EOL) care are only sparsely mentioned in the standards of care for management of DMD. 1 A systematic review from 2017 found a limited amount of literature dealing with EOL conversations with young people with NMDs. 7 Palliative care is often introduced late, and conversations about EOL care are often postponed until acute or critical illness appears. 8 A study from the United Kingdom revealed that none of the participating DMD men remembered having spoken with a clinician about EOL. 9 Standards of care and management of DMD mainly focus on the physical symptoms and less on how lives are lived.1,10,11 The literature in this field is sparse, and clinical practice in Denmark does not systematically combine the rehabilitation of adults with DMD with palliative care. As with other NMDs, rehabilitation assists and focuses on adaptation to challenges of living with a progressive disease, and palliative care is essential to improve quality of life (QOL) living with a life-threatening disease. 12
Studies often focus on the caregiver’s perspective of living DMD, and there is a lack of perspectives from the point of view of the adults with DMD. Therefore, the aim of this study was to investigate the reflections on wishes and needs of adults living with the life-threatening disease DMD to target future palliative rehabilitation.
Methods
Design
The design was qualitative, and the methodology was Interpretive Description (ID). 13 The study was inspired by the theoretical framework on salutogenesis and Sense of Coherence (SOC) by Aaron Antonovsky. 14
Setting
The study was conducted at The National Rehabilitation Centre for Neuromuscular Diseases (RCFM), and data was collected in March 2025. RCFM is a highly specialized tertiary hospital for NMDs in Denmark. 15 RCFM uses a multidisciplinary, person-centered approach to enhance activity, participation, and QOL. 16 The services provided by RCFM are free of charge and funded by the Danish healthcare system. 17
Recruiting and participants
Study participants were recruited from RCFM’s patients register, which includes the entire Danish population with DMD. In January 2025, the population counted 93 persons aged 18–52. Inclusion criteria were adults ⩾18 years of age with a genetically confirmed diagnosis of DMD. Persons who were verbally and cognitively affected and unable to participate in an interview were excluded (12 individuals). 18 Based on the study criteria, 40 people were invited to participate by random selection and via Secure Digital Mail. People who did not respond to the invitation were contacted by phone. A total of 13 non-ambulatory men with DMD was included in the study (Table 1 and Figure 1). Patient involvement was used to ensure relevance for the study population. Two people with DMD were purposely selected to give feedback on the invitation and interview guide and to participate in a pilot interview.19,20
Participant characteristics (n = 13).


Flowchart for recruiting participants.
Data generation
Individual interviews were used for data generation. 21 A semi-structured interview guide with open-ended questions was developed (Table 2). Two pilot interviews were included in the dataset.
Semi-structured interview guide.
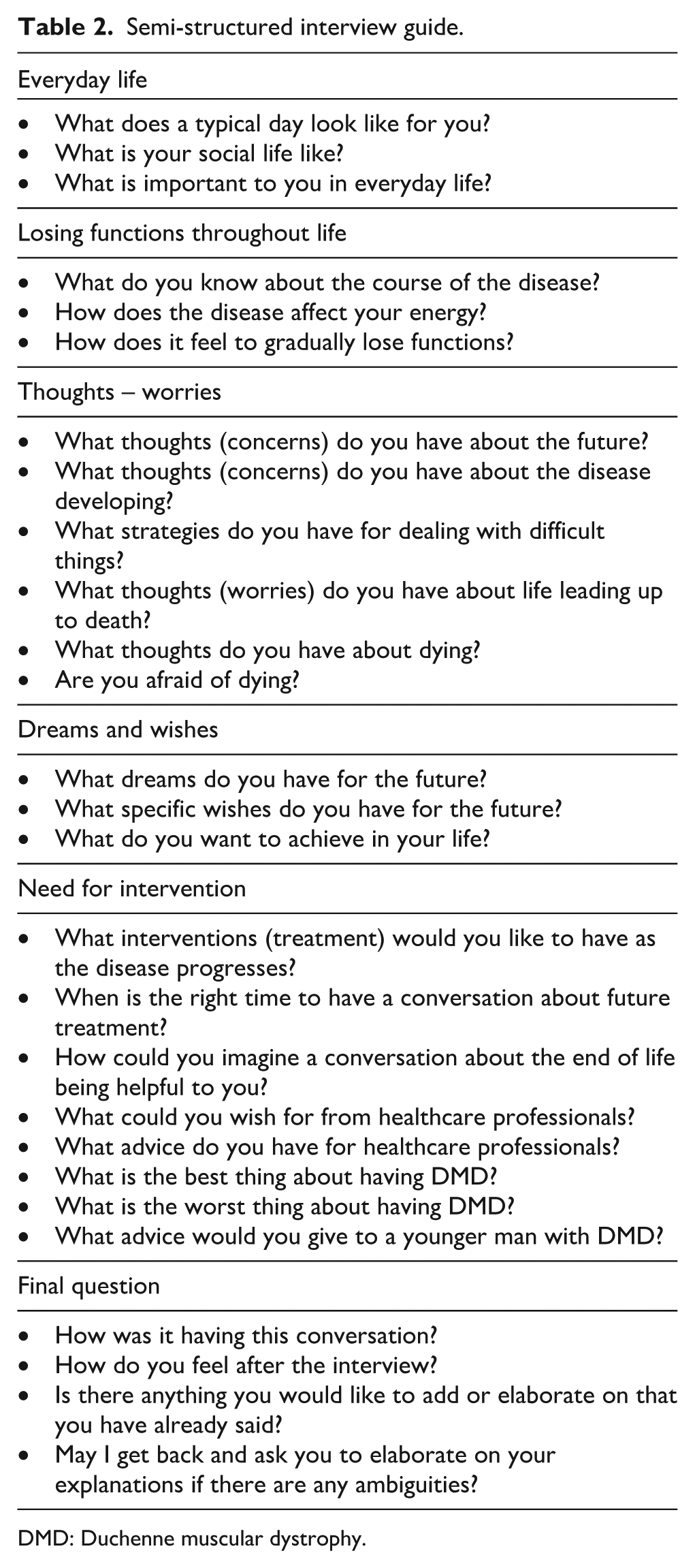
DMD: Duchenne muscular dystrophy.
