
Abstract
Introduction:
Bereavement affects individuals in diverse ways, and the support they require can vary significantly. For grief to be effectively recognised and addressed in both clinical and research settings, appropriate and validated assessment tools are essential. However, there is a notable gap in child-specific tools, particularly those that use non-verbal approaches to support young children and individuals with Special Educational Needs (SEN), who may have limited verbal communication.
Aims:
This scoping review aims to explore and map existing evidence on grief and mental health assessment tools that incorporate non-verbal methods. The focus is on tools used with children aged 11 and under, and with older children or adults who have additional learning or communication needs, in therapeutic and research contexts.
Methods:
We conducted a scoping review using Arksey and O’Malley’s five-stage framework. Searches were carried out across five databases – CINAHL, Medline, PsycINFO, Cochrane Library and Scopus – from their inception to 7 December 2023. Data from eligible studies were analysed using descriptive statistics and content analysis.
Findings:
From 1498 screened papers, 22 articles were included. Most described mental health tools rather than grief-specific assessments. Five key themes emerged: tool development processes; language and item selection; use of visual imagery; response format design and psychometric properties, including feasibility and utility. These features illustrate how non-verbal methods can support communication and engagement in assessment.
Conclusion:
This review highlights current approaches to assessing grief and mental health in children and individuals with SEN using combinations of verbal and non-verbal methods. It provides a foundation for future development of accessible, structured grief assessment tools tailored to these populations and underscores the urgent need for such resources in practice.
Plain language summary
This scoping review examined the existing research on therapeutic and support tools that use non-verbal methods to engage with and assess the grief and mental health needs of young people, particularly those with special educational needs (SEN). The review identified 22 relevant articles, which we analyzed and identified five main themes: these were, (1) the development of these tools and approaches, (2) how the tools work using key verbal and non-verbal features, (3) the use of visual representation and imagery, (4) the response options available, and (5) the effectiveness and performance of the tools. The review found that there is a lack of accessible, structured grief assessment tools that use non-verbal methods for bereaved young children and those with SEN. The findings provide an evidence base for further developments in this field, highlighting the need for more research and the creation of such tools to better support these populations.
Keywords
Introduction
The need for formal assessment and screening practices to determine need and appropriate levels of support-provision in bereavement policy and practice is growing in recognition.1,2 A variety of tools are available to assess grief and bereavement support needs in adults, 3 with many also used as outcome measures for evaluating interventions and services. 4 Grief measures should be used for the same purposes when supporting bereaved children and young people, but must sensitively reflect differences in child grieving (including developmental shifts in the meanings of loss 5 ), language abilities and comprehension, significant life relationships and social contexts (e.g. parental, school/education systems).6,7 Given the more limited language abilities of younger children and those with Special Educational Needs (SEN), and the fact that many children lack the words to express what they mean when it comes to talking about a death or traumatic experience6,8 approaches which use non-verbal methods to assess and explore child grief are also needed.8–10
Two recent systematic reviews have investigated grief instruments used with children and adolescents, confirming the absence of and need for more accessible child grief tools. Zhang et al. 11 identified a total of 24 grief assessment tools, clustered into three categories: general-purpose grief scales (n = 9), maladaptive grief reactions scales (n = 13) and specialised grief scales (n = 2). Ennis et al. 12 focused on tools used to assess maladaptive grief in children following traumatic loss, identifying 17 measures, in addition to various adaptations and variations of these measures. Many of these measures were directly adapted from adult measures with minimal testing of face and content validity, raising questions over their age and developmental appropriateness.11,12 Most were designed for and validated with older children (e.g. 8+), and all are reliant on verbal or written communication exchange, making them difficult to use with those with limited means of verbal communication or who are too young to express their feelings verbally. For some of the tools, lengthy administration times due to a large number of items likely also limits their suitability for use with younger children. 11 Similar problems have been reported in the wider field of mental health assessment in children. 13
Although not reflected in available child grief tools, a variety of alternative non-verbal approaches have been used therapeutically and in research with children with mental health problems and/or who have had traumatic experiences, including bereavement. 14 In mental health research/practice, the use of pictures and images in stories, questionnaires and interviews has been shown to provide a means of engaging with children, with pictorial formats assisting comprehension and the interest and focus of children, whilst also avoiding over-reliance on the vocabulary of the child. 15 Play therapy – including sand play and puppet therapy – has also been shown to effectively engage children, whilst offering insight into their experiences and feelings. Within these approaches ‘play’ is recognised as a form of language, and a meaningful way for children to explore and express their experiences and emotions, often using objects/mediums such as sand, puppets and toys/figures to project or convey difficult experiences and feelings.10,14,16,17 Likewise, art therapy, involving drawing and other forms of visual image-making, is used to help children access their feelings and give meaning to experiences that cannot easily be expressed in words.8,18,19
Responding to this need for accessible child grief tools, we are developing a pictorial version of the Children’s Attitude to Grief (CAG) Scale for use with younger children and older children with SEN. 20 Like the original Adult Attitude to Grief Scale, 21 the CAG is used both as a psychometric measure of vulnerability in bereavement – based on the interacting concepts of overwhelm/control/resilience in the Range of Response to Loss model of grief, 22 rather than a list of symptoms and a therapeutic conversational tool for qualitatively exploring client grief. We conducted this scoping review to better understand the key methodological components and features of tools/approaches which assess or explore grief, mental health and well-being using non-verbal methods. While directly informing the design of our own tool, this descriptive, systematically conducted review will also be helpful for other researchers and practitioners interested in designing and/or selecting similar research and assessment tools for children and adults with limited verbal communication in these fields of research and practice.
