
Abstract
Background:
People with dementia experience a gradual decline in cognitive and physical functioning, which makes the organization of end-of-life care in the right place challenging for them, their caregivers, and healthcare providers.
Objectives:
This study aims to understand the challenges of organizing end-of-life care for people with dementia in Latin America.
Design:
The study used a qualitative design.
Methods:
Two focus groups, one individual interview, and one dyadic interview were conducted with 15 stakeholders from 12 Latin American countries: Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, El Salvador, Guatemala, Mexico, Paraguay, Peru, and Uruguay. Thematic analysis was used to identify patterns within the data.
Results:
Although there were differences between and within the countries, end-of-life care was often affected by the socioeconomic contexts, which represent barriers for access to healthcare services; under-tapped informal caregivers’ potential; societal norms and cultural expectations around care and informal caregiving; the dementia-trajectory itself; and an inadequate assurance of policies, skilled workforce, and services.
Conclusion:
In Latin America, end-of-life care for people with dementia has many challenges for those directly affected, caregivers, and the wider healthcare system. Routes to improvement are needed to ensure that all people with dementia and their families can navigate the end-of-life process with adequate and equitable support.
Background
Dementia is a chronic, incurable condition characterized by a progressive decline in cognitive functions and behavioral changes that result in increased dependency. 1 It is one of the leading causes of serious health-related suffering and a burden on society and health systems that is expected to grow by 264% between 2016 and 2060. 2 Due to its increasing prevalence and burden on caregivers and healthcare systems, dementia is a public health priority.1,3
The prevalence of dementia in Latin America is higher than in other world regions. 3 It is estimated that in Latin America and the Caribbean, 4.5 million people were living with dementia in 2019, and around 13.7 million will live with dementia by 2050, nearly twice the projected increase for the United States and Canada. 3 Additionally, the mortality rate is estimated to be around 1.6–5.7 times higher in people with dementia than in those who do not have it. 4
Additionally, many factors may influence the provision of end-of-life care for people with dementia. The unpredictable trajectory, difficulties in communication, challenges in symptom assessment and management, and the high levels of dependency associated with advanced dementia complicate adequate end-of-life provision. In general, people dying from dementia receive poorer quality end-of-life care compared to patients dying from cancer, 5 and there is inadequate pain control, unnecessary interventions, and limited access to specialized palliative care services.6–8 These challenges are amplified in Latin America due to fragile healthcare systems, economic instability, deficiency in formal care facilities and training, gender stereotypes of care where caregivers are primarily women, significant socioeconomic disparities, 9 deficient healthcare infrastructure, persistent stigma, insufficient awareness, 10 as well as due to vast inequalities in access to palliative care and advance care planning. 11
Although an established framework of action for public health response to dementia exists, 12 there is still a wide disparity worldwide in its recognition as a public health priority that needs addressing. Some regions of the world, such as Africa, 13 lack national dementia plans, whereas others, including Europe, have had significant advancements in developing national dementia strategies. 14 In Latin America, only a few countries (Chile, Costa Rica, Cuba, Dominican Republic, and Mexico) have national dementia plans. 15 Of these, only the plans of Chile, 16 the Dominican Republic, 17 and Mexico 18 include palliative care.
Despite its importance, end-of-life care for people with dementia remains under-researched, particularly in low- and middle-income countries, where healthcare resources are limited, and the burden is higher.9–11 A recent study on the place of death in Latin America highlights significant variability in where people with dementia die, with hospital deaths accounting for 69% of cases in Brazil, while in Guatemala, only 4.7% of deaths occur in hospitals. 19 While patterns in where people with dementia die show significant variations, they provide little understanding of the challenges involved in organizing end-of-life care.
The research also has not fully addressed the challenges of providing end-of-life care for people with dementia or the circumstances surrounding their deaths. Therefore, a deeper understanding of how end-of-life care in dementia is organized across Latin America was deemed necessary. Thus, this research aimed to understand the challenges of organizing end-of-life care for people with dementia in Latin America. The main research questions were: (1) How is end-of-life care for people with dementia organized across 12 Latin American countries? and (2) What factors influence the provision of end-of-life care for people with dementia?
Methods
This research is part of the “Place of Death in Latin America” project, 20 which contains a database with death certificate data and statistical reports from 12 Spanish- and Portuguese-speaking countries in Latin America (Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, El Salvador, Guatemala, Mexico, Paraguay, Peru, and Uruguay). To better understand the variables that may influence the location of death in the region, a qualitative study was conducted to explore the organization of end-of-life care through the views and experiences of people involved in caring for individuals with dementia in these 12 countries.