All interviews were conducted by the first author. Eleven interviews were conducted in the participants’ private homes, and two were conducted online due to geographical distance. Interviews lasted between 34 and 66 min, with a mean of 54 min.
Interviews were recorded on audio files, and transcription was made with Transcriber 1.6, an AI-powered speech-to-text service. Trancriber was available trough the GDPR-regulated database UCloud, a platform for interactive High-Performance-Computing in Denmark. The raw transcription file was corrected while listening to the complete audio file.
Data analysis
The ID methodology guided the data analysis.13,22 The aim of ID is to improve healthcare practices, and research questions must arise from experienced challenges and problems. 13 The methodology is inductive and strives to create new insights, understanding, and knowledge to the clinical field. 13 ID expands the descriptive part with interpretation to find connections and patterns in data that can contribute to theory development and practical implications. 22
During the interviews, the concept of using Aaron Antonovsky’s salutogenesis theory emerged and was subsequently employed inductively inspiring the analysis of the data as a theoretical lens.13,14 Salutogenesis focuses on components that promote health and well-being rather than on factors that cause disease. 14 To experience a high SOC, one must score high on the core components, comprehensibility, manageability, and meaningfulness. 14 The theory was relevant for gaining insight into how to handle stressors, coping, and managing life with a lifelong progressive disease.
The analysis was an inductive and iterative process following ID’s four steps of analyzing.13,22 (1) Initial content analysis and coding were done by both authors. Focus was to seek patterns and connections that would reveal relevant themes and subthemes and lead to a coding framework. (2) Data were uploaded to Nvivo™ 15, a software for qualitative data analysis. Transcripts were reread, and the coding framework guided the first author in categorizing data by clustering meaningful information, patterns, and connections (Table 3). (3) Extraction of meanings and patterns was captured from the final themes and analyzed through the theoretical lens of SOC. (4) The key themes were finally identified by both authors and illustrated in a model13,22 (Figure 2).