Methods
The review aimed to identify and map the key methodological components and features of clinical and research tools or interviews which assess or explore grief, mental health and well-being using non-verbal methods with children (aged 11 and under) and young people/adults with additional learning or communication needs.
The reporting of this review conforms to the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines for scoping reviews (Table A1). 23 The protocol for the scoping review was published on the public Open Science Framework platform on 09 May 2024 and can be accessed at https://doi.org/10.17605/OSF.IO/UB7ZC.
The review objectives were to:
Map available clinical and research tools/approaches which use non-verbal methods to assess and/or explore grief, mental health and well-being, and the related concepts of quality of life and coping/resilience in young children and people with SEN or other communication needs.
Identify and describe the key methodological components and features of these tools/approaches.
Assess the evidence on the performance, feasibility and acceptability of these tools/approaches.
Review design
A scoping review methodology was selected as our aim was to establish an overview of the current evidence base related to the topic (in this case ‘tools’) of interest. 24 The review followed Arksey and O’Malley’s 25 rigorous and transparent five-stage framework, as updated by Levac et al., 26 to enable replication of the search strategy and increasing the reliability of the review findings. The five stages involve; (1) identifying the initial research questions, (2) identifying relevant studies, (3) study selection, (4) charting the data and (5) collating, summarising and reporting the results.
Identifying the research question
The following research question was identified for this review; What are the key methodological components and features of clinical and research tools or interviews which assess or explore grief, mental health and wellbeing using non-verbal methods with children and young people/adults with additional learning or communication needs?
This question was underpinned by the PCC (population, concept, context) framework. 27 The PCC framework is recommended as a guide to create clear and meaningful objectives and eligibility criteria for a scoping review. See Table 1 for PCC framework developed to refine the research question and determine search terms.
PCC framework.

SEN: Special Educational Needs.
Search terms
Based on Medical Subject Heading (MeSH) terms and a set of key words, a preliminary search in Medline and Cumulative Index to Nursing and Allied Health (CINAHL) was conducted to identify articles on the topic. The keywords identified in the titles and abstracts of relevant articles, along with the MeSH terms used to index them, were utilised to develop the full search strategy by the study team (N.H.K., S.G., E.H.), with input from the wider team and the Public Involvement Youth Group. Three sets of terms were developed and combined according to the population (e.g. children, people with additional learning or communication needs), the ‘condition’/‘treatment’ (e.g. grief, mental health, therapy, counselling) and terms relating to non-verbal assessment methods (e.g. picture, pictorial, smiley, questionnaire, interview, measure). See Table A2 for the Medline search strategy.
Identifying relevant studies
A broad search was performed across a wide range of databases. CINAHL via Ebsco, Medline via Ovid, PsycINFO via Ovid, Cochrane Library (CDSR and CENTRAL) and Scopus, for studies published from inception of the databases to 7 December 2023. The archives of the key journal ‘Bereavement’ were also hand searched back to 2018, as the journal is not indexed in these databases. After the systematic searches, the reference lists of included papers in this review were scanned for potential articles. Experts working in the field were consulted to identify any potential sources that may have been missed in the searches. All references identified from the database search were uploaded to reference manager software (EndNote, version X20.6) 28 and screened by one reviewer (M.M.) to remove duplicate records. The final deduplicated EndNote library containing (n = 1498) unique articles were imported into the systematic review management platform Rayyan. 29
Selecting the studies to be included
The eligibility criteria for inclusion of papers were:
Reports of empirical studies of tools/questionnaires or interviews used clinically and/or in research to assess/explore grief OR mental health and well-being OR resilience/coping OR Quality of Life using methods which were not wholly verbal (e.g. questionnaires which involved pictorial representations of concepts/items).