We conducted two focus groups and, for those who could not participate in the focus groups, we conducted one individual interview with a health practitioner and one dyadic interview with a bereaved caregiver of a person with dementia and her accompanying physician. The results are reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplemental Appendix A). 21
Participant recruitment
We aimed to have at least one representative per country. We identified candidates through professional networks, websites, and social media from national dementia organizations for each included country, except for Paraguay, which does not have a National Association related to Dementia.
Purposive sampling was used to select different participants/informants involved with caring for people with dementia across diverse medical specialties or roles (psychiatry, geriatrics, primary care, palliative care, organization of patients/families, community volunteers, informal caregivers, and academics with relevant expertise). In total, 37 professionals from diverse fields and 18 national or regional dementia-related associations were contacted (Supplemental Appendix B) via email with an explanation of the study, relevant research articles,20,22 and a formal invitation to participate. Of the 55 sent emails, 12 agreed to participate, 1 professional referred us to a colleague in his country, and 1 suggested inviting a bereaved caregiver with whom he had worked before.
Data collection
Zoom links for two different time slots were provided to those interested in participating in an online virtual focus group. However, we accommodated the meetings according to the availability of the participants. Two of the authors (T.P. and P.H.A.) facilitated the groups and interviews in Spanish between November and December 2023. T.P. is a medical doctor and sociologist, and P.H.A. is a psychologist; they are both Latin American female researchers in palliative care with experience in qualitative research.
At the beginning of each meeting, participant consent was confirmed, and all participants provided verbal consent to record it. A brief introduction to the participants and the study’s goals was provided, followed by an opportunity for participants to ask questions. The discussion started with open-ended questions about the end of life and where people with dementia die as triggers.
After the initial discussion, quantitative statistical descriptive data on the place of death of people with dementia in the 12 countries 23 were presented as elicitation. Then, two additional trigger questions were asked: What factors may be influencing end-of-life care and the place of death of people with dementia in your country? And how could the provision of end-of-life care for people with dementia be improved? After these opening questions, the participants engaged in dynamic discussions about the end-of-life situation for people with dementia in their respective countries. The diverse participants’ experiences with dementia patients and carers were utilized to frame questions and encourage contrasting perspectives among participants, fostering a deeper and more nuanced exploration of the topics under discussion. All participants were given data from all countries, except for the caregiver and the physician from the dyadic interview, who were only provided with general information about the study.
Only the experts and the two facilitators were present during the meetings. All the meetings were audio-recorded. The facilitators took field notes and discussed them post-session. Audio recordings were transcribed verbatim using Whisper AI, an automatic speech recognition system. 24 PHA reviewed and corrected the 152 pages of transcripts against the original audio recording. Transcripts were not returned to participants for comment or correction. Finally, for this manuscript, anonymized quotations were translated into English.
Data analysis
Reflexive thematic analysis was used to identify, analyze, and report patterns within data. 25 A semantic approach was employed in the analytic process, which involves describing, organizing narratives, summarizing, and interpreting the data to theorize the significance, meanings, and implications of the themes, as well as the organization of end-of-life and influencing factors.
MAXQDA 26 was used to manage and conduct the analysis. Clear guidelines were established for using reflexive thematic analysis and its process. Disagreements were resolved through open discussion, where the codes and themes were checked against each other and then re-examined in relation to the original data set. The analysis was performed in Spanish, and the standard steps were followed 27 :
(1) P.H.A. and T.P. familiarized themselves with the data by repeatedly reading and jotting notes.
(2) An inductive process was used for code generation (open coding first, then axial and selective coding), which P.H.A. initially performed.
(3) Both researchers identified and compared subthemes, which were categorized into main themes through discussion.
(4) In scheduled work sessions, both researchers reviewed the themes and their connections.
(5) Defining and naming the themes was performed during virtual work sessions.
(6) P.H.A. prepared a narrative summary, which was iteratively reviewed and refined by T.P. and P.H.A.