An illustration of the coding and analysis process in the categorical theme: Living in the present, the clock is ticking faster.
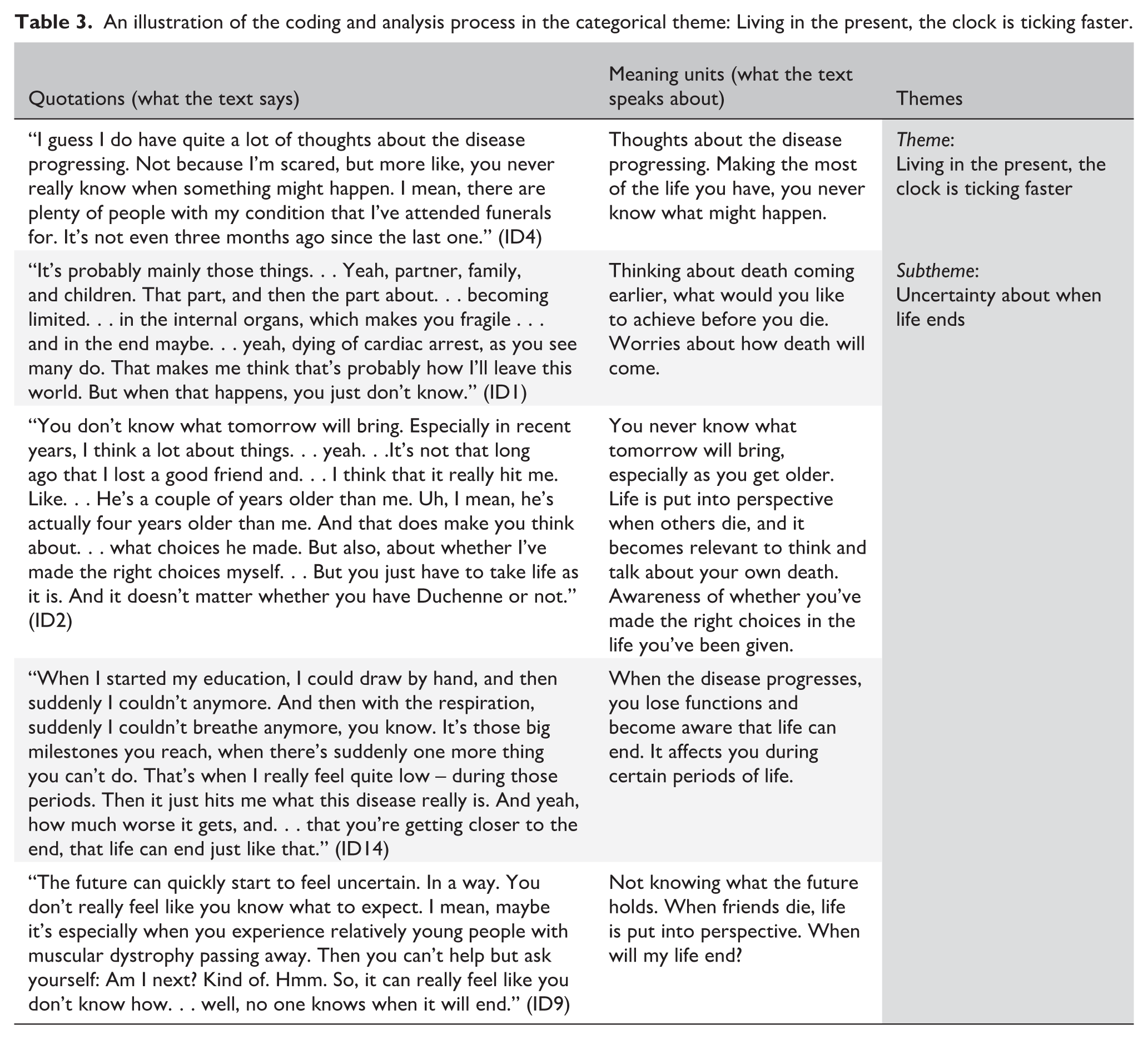

Illustration of the inductive analysis and coding process leading to the final themes. Guided by the Interpretive Description Methodology and the theoretical lens of Aaron Antonovsky’s Sense of Coherence Theory.
Ethics
This study was conducted in accordance with the Declaration of Helsinki. 23 According to the Central Denmark Committee on Health Research Ethics, the study could be conducted without approval from the Committee [Request no. 1-10-72-103-24]. All participants were informed orally and in writing, and consent was obtained from all participants. The participants were guaranteed anonymity and could withdraw their consent at any time.
Results
The study gave new insights into living and navigating with a life-threatening disease from an adult perspective. The prospect of premature death was regarded as a condition of life. Finding meaning in the disease and getting the best out of life were repeated themes. Being acknowledged as experts and being listened to were the participants’ most important messages to healthcare professionals. Dealing with progression was a condition and living in the present and taking life as it comes were coping strategies to manage uncertainties. The participants valued having social relations, but as they grew older, they also enjoyed their own company. Having dreams for the future, like everybody else, supported a feeling of normality, even if realizing their dreams were difficult. The participants had thoughts about the future which they rarely spoke about, but when asked directly, they willingly shared (Figure 3). Antonovsky’s theory about SOC guided the understanding of how managing, comprehending, and being able to find meaningfulness was possible for adults living with DMD.