Study participants were children of UK primary school age and below (11 and under); and/or young people and adults with Special Education Needs (SEN); and/or people (adults, children, young people and adolescents) experiencing language/communication barriers due to other reasons (e.g. non-native speakers/migration background/low-literacy levels).
Exclusion criteria were studies of tools which did not involve any form of non-verbal communication of the concepts/feelings being explored, or that were used exclusively with children above primary school age, and/or young people/adults without SEN or other language barriers.
Additional exclusion criteria that were applied included studies of measures specific to a condition or context, where the context/condition was not relevant to the focus of the review (e.g. pre-operative anxiety, quality of life (QOL) in relation to specific illnesses). Book chapters and conference abstracts were also excluded.
To select studies for inclusion, we used an iterative approach. N.H.K., E.H. and S.G. independently reviewed the titles and abstracts, followed by full-text screening. At all stages of the screening process, any disagreements between the reviewers were resolved through discussion, and when necessary, by consulting a third reviewer. A record of decisions was kept on Rayyan. To facilitate calibration, the team met during the process, with the first meeting focused on creating a shared understanding of the criteria and later meetings focused on comparing selected citations and discussing any discrepancies. The PRISMA diagram (Figure 1) reports the different stages of article selection. Studies that had used a relevant tool (e.g. as an outcome measure) but were not reporting empirical findings relating to the development or evaluation of the tool were initially retained at full-text screening and details of the tool extracted. The validation study for the tool (if not already included) was then retrieved and screened for inclusion. In total, 22 studies were eligible to be included in the review.
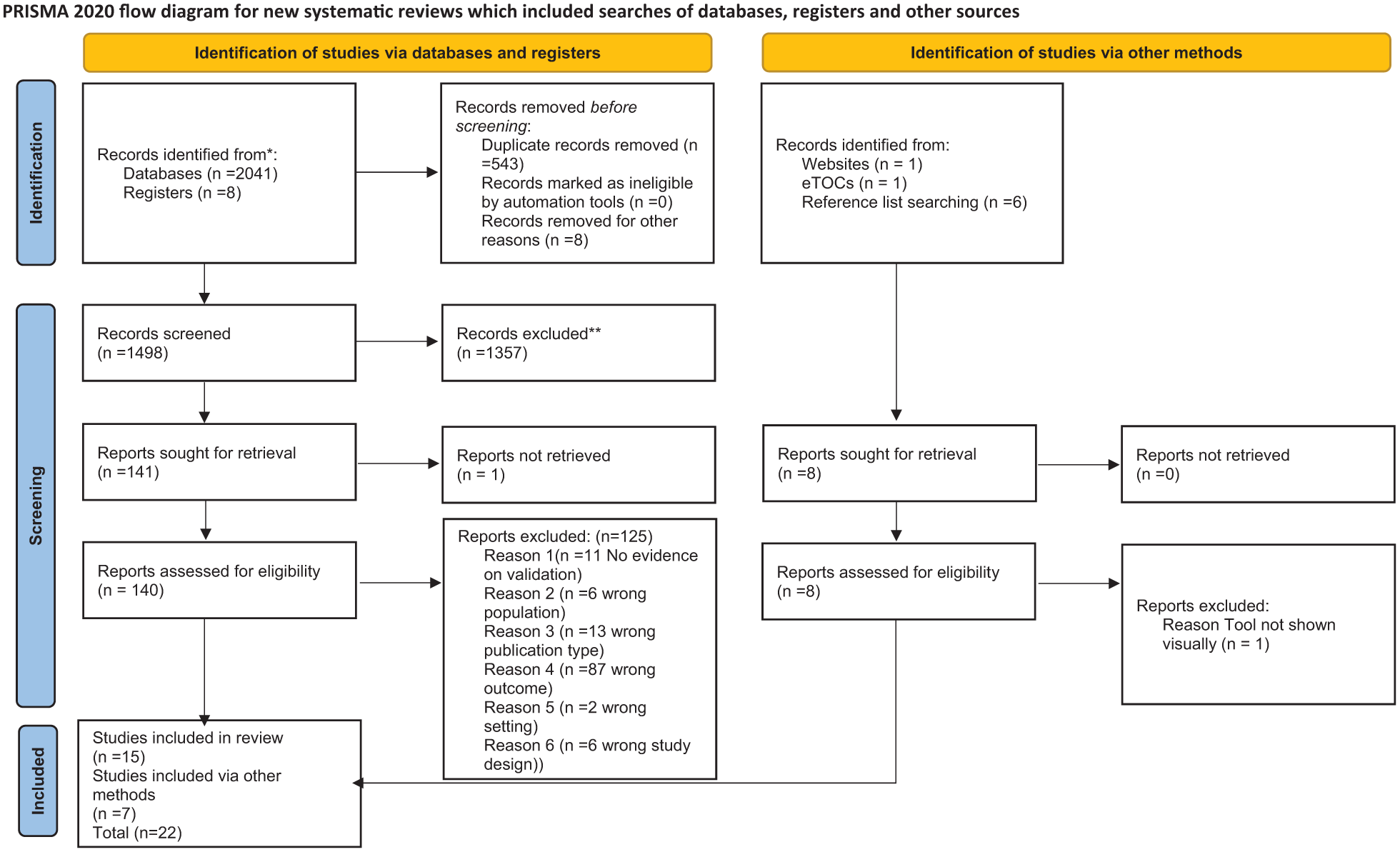
PRISMA diagram.