Results
Participants
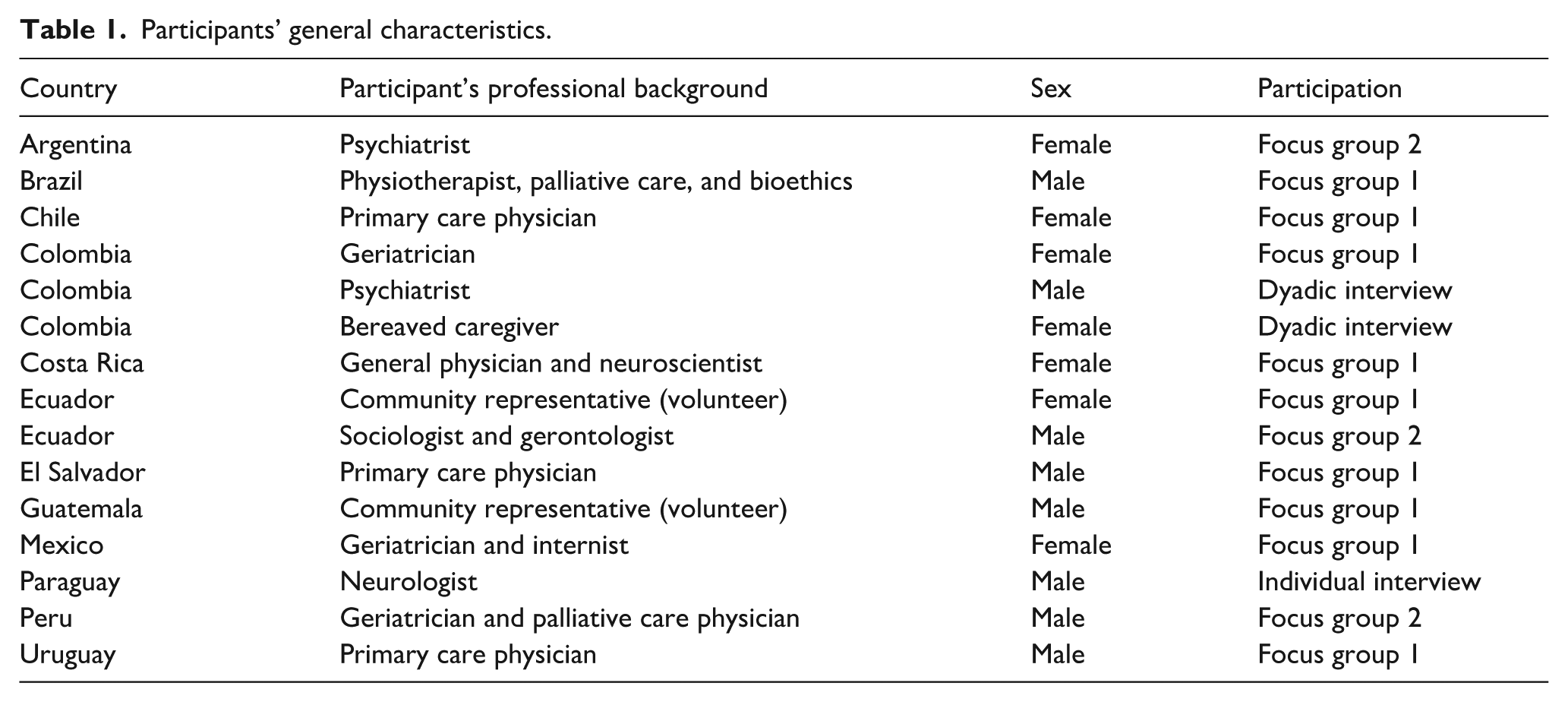
A total of 15 participants from all 12 included Latin American countries participated in the study. Twelve came from different professional disciplines, two were community representatives (volunteers), and one was a bereaved caregiver of someone with dementia, providing a broad perspective. Due to the availability of the participants, we held four online meetings ranging from 54 to 137 min. The first focus group lasted 137 min, the second focus group lasted 106 min, an individual interview lasted 54 min, and a dyadic interview involving a bereaved caregiver and the treating physician lasted 106 min. Table 1 details the participants' backgrounds and countries.
Participants’ general characteristics.
Themes and subthemes
The main topics discussed in the focus groups and interviews were categorized into five main themes of aspects influencing how and where end-of-life care in persons with dementia is organized: (1) socioeconomic contexts create important barriers for (equitable) access to healthcare services; (2) the potential of and support for informal caregivers is under-tapped; (3) societal norms and cultural expectations shape the practices and expectations around care and informal caregiving; (4) the dementia-trajectory itself presents challenges; and (5) inadequate assurance of policies, skilled workforce, and services for end-of-life dementia care limits options (see Table 2). However, it is essential to consider that all themes and subthemes were interconnected and influenced the end-of-life situation of people with dementia and their caregivers.
Themes and subthemes regarding the factors influencing end-of-life care organization for people with dementia in Latin America.

The bereaved caregiver confirmed the nuances of caring that the other participants mentioned in the focus groups. Additionally, country characteristics were shown to influence the conditions that affect the organization of end-of-life care for people with dementia. As a participant mentions, the variability among countries is so significant that “it can range from having such good and excellent services that people choose it, to having such horrible and deficient services that I will never be able to access anything other than dying at home” (Primary care physician from Uruguay).
Socioeconomic contexts create important barriers for (equitable) access to healthcare services
Economic and social determinants of health (subtheme)
Some Latin American countries face sociopolitical turbulence that directly affects all their inhabitants, regardless of their socioeconomic status. For example, at the time the caregiver from Colombia was taking care of her mother with dementia, there were social and violent outbreaks that “resulted in road closures and access difficulties. M.E [the caregiver] had trouble getting medications and services for her mother” (Psychiatrist from Colombia).