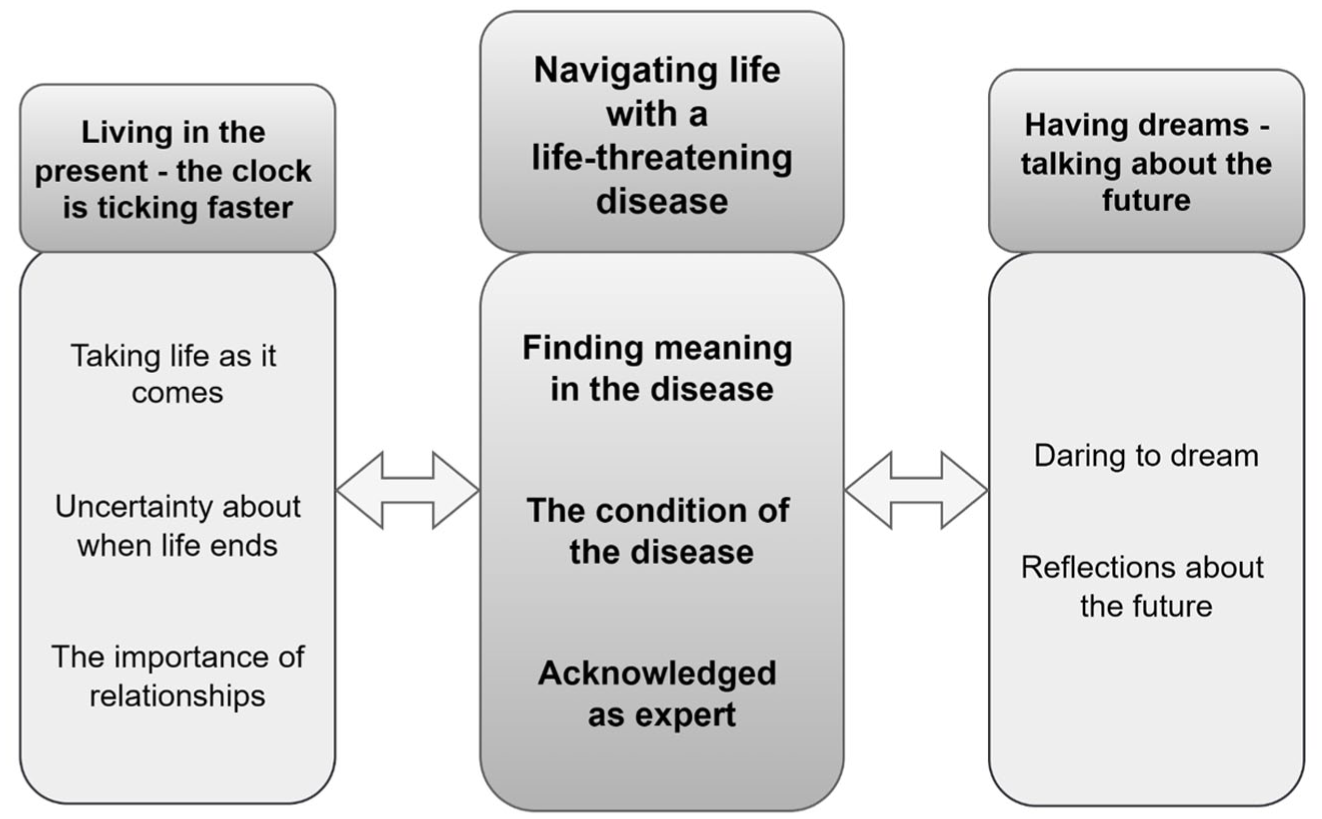
Illustrating reflections of adults with DMD living with a life-threatening disease.
The participants offered advice for younger people living with DMD and for healthcare professionals based on their lifelong experience (Table 4).
Advice for boys with DMD and healthcare professionals from adults with DMD.

DMD: Duchenne muscular dystroph.
Navigating life with a life-threatening disease
Finding meaning in the disease
All participants described the importance of being able to participate and contribute to this study and to society. They pointed to the importance of giving a different perspective on life, showing how to live with disability, and being a role model for others living with DMD. Participants were able to find meaning in the disease and think positively about what it contributed to. Having DMD gave them a positive mindset and helped them focus on what they could do.
I guess the best thing about having DMD is the person you become. All the shit that comes with the disease, it also changes who you are, . . .it changes a person to have such a life-threatening disease. I think it has made me a better person, I have no doubt about that because there are so many shitty things in your life, so you have to focus on all the things that are good. (ID2 in his 30s, invasive ventilation (IV))
The participants said that with all the problems and losses in life, it was important to find a mindset with which life was worth living, to be grateful, participate, and contribute. Some said that their perspective on life had made them better, wiser, and more empathic persons.
The best about DMD is the perspective on life. . . I have more empathy for people and understand other people’s problems better. . .it’s because I have been through some difficult things and have a different perspective on life which have made me stronger. . . adversity has made me stronger. (ID3 in his 40s, IV)
Finding meaning in living with DMD, finding solutions, and managing life were important to support a high SOC. All the participants had vast experience of living with the disease, and the condition forced them to get the best out of life. Most of them had accepted life’s circumstances but still grieved, being unable to do the same as everybody else.
The condition of the disease
Living with a chronic life-threatening disease affected all the participants, and they reflected on the constant disease progression and how it restricted them. They saw DMD as a condition of life and had learned to deal with the gradual loss of functioning, were aware of the constant progression and tried to prepare for and adapt to future loss of function, despite never getting used to it. The participants felt the disease was quite stable and that major losses, like ambulation, had happened years ago. Progression or acute illness reminded them of the severity of the disease. One of the biggest and most challenging interventions in adulthood was getting IV.
It’s been a very long time since loss of functioning was on my mind. . . . I mean, after the big stuff, the bigger things when I lost ambulation, couldn’t feed myself, couldn’t turn in bed. The big things occurred many years ago. My neck’s a little weaker and I can’t sit like before, but otherwise, I don’t think about it very often. It progresses very slowly. Or how can I put it? It’s not slow. . . But when you can no longer do much, nothing really changes. (ID4 in his 30s, IV)
The limitations of the disease in adulthood influenced many facets of life. The participants’ gradual loss of muscle strength and functioning affected their physical and mental energy. Physical impairment increased their need for assistance, while reduced mental energy led to more rest and staying home. Other impairments restricted social participation; a weakened voice, slurred speech caused by a hypertrophic tongue, forced the person to become quieter and more observant.