Charting the data
The data extraction template (see Table A3) was developed by the study team in Microsoft Excel and included specific details relating to the participants, concept, context, study methods, type of tool and description of tool, including key methodological components and findings relating to the tool’s psychometric properties, utility and feasibility.
N.H.K. and E.H. piloted the data extraction template, which was modified based on the pilot and then used to extract data from the included studies. Data were extracted independently, checked by a second reviewer for consistency and accuracy and, where required, disagreements resolved through discussion. Authors of one paper were contacted to request additional information. Five further papers were identified from searching references within the 17 articles. The quality of the studies was not evaluated as this is not necessary for the purpose of a scoping review which aims to map/describe the evidence.24,25,31
Analysis
Analysis of the articles involved a two-stage approach27,31: first, a descriptive statistical analysis to quantify included sources, publication types, years of publication and theme frequency across sources; second, a basic content analysis of the data extracted from the 22 articles. The analysis was undertaken by N.H.K. and E.H. and followed a rigorous and systematic six-stage approach, 32 outlined in Figure 2.

Approach to analysis.
Broad initial codes were applied to reflect categories of interest relating to the research question which served to guide an inductive approach to coding. Development of the coding framework was continually checked in relation to the original source of data and the scoping review question. Interpretation of analysis was also checked against the original documents, data extraction templates and the researchers’ notes. 33 Five themes were identified in the analysis of the articles: (1) Development of tools and approaches; (2) Language used and items included; (3) Visual representations and imagery; (4) Response options; (5) Psychometric properties, utility and feasibility.
Results
Study characteristics
Twenty-two articles were included in the review. Of these, most were quantitative validation studies of assessment tools or measures (n = 15),13,34–47 with five of these studies also reporting the measure’s development.13,36–38,45 Two were qualitative development/validation studies,14,48 three were observational studies49–51 and two were intervention studies that used a relevant measure in a pre-post study design and reported evaluation data relating to the measure.52,53 Studies were carried out in 14 countries, most commonly the United States (n = 5),35,37,40,42,51 the United Kingdom (n = 3)34,36,43 and Canada (n = 2).45,46
Table 2 provides an overview of the articles, the approaches identified in the article, the purpose of the measure, key features of the measure, aim of the study, key findings relating to the psychometric properties or use of the measure in observational/interventional contexts, and key features of development/validation where given. A summary of key considerations for design and implementation has also been included in the table to reflect the learning identified via our analysis. A separate table reporting the detailed statistical results of the included psychometric validation studies is included as Supplemental File 1.
Summary of papers included in the review.

HADS: Hospital Anxiety and Depression Scale; CoRG: Collaborative Research Group; ID: intellectual disabilities; PSC: Paediatric Symptom Checklist; CBCL: Child Behaviour Checklist; ICC: interclass correlations; MBSR: mindfulness-based stress reduction; PWI-ID: Personal Wellbeing Index–Intellectual Disability.