I remember I started being unable to raise my voice in big crowds. . . No one can hear what I’m saying, and it’s been really difficult because I used to be able to speak up. For me, that’s one of the biggest impacts. It’s been annoying. (ID5: man in his 20s, non-invasive ventilation (NIV))
All the participants reflected on accepting the gradual impairment. They managed by finding new solutions, focusing on the positive, holding on to what was important, and accepting their new condition. Some participants coped with impairment by seeking solutions in assistive devices and technologies, and they appreciated living in Denmark where they were provided with personal assistance 24 h a day.
There’s always grief related to loss of functioning. Now you can’t. . . But it hasn’t taken me very long to get over it. It’s mainly finding new ways to do it. . . . saying never mind, you can’t do anything about it. And then get your personal assistant to do it instead, or people around you can help. (ID1 in his 20s, NIV)
Acute illnesses like the flu or pneumonia were described as a sudden progression that caused new limitations in activity and participation. Returning to the same physical level as before an illness was often difficult. They knew about the stages of the disease; some knew all the details, and others would deliberately not relate to future progression until it occurred.
Before I turned 18, I was afraid others would find out that my illness could be life-threatening. I was afraid and wanted to protect myself. I didn’t really want to face the fact that it was a life-threatening disease. I knew that I could easily get in-depth information about my illness, but I didn’t dare do a google search. I tried to push it away, but deep down I knew the reality. In my early teens, I didn’t know that my illness was life-threatening, but it slowly dawned upon me. (ID6 in his 30s, NIV)
Living with a life-threatening disease made the participants aware of their ongoing loss of function. Comprehension and acceptance of disease progression were coping strategies to support a high SOC. Manageability and meaningfulness were supported by seeing the positive things and finding creative solutions. Still, the participants said they never got used to the progression and ongoing impairments that kept limiting their ability to participate and live as before.
Acknowledged as an expert
Having a rare disease like DMD created a need for being recognized as an expert on one’s own life. Having a voice and being acknowledged were important to the participants. Being unable to manage and control all aspects of life with a life-threatening disease, it was important to take control over the things they could. Most of them learned about the disease progression by comparing themselves with older friends who also had DMD.
I would say I know a lot about the disease. I see it unfold in my peers with DMD and those who are older. So, I know a lot about it. I think my knowledge comes from listening to others with muscular dystrophy, primarily. You hear what they struggle with, like things I don’t know about and some of the side effects that you can have. (ID8 in his 30s, NIV)
The participants also described acquiring knowledge about the disease from physicians and RFCM; some had been well informed from an early stage; others had been in denial during their teenage years and had felt alone. Most participants realized the severity in their late teenage years when physical impairments became more obvious.
I didn’t think much about the disease when I was a child, not until the end of elementary school, when I started falling and couldn’t run. And then it was just like. . . I was a bit alone with it. (ID10 in his 20s)
When treated at local hospitals, most participants felt they had to be experts on the disease to secure the right treatment and demanded that specialized units were involved when necessary. They advocated for an individual approach from healthcare professionals and the importance of listening and asking questions.
They just don’t listen. I had just had a fracture. . . . I was supposed to come in and have it looked at. Then he asks me twice if I could stand up. I mean, what the hell do you think, I have DMD? . . . And he didn’t really listen at all. (ID1 in his 20s, NIV)
The participants appreciated the regular – especially cardiac and respiratory – checkups and seeing a neurologist or rehabilitation specialist; they felt safe when talking with a specialist. They emphasized the importance of checkups to avoid overlooking them as adults. Being acknowledged as experts supported manageability. Having a voice was essential, and their most important message to healthcare professionals working with DMD was to listen and treat them as individuals with special needs. The central theme of navigating life with DMD and adapting to diverse life circumstances led to the theme about living in the present was a recurring topic in interviews.
Living in the present – the clock is ticking faster
Taking life as it comes
The participants described that everyday life was good when physical and mental conditions were stable, and even though life was filled with practical challenges, it was still considered worth living.
Of course, it’s always difficult when you’re losing functions. I’d be lying if I said it was a walk in the park. But on the other hand, everyone loses functions over time. It just comes sooner for us. And then there’s the upside that you can really appreciate what you have now and what you can do now. (ID9 in his 30s, NIV)
The importance of enjoying life and living in the present was significant, and many participants made statements like “You only live once.” Progression was described as a life condition, and accepting the life they were given was important. The men preferred to get the best out of life, not wasting energy on lost causes and seeing possibilities rather than limitations.
I’m always very good at looking on the bright side. You only live once, so enjoy it as much as you can. Well, that’s always been my strategy. To do everything while you can, I mean live life, quite simply. I’m just unfortunate to have this disease. There’s nothing I can do about it. I must live with it and make the best of it. That’s what I’ve always thought. (ID5 in his 20s, NIV)
Losing functions was a normal part of life, which the participants had learned to accept. They said they did not or did not want to give much thought to the fact that life might be short and that sadness and grief over what was lost became less pronounced with time.
When you have DMD, all your physique slowly declines, and you have time to continuously work through various physical limitations. I think that’s a big part of the reason why you can get up every day and still be happy. I’ve had DMD for so many years and I am used to all the thoughts that come with the disease. . ., and the physical limitations come just as slowly. In addition, I don’t have an alternative. So, if I’m sad about it, it’s not going to be easy. When you don’t have an alternative and you’ve been in it for so many years and you’ve thought long enough, you reach a point where you can't be sad anymore. (ID6 in his 30s, NIV)
Even though functional loss was a life condition, it seemed like the participants were able to manage life, find meaning, and live in the present. Comprehending the disease and life situation seemed to be easier as life went by. Those are competencies that can initiate and promote a higher experience of SOC.
Uncertainty about when life ends
Knowing the risk of early death enhanced their desire to live in the present and find meaning in life. The participants described death as being close, yet distant. They had all lost friends with DMD, and some described how death had become part of their everyday life. The participants explained that having friends who died put life in a different perspective, giving rise to thoughts about one’s own condition, the progression of the disease, the uncertainty, vulnerability, the uncontrollable nature of the disease, and never knowing what tomorrow would bring.
When friends die, I realize what the disease is like and how much worse it will get, also, you get closer to the end, life can be over at any moment. Every time another person with DMD dies, reality really strikes, I start thinking about all the things I want to achieve and stuff like that. But fortunately, I think I’ve always been able to enjoy what I have and go out and do things and have fun. (ID13 in his 30s, IV)
The participants explained that they tried not to think about the future because of the risk of a negative mindset. Thoughts about death would pass and were mostly discussed in connection with friends who had died and acute illness. They described being aware of their shorter life span and coping with it by living in the present and being proactive in living out their dreams.
I don’t know how I’ll feel in a year or what the world will look like in a year. Yeah, a lot of things can change, so I think I just try to make the best of what I have. I think I have many thoughts about the progression of the disease. Not because I’m afraid, but also because I never know when something will happen. Things can quickly take a completely wrong turn. (ID4 in his 30s, IV)
Thoughts about dying and death were distant most of the time and appeared only to emerge in connection with acute illness and friends dying, but when asked about death, they did not mind talking about it, although it was difficult. They appeared to have developed strategies to cope with life and manage gradual losses but did not talk much about them; however, they are factors that may influence all three core components of salutogenesis, promote health and well-being and shape the experience of SOC.
The importance of relationships
The participants described that social life had changed over the years. Progression of the disease resulted in less energy and spending more time at home. Some were satisfied with the number of people in their lives, while others wished to be part of a bigger community. A few of the participants struggled with meeting new people. Parents and siblings were important relatives in adult life, and it was safe to talk about difficult issues with them, but difficult to talk about dying and death. They shared concerns about the disease with peers but rarely discussed dying and death. In general, they did not talk about difficult issues with anyone. The participants mentioned having important relationships with their personal assistants, who were not considered merely employees but friends with whom they could share most things.
Sometimes you feel like your personal assistants are the ones closest to you, they become your friends. Do you really need more? The only people I don’t talk about life and death with is my family, when it comes to my illness. I think I could get my parents to talk about it if I wanted to, they’ll always help me. But I haven’t felt the need to talk to them about it yet. (ID6 in his 30s, NIV)
The participants described various kinds of friendships, all mentioning that being able to do something for other people and having social relations were crucial to staying mentally healthy.
Yes, it’s important for me to have good relationships, because I feel that’s the most important thing, because then everything else is irrelevant. That’s it. That’s certainly what I care about the most, so yeah, my mental health is probably what I care most about. (ID10 in his 20s)
The number of relationships did not seem to determine whether social life was good. It appeared that parents and siblings played an important role throughout life, and having a family made a difference in being satisfied with social life. Some participants developed friendships with their personal assistants, which prevented loneliness. Friends and family were crucial in times of acute illness and disease progression, supporting manageability and helping with big decisions in life to promote a greater SOC. Appreciating life despite its uncertainties and valuing relationships paved the way for the final theme concerning dreams and reflection about an uncertain future.
Having dreams – talking about the future
Daring to dream
Living with a life-threatening disease meant that some participants did not have any dreams for the future. They tried to stay positive and accepted that the condition put a limit on their dreams and wishes.