Measure characteristics: Conditions and populations being assessed
A total of 21 different measures/tools were identified across the 22 included studies. Measures assessed mental health (n = 10),13,35–37,39–41,45–47,52,53 depressive symptoms (n = 1), 42 trauma (n = 2),44,49 anxiety (n = 1), 48 stress/coping (n = 2),51,52 mood (n = 1), 34 emotional states (n = 1), 50 quality of life (n = 2)38,43 and grief or collective grief (n = 2).14,49 Eight of the measures were new measures,13,34,37,42,45,48,50,52 11 were adaptations of existing child measures31,35,39,46,47 or measures originally used to assess a different condition or population group.36,38,40,41,43,44,49 A further three studies reported on novel non-verbal approaches to enhance and facilitate communication during research interviews14,51 or in a therapeutic context. 53
The measures were designed to be used with a variety of population groups. These included children ranging in ages from between 3 and 16 years,13,35,37,39,42,44–47,49,53 children with autism, 48 children/adolescents with psychiatric disorders, 50 parents with low-literacy levels,40,41 people with learning disabilities,36,43,52 adults with hearing loss and intellectual disabilities, 38 adults with aphasia following stroke, 34 siblings of children with cancer 51 and bereaved children. 14
Developing the measures
Varied approaches were taken in the development (or adaptation) of the different measures. These included interviews and observations,13,14,48 focus groups13,36 and consultation/collaboration with a range of professionals (e.g. teachers, clinical professionals, support workers), parents, children and/or the learning disability (LD) community.13,36–38,40,42,43,45,48
These consultative processes commonly led to a reduction of questions and/or item selection,13,37,43 simplification of language to meet the needs of the population group,13,36,38 development of pictures to illustrate questionnaire items or constructs (e.g. mental health symptoms),40,41 visual representations of pictorial characters (of different gender, ethnicity, etc.) and general imagery.13,35,42,45 The number of options given in response rating scales were also sometimes reduced.36,43 Early piloting of measures was helpful in highlighting what wasn’t possible/appropriate (e.g. computer-based self-administration in adults with LD and hearing loss 38 ; classroom administration of a questionnaire with very young or autistic children 13 ). These specific adaptations and methodological features of the different approaches are discussed below.
Language used and items included
A variety of approaches were used to develop the questionnaire items, with the aim of ensuring that question construction was suitable for their target populations. This included evaluation of a pre-existing measure that informed adaptations, 36 focus group discussions that informed each iteration, 13 consultation with parents and teachers to choose scenario-specific questions 48 and collaborations with specific groups, such as healthcare professionals alongside a graphic designer 40 and adults with LD. 36 Piloting and seeking feedback on the suitability and feasibility of questions was also undertaken with individuals with LD. 38 These activities typically led to modifications in language to improve accessibility, particularly where the tool was an adaptation (i.e. from CORE-OM to CORE-LD 36 and MANS-LD to Mini-MANS LD 43 ) and a reduction of questions/pictures/items to be included in the measure.13,36,37,45
The number of items varied greatly across the different measures, reflecting the diversity in purpose and scope of the different approaches. These ranged from shorter measures with between 1 and 15 items13,34,36,38,43,48,50,52 to multidimensional pictorial questionnaires with between 97 and 137 items.35,37,39,40,45–47 The items were delivered in a variety of ways that ranged from first person ‘I’ statements, for example, ‘I can tell someone how I feel’, 13 direct questions about themselves, for example, ‘Have you bottled up angry feelings?’35–37,42 and third person approaches that ask whether they act/feel like a depicted character.35,37,39,45–47
Semi-projective measures (where realistic, familiar pictures or objects are presented to children to explore issues that may not be accessible via projective approaches) and wholly/fully projective approaches (where children used drawings to convey their thoughts and feelings) were used in five studies. These usually used a small number of ‘open-ended’ questions to elicit responses,44,49 with sand trays, pictures, drawing and puppetry also used to qualitatively explore views and experiences.14,49,51,53 The semi-projective approaches were considered to be a less confrontational and direct way of dealing with sensitive topics, 14 to engage children’s interest, cooperation and motivation, whilst minimising anxiety. 49 More detailed examples of these approaches are provided in Table 3.
Semi-projective techniques exploring grief and coping with family illness.