When I was younger, I had many dreams about the future, but now I feel that I am satisfied with the life I have today. I guess I don’t have that many expectations for the future, like getting a girlfriend, like most people still want. I think I have accepted that it’s not going to happen. (ID3 in his 40s, IV)
Others dreamt about the same as other young men their age: relationships, being part of their community, traveling, and experiencing the world, but were aware that such dreams would most likely not come true.
There are many things I want to do. There’s a future and a wife and children and a house and whatever else people want. Just ordinary thoughts for a man, but like other people, I see it falling apart. It’s a heavy thought, because you know your time is limited. . . . I’m looking at a deadline. I know there are things I would like to have done before. . . . But it’s not certain they can be done, so I have to suck it up and take it as it comes. (ID7 in his 20s, NIV)
The men dreamt about an ideal life with no restrictions, but real life had its limitations. They described that it was difficult and almost impossible to imagine the future, alternating between dreams and reality. Some had already fulfilled their dreams by doing voluntary work and participating in sports. Others had dreams but no specific plans to make them happen, maybe as a way of protecting themselves from disappointment. This strategy could help support comprehensibility, manageability, and meaningfulness in life with an uncertain future.
Reflections about the future
The participants did not seem to reflect and talk much about the future in general, but when asked during the interview, they all openly shared their thoughts about difficult issues like progression and premature death, even though it was difficult to articulate and relate to. They indicated that timing was essential, but that the appropriate time for having this type of conversation was individual and depended on age and the state of the disease. All the participants appreciated being asked, stating it was nice to talk about these issues.
I think it’s been great to have this conversation. It feels good to just talk about it. Of course, there are a lot of things that we’ve talked about that I don’t think about every day. It’s also good to be forced to think about it. So, it’s fine, it’s probably started some new thoughts. However, I feel confirmed in my belief that I have the right attitude toward it. So that also gives me energy. (ID13 in his 30s, IV)
The participants stated that it required courage to talk about the future, and that it was easier when asked directly by someone who was willing to discuss it. They explained that even though the EOL was not near, having a conversation about it was useful, even if it was uncomfortable.
I thought it was interesting to have this conversation, and I think it is important that a bridge is built to have these good conversations. I think some people are more affected by these thoughts than others and don’t necessarily feel it’s so easy to talk about. I think there is potential in finding out how to open up the conversation or educate someone, so it feels safe talking about these things. The best thing would be a holistic effort, that you don’t feel that things are seen isolated, but it all affects your life, in a total package. So, it’s both what’s happening physically and mentally. And the framework for the conversation all plays a role. (ID8 in his 30s, NIV)
The participants seemed unfamiliar with talking about future care and treatments, but if someone asked about it, they accepted and appreciated it, and openly shared their thoughts. They indicated that if someone had the courage to ask and facilitate the conversation, it felt nice to talk about. Indicating that this might be a future intervention that could support a higher SOC when living with DMD as an adult.
Discussion
This present study provided new, important insights into the lives, dreams, and wishes for the future of adult men with DMD. Being aware of the seriousness of the disease, the men expressed a transient sadness when losing functions while still appreciating life despite their gradual impairment. This is in line with findings in a prior study addressing the phenomenon “disability paradox” that explains why people with serious and persistent disabilities report good and excellent QOL. 24 Antonovsky argues that people who have a high SOC are able to handle the stress they are exposed to. 14 The theory may help explain why the participants in our study could adapt and cope with uncertainties by living one day at a time and rarely looking into the future. Several studies about DMD and their caregivers have shown that people with DMD adapt to continuous disease progression and that uncertainties cause them to live 1 day at a time.25,26
A study by Rose et al. 27 reported that acceptance and effective coping skills were the most important determinants for QOL in patients with muscle diseases. Likewise, Garrino et al. 28 found that patients with rare diseases used adaptive strategies to cope, thereby improving QOL. Both our study and Pangalila 29 found that, experiencing disease progression throughout life, people with DMD seem to adapt and adjust their activities and goals continuously, which may influence QOL.