Visual representations and imagery
All 22 articles reported on the way in which imagery was used in the measure (or administration of it) and why. Imagery was commonly used to support understanding and give context to the question,13,37,48,49 to act as a tangible visual aid,14,38,51 to provide a resource for communicating a response,34,37,43,48 to give an accessible way to deliver the question itself37,40,41,45 and to complement other modes of communication, such as questions being read aloud, which were used to help reduce ambiguity in the images that the children were focusing on.46,47
Different approaches were used to develop the imagery. In two studies, children were asked to interpret and explain preliminary selections of pictures, with their comments used to inform modifications or the removal of images.37,45 Other approaches included consultation with colleagues who were familiar with a specific, longer version of the tool, 36 collaborative exercises between children, professionals and a cartoonist to create the pictures, 13 and a collaboration between a professional illustrator and adults with LD. 38
Pictures/symbols in cartoon form were most commonly used to illustrate questions, ,13,35–37,39–42,45–47,49 with photographs used in three measures.34,43,48 Examples included pictures depicting children expressing possible responses to a scenario (e.g. crying, hiding), 48 adults portrayed in different scenarios which were illustrative of the question and response options, 43 and variations of a face changing from sad to happy. 34 Additional mediums were also sometimes used to support the visuals such as computer assisted/video approaches34,39,47,48 and sign language. 38 Tangible mediums of sand trays/sand tray figures 14 and puppetry 51 were used in interview-style approaches to support children telling stories via an entity separate from themselves (i.e. the puppet or figure). One therapeutic approach also used dolls and puppets to introduce therapeutic concepts to children. 53 Drawing was also used in the one wholly projective measure that was included. This required responses to be given in the form of freehand drawings of a house, a tree and a person which were then quantitatively scored using a scoring key. 44
Imagery took various forms including cartoons of people that were to some degree relatable (cultural, gender, ethnicity, etc.),13,35–37,49 cartoons that were intentionally ‘gender ambiguous’45,46 or could be changed to match gender,39,47,49 or symbolic representations such as smileys and tick/cross options.36,43
Response options
A variety of response options were used in the measures. These included choices of simple, binary ‘Yes/No’ answers,35,37,39,45–47 selections of pictures which represented different response options,42,48 Visual Analogue Scales that require the user to choose a point on a visual scale13,36–38,40,41,43,50,52 and open-ended responses (requiring evaluation via thematic analysis 14 or content analysis48,51). Rating scales were also commonly used,13,36–38,40,41,43,52 mostly comprising 3 or 5 points, with the exception of one 7-point scale. 50 Following community consultation, it was notable that one adapted measure moved from a 5 to 3 point scale, to ensure feasibility and accessibility for the target LD population. 36
Across the measures there were multiple images or objects used to help users understand and communicate their response. These ranged from object representations, for example, beakers depicting frequency of feelings (an empty beaker representing ‘not at all’, half-full beaker for ‘sometimes’ and a full beaker for ‘a lot’), 36 and cartoon characters depicting three different frequencies of a symptom (‘never’, ‘sometimes’, ‘often’), 41 or arms shown at different widths to represent ‘how much’. 37 The European Health Interview Surveys–Quality of Life (EUROHIS-QOL BSL) incorporated an additional experimental approach in the form of a ‘light response’ (an animated lightbulb) that could be adjusted (in brightness) to communicate the users perceptions of their QOL. 38 Smiley faces 38 and situation-specific questions that incorporated a choice of responses/behaviours in picture form were also used.42,48 The tangible mediums of sand trays and drawing represented alternative forms of response, alongside the talk of participants.14,44
Psychometric properties, utility and feasibility
Most of the included studies evaluated at least some of the psychometric properties of the measures. This commonly included establishing test-retest reliability13,35,36,38,40–42,45,46 and/or internal consistency13,34–37,39,42–45,49 with most findings within the range of acceptable to very good. A small number of studies carried out either exploratory13,44 or confirmatory 39 factor analyses to examine the underlying factor structure of measures. For some measures, convergent validity was confirmed through correlation with related instruments34,38,43 while criterion validity against clinical judgement was also demonstrated. 45 The ability to discriminate between community and clinical samples when comparing example mean scores or prevalence estimates13,40,45,47 was also tested for some measures, with two studies reporting data on the sensitivity and specificity of measures based on suggested cut-off points.13,41
Two studies directly compared the psychometric properties of a measure’s pictorial adaptation with the original tool, confirming equivalence/comparability.40,41 A further three studies explored correlations between self-report measures and proxy measures from others. Two studies found poor agreement between pictorial self-report tools and proxy measures obtained from parents and/or teachers,35,42 while a third study reported mixed results for the agreement between the adapted sign language based self-report tool and proxy measures from professional carers. 38 A fourth qualitative study also found high levels of disagreement between child- and parent-identified coping strategies. 51 Four studies demonstrated measures’ ability to detect change over time, such as pre- versus post-intervention36,37,52,53 or current versus retrospective ratings. 50