The participants in our study had personal assistants 24 h a day and they lived with NIV or IV. 30 In Denmark, a strong social and healthcare system pays for personal assistance to people with DMD, and a study by Dreyer et al. 5 found that having an invasive ventilator contributed to living independently. This context might influence the participants’ experiences and differ in settings with fewer resources. A recent Danish study on living with personal assistants found that the distinction between being a friend and being an employer could be complicated. 31 In our study, this issue was not addressed as a problem. A review on social relations, mental health, and well-being in people with physical disability found a consistent association between social support and mental health, with social support preventing negative consequences of the stressors caused by living with a disability. 32
The present study indicated that certain life events could initiate conversations about death and dying. Abbott and Carpenter 25 also found that premature death was not top of mind, but came into focus in case of acute illness, and the death of friends was also found in a study about the everyday lives of boys with DMD. In our study, the participants were aware of the severity of the disease, but the future and premature death were rarely discussed. Antonovsky’s description of how conversations about uncertainties and the ability to achieve comprehensibility and manageability can support SOC 14 was supported by the participants’ appreciation of conversations about the future. Being acknowledged as an expert and feeling responsible for their own care was essential, especially when admitted to local hospitals. A review of people with rare disorders supports the experience of having encountered uninformed healthcare professionals and having to be an expert on one’s own disease to get the right treatment. 33
In this study, the participants were unfamiliar with talking about future care, but when asked, they reflected and willingly shared their thoughts. Chrastina and Haroková 34 found that it was challenging for families to discuss EOL issues with their children with DMD, and they expected the topic to be brought up by professionals. Advanced care planning (ACP) 35 could be a relevant method for planning future care and pathways. ACP is a conversation between the patient, relatives, and healthcare professionals about the patients’ wishes for their final stage of life. 36 The rationale is that the earlier difficult topics are addressed and discussed, the easier it is to accommodate wishes and needs. 37 Timing is essential and should be initiated by healthcare professionals when the patient shows signs of wanting to talk. 38 To guide healthcare professionals, Willis et al. 39 have developed a traffic light system for NMDs to help identify and prioritize those who might benefit from ACP and palliative rehabilitation. The traffic light system could be a recommended screening tool to determine who may benefit from, and when to initiate ACP and palliative rehabilitation.
Study limitations
Experience from clinical practice has shown that adults with DMD can be difficult to reach, which was confirmed in this study. This might be explained by their broad cognitive profile, with risk of delays in cognitive and social development. 11 Representative credibility can be challenged by the small sample, with only 13 adults participating out of 93 eligible individuals in the national cohort, which may limit transferability. However, the participants in this study represented a variety of ages and disease stages, providing sufficient information power. 40 The ID methodology does not seek an endpoint at which saturation is reached; however, in this study there was a high degree of consistency in the information given. 22 There is a pronounced risk of bias in that we might have reached the most resourceful part of the population. However, one might argue that they are advocates for the most vulnerable in the population.
Individual interviews were used to gain in-depth knowledge of a rarely discussed sensitive topic. Interviews were conducted in the participant’s homes to create a safe and comfortable setting, which encouraged participation by removing the need to travel.
Epistemological integrity was sought by being transparent about the research process from the aim arising from clinical practice and throughout the study. 22 ID offers the possibility to include theory along the way, and interpretive authority was supported by including Antonovsky inductively. 14 The salutogenetic concept was in line with the aim of this study. 14
Analytic logic was supported through the step-by-step analysis, an iterative process through which themes and subthemes are defined. 22 The transparency of the process is visualized in Table 3 and Figure 2. Throughout the analysis process, the authors paid constant attention to the fact that clinical experience might influence interpretation. The first author’s position 13 as an experienced clinician working with DMD and having a preunderstanding and in-depth knowledge about the diagnosis was considered a strength, which led to confidentiality and understanding between participant and interviewer. Possible limitations could be preconceptions and potential blind spots.
The strength of the study was the patient involvement to inspire and guide the process. The feedback was very useful to clarify the invitation and interview guide.
Reflections and perspectives from this study could be relevant for people living with other neuromuscular or life-threatening diseases. There is a need for further studies to investigate relevant methods for healthcare professionals to initiate conversations about wishes and needs for future care.
Conclusion
This study provided new insights into reflections on wishes and needs of adults living with DMD. Navigating life with DMD was considered a condition of life, and being able to accept and adapt to uncertainties were effective coping mechanisms affecting the participants overall SOC. Furthermore, living with a life-threatening disease was managed by living one day at a time, finding solutions, taking life as it comes, and getting the best out of it. Also, having dreams like everybody else despite the uncertain future was important. Finally, talking about future care felt strange to the participants but was easier if someone dared to ask directly, however timing and addressing individual needs were essential.
The findings clearly indicate that future rehabilitation should include mental and existential issues and not be limited to issues concerning physical limitations. Healthcare professionals are recommended to initiate regular contact with adults with DMD and ask about their wishes and needs for the future. Healthcare professionals must be attentive to timing and have the courage to initiate conversation when the patient signal readiness to talk. Asking about death and dying is difficult for both healthcare professionals and relatives, but the present study shows that men with DMD are willing to share their thoughts even though it is difficult. To support healthcare professionals to initiate conversations, a systematic way of initiating and facilitating conversations is recommended, maybe in the form of a short interview guide. Palliative rehabilitation interventions are recommended which are tailored to the physical, mental and existential wishes, and needs of the person.
Footnotes
Acknowledgements
We would like to thank the participants for openly sharing their thoughts and making this study possible.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. According to the Central Denmark Committee on Health Research Ethics, the study could be conducted without approval from the Committee [Request no. 1-10-72-103-24].
Consent to participate
All participants were informed about the study orally and in writing and written or oral consent was obtained from all participants. The participants were guaranteed anonymity and could withdraw their consent at any time.
Consent for publication
Informed consent for publication was obtained from the participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data that supports the findings are available on request from the authors. Data is not publicly available due to the containing information that could compromise the privacy of the participants.