Qualitative evaluations provided evidence for the utility and feasibility of the measure(s) in practice. Visuals were seen to provide helpful context and aid participants’ understandings of questions,41,48 as well as aiding information processing and engagement.14,35,37,45,48 Projective or semi-projective techniques were also seen as enabling the participant to speak about their experience in the third person (through the character).44,49,51 Feedback from parents/clinicians anecdotally indicated the acceptability of measures, including the relatability of the imagery used (incorporation of different genders, ethnicities and cultures).13,35,39,47 Other findings relating to implementation included the potential need for repeated administration of a measure to familiarise the user with the process, aiding cognitive ability and the potential for engagement (for adults with LD). 38
Limitations relating to accessibility were noted in three studies; firstly in relation to children needing greater support and direction than is possible in the intended group setting (e.g. very young children and those with autism). 13 Secondly where younger children (under 5 years) may not possess the ability to comply with the verbal instructions on the questionnaire, 37 or thirdly and similarly have the degree of verbal ability needed to engage with the interview process and not become engrossed in the play element of the sand trays. 14
Discussion
This scoping review has mapped the evidence for clinical and research tools or interviews which use non-verbal methods to communicate with young children or people with additional learning or communication needs, for the purposes of assessing or supporting their grief, mental health or well-being. While the review confirms the absence of accessible (non-verbal) child grief tools, 21 relevant measures or approaches were identified across predominantly mental health conditions, populations and settings. By systematically mapping and describing the methodological features of these tools and approaches, this review has provided a helpful evidence base for the design and development of our own accessible grief tool. The review findings will therefore also be useful for researchers planning similar endeavours, or for those interested in selecting suitable measures in these fields of research or clinical practice.
The key features of the different tools and approaches that we identified were categorised into four main themes which represent the different options and considerations available to researchers and clinicians interested in developing or selecting appropriate tools. These included; the collaborative processes involved in the development and adaptation of pictorial measures; the simplification of language, question and questionnaire structure (e.g. using direct or indirect questions); ways of incorporating visual representation, imagery and other mediums for facilitating understanding, identification and expression (including being relatable to specific or diverse groups of participants); and selecting accessible verbal and visual response options (e.g. using visual scales, binary responses or three point frequency/quantity scales).
This synthesis demonstrates the diverse ways that visual and other mediums can be used to support the delivery of an assessment tool or interview-style conversation, whilst also enabling more accessible response options. The positive evaluation results that were reported indicate the acceptability and effectiveness of these approaches for engaging with children and adults with learning or communication challenges when exploring sensitive topics such as grief and mental health, which can in themselves be difficult for children to discuss.6,14 They are also consistent with previous research and theory which has described the benefits of alternative non-verbal, projective/semi-projective approaches such as illustrated stories, art therapy and play therapy for supporting children experiencing bereavement, trauma or mental health problems,8,10,16–19 demonstrating how these traditionally non-directive therapeutic approaches can also be applied in more directive ways, incorporating verbal instructions, questioning and methods of analysis. The benefits of the collaborative approaches used to develop the images and question items in many of these studies13,36–38,40,42,43,45,48 also support the growing emphasis on community co-production and patient and public involvement in research, particularly when working with children or minoritised communities, whose perspectives, understandings and interpretations may significantly differ from those of research and clinical teams.54,55
Given our specific interest in grief, and the recognised importance of using validated assessment tools for determining level of need and appropriate intervention,1,6 the absence of accessible, structured child grief tools is notable, and consistent with other recent review findings which identified only fully verbal/written examples of child grief tools.11,12 Of the two grief related approaches that were included, one was focused on qualitatively exploring coping and collective grief and trauma following the assassination of the Israeli prime minister, 49 while the other used sand trays as part of a semi-structured interview to explore child grief experiences. 14 Although very different from each other (and the predominantly mental health tools considered in the review), both studies suggest the value of using visual imagery or sand tray figures to depict different social scenarios, combined with open-ended questions which encourage children to tell or show their story or feelings. Interestingly, both also provided the option of responding in the third or first person (i.e. speaking about themselves or projecting their thoughts onto the character in the picture or sand tray), with the benefits of these semi-projective approaches similarly described in the wider literature.8,10,16,17 Therefore, although the evidence for grief-specific tools is lacking, the common features of these approaches, alongside those from the majority ‘questionnaire’ based approaches used in mental health assessments, can provide a helpful and important steer to this underdeveloped area of research.
Limitations of this scoping review and implications for further research
The articles in this scoping review varied in their purpose, ranging from development and/or validation studies to observation and intervention studies. They focused on multiple areas of mental health and well-being and incorporated different styles of delivery and evaluation. This resulted in some inconsistencies in the detail available across the papers with notable gaps in some study reports. For example, very few studies validated new measures against other established measures or compared scores in community versus clinical samples, highlighting that some measures may benefit from more comprehensive and rigorous testing. However, as this was a scoping review focused primarily on mapping and describing available tools, we did not conduct a rigorous appraisal of the quality of the evidence for included measures, which limits the conclusions that can be drawn on their effectiveness. Future systematic reviews are needed to establish the effectiveness of these measures by appraising study quality and their psychometric properties, using recommended tools such as COSMIN checklists.56,57 In doing so, however, it will also be important to critically consider whether all components of these check lists can be reasonably applied to research developing these more accessible measures and whether any modifications of the checklists might also be needed going forwards. If possible, future reviews should also include book chapters and studies published in languages other than English. Due to resource constraints, this was not possible in this review but would likely have increased the yield of relevant approaches and studies for consideration.
Limitations in the utility and feasibility of measures were inconsistently reported across the included studies. Study limitations that were identified included lack of agreement between non-verbal self-report measures and proxy-report measures (obtained from parents)35,42 and the inappropriateness of tools or approaches for very young children.13,14,37 The older age ranges used in some of the other measures included in this review might also mean that they are not appropriate for those with the most limited verbal abilities. More research on the best methodological approaches for working with these specific populations clinically and in research would therefore be helpful, and could address the noted absence of research with bereaved young children and people with SEN.6,58
Finally, although the articles included are relevant to our field of interest, the absence of any validated grief measure or tool incorporating non-verbal communication methods strongly affirms the need for such tools, including the pictorial version of the Children’s Attitude to Grief Scale which we are currently developing. While there is a tradition of using creative methods in bereavement support (e.g. see archives of https://www.bereavementjournal.org/index.php/bcj), the absence of empirical data for these approaches meant that they could not be included in this review. These review findings therefore also point strongly to the need for greater evaluation and reporting of ‘non-verbal’ approaches which are being used to assess and support bereaved children and adults with additional needs.
Conclusion
The range of approaches covered in the review shows that there is likely ‘no one size fits all’ approach for engaging with young children and those with limited verbal abilities in research and practice. However, the common features, benefits and limitations that have been identified in the development, design and implementation of these tools or approaches provide helpful pointers for researchers or clinicians considering designing or selecting such measures for use in their research or practice. A context/condition/person centred approach in the development of measures (both novel and adapted versions) is essential, with the benefits of collaboration with children, parents and professionals well demonstrated across the studies. While all of the measures and approaches included in this review required some level of verbal interaction or instruction, they showed themselves to be accessible to diverse groups of people with more limited verbal communication, and who therefore seem likely to benefit from these hybrid (verbal and non-verbal) approaches. This review accordingly provides an encouraging foundation for further developments in this field.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251413281 – Supplemental material for Non-verbal methods for assessing grief and mental health in children and individuals with additional communication needs: A scoping review
Supplemental material, sj-docx-1-pcr-10.1177_26323524251413281 for Non-verbal methods for assessing grief and mental health in children and individuals with additional communication needs: A scoping review by Noreen Hopewell-Kelly, Silvia Goss, Mala Mann, Linda Machin, Timothy Pickles, Freya Field, Letizia Perna, Lucy Selman and Emily Harrop in Palliative Care and Social Practice
Footnotes
Appendix
Data extraction template used to extract information from included studies to answer the scoping review’s questions.

| Domain | Extracted information |
|---|---|
| Study characteristics | First author last name |
| Year of publication | |
| Country in which study was conducted | |
| Title of publication | |
| DOI of publication | |
| Study type | |
| Aim of study and methodology | |
| Population characteristics | Population |
| Age range | |
| Characteristics of non-verbal tool/approach | Condition (e.g. grief, mental health, wellbeing) |
| Name of tool/approach | |
| Type of tool/approach | |
| Description of tool/approach | |
| Key findings | Key evaluation findings (e.g. psychometric properties of tool/approach, including utility/feasibility) |
| Key findings in relation to development/design/implementation of tool/approach |
Acknowledgements
We would like to acknowledge the support given to the CAG study from the study advisory group and participants and staff at Winston’s Wish who have supported the wider study.
Ethical considerations
All papers included in the review reported on appropriate ethical clearance in their work. No further ethical considerations were required.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a philanthropic grant to Winston’s Wish. It was also supported by the Marie Curie core grant funding to the Marie Curie Research Centre, Cardiff University (grant number MCCC-FCO-11-C). E.H., S.G., M.M. are supported by this Marie Curie core grant funding (grant number MCCC-FCO-11-C).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.