Moreover, individual contexts directly affect people with dementia and caregivers by influencing the economic and social determinants of health, such as education, healthcare access and quality, or access to care facilities and services that people can utilize at the end of life. When talking about where people with dementia die, our expert highlighted that “with a higher level of education, there are probably more resources, better social support, and many of these patients have [health] insurance [to allow hospitalizations]” (Geriatrician and palliative care physician from Peru).
Structural inequities (subtheme)
These types of inequity in the system also influence the end-of-life care. Participants noted significant differences in the resources available to the population between rural and urban areas. This is particularly relevant in countries such as Paraguay, where inequities persist as a significant issue regarding economic disparities and conditions, and in others, such as Uruguay, where access to health services is less determined by financial status but still influenced by resource allocation in certain areas. Our experts mentioned: “other [people] don’t die in the hospital because there isn’t one in their area” (Neurologist from Paraguay) and “In an area with around 600,000 people, there are two institutions with a capacity for about 100 people. So, in reality, the access is very, very, very limited” (Primary care physician from Chile).
The potential of and support for informal caregivers is under-tapped
Decision-making responsibilities (subtheme)
In most of Latin America, families are the primary caregivers, and the home is the principal place of care. Thus, many families assume full responsibility for care and joint decision-making responsibilities, frequently without adequate knowledge or support. This care responsibility becomes particularly complex in the absence of proper support systems. Caregivers also seek emotional and psychological support to navigate the uncertainty and doubt of all these challenging decisions.
Properly trained professionals can empower families to make informed decisions that align with patient preferences and needs. For example, our participant caregiver expressed the desire for more direct assistance from professionals: “(. . .) It would be really great if the doctor went to the house, attended to the patient, and also helped one resolve many doubts that fill you and worry you. ‘Am I doing this right?’ ‘Am I acting wrong?’” (Bereaved caregiver from Colombia)
Caregiving burdens (subtheme)
The lack of preparation and support, and the changing demands and complications of caregiving, added to the complex decision-making responsibilities, can lead to significant caregiving burdens, such as stress and emotional exhaustion. Throughout this (often long) trajectory, families may hire private formal caregivers if they have the financial means and if such caregivers are available. However, hired caregivers are frequently not trained to provide this care, which could also become burdensome. As the caregiver from Colombia narrated, I had nurses who stole from me, I mean, they stole in my house. So that’s also a risk for the whole family (. . .) instead of giving my mom her medication, they were taking it (. . .) these medications are sold on the black market, and that’s how they make some extra money. So, we had to start setting up a system to verify if she actually took the pills (. . .). We had to install cameras due to the thefts (. . .), we had to implement all of that to ensure she was given the medication, that she wasn’t mistreated, and that they didn’t leave her crying (. . .). (Bereaved caregiver from Colombia)
There are similarities across countries regarding the needs of both caregivers and people with dementia. Participants expressed concern about the limited options they may face due to the availability—or lack thereof—of resources. Participants also highlighted the high out-of-pocket costs for medical care, therapies, and equipment that, along with the disease trajectory, strain families financially, particularly in more deprived areas. As participants mention: “It has a lot to do with the healthcare system and the few possibilities of actually doing what people want, (. . .), but that’s because it relates to their economic conditions” (Geriatrician from Colombia) and “In Ecuador, the social system is very poor, (. . .), if you can pay privately, you can do so, but it’s very basic. People don’t have full access to private medicine, and getting an appointment through social security is very difficult” (Community representative [volunteer] from Ecuador).
Societal norms and cultural expectations shape the practices and expectations around care and informal caregiving
Cultural variations (subtheme)
These are also significant when understanding end-of-life care of people with dementia in Latin America. Elements such as religiosity, language, familial relations, and how people are seen and treated according to their age play a role in dementia care. For example, a participant mentioned that in Mexico, “sometimes the functional state of the person is not considered when making decisions; it’s just ageism that prevails. When someone is older, certain treatments may no longer be offered” (Geriatrician and internist from Mexico).
Societal expectations (subtheme)
The decision-making process of people with dementia and their caregivers about the place of care and the place of death is also influenced by societal expectations toward institutionalization, dementia, and death. Determining the preferences is often influenced by differences between people with dementia and their caregivers. For example, in Peru, close-knit family bonds are crucial in caregiving and determining the place of care and the place of death. However, while patients may prefer to die at home, family members may struggle to fulfill this wish due to emotional or logistical constraints: “People surely prefer to die at home. The family members, depending on how emotionally capable they are of accompanying someone to die at home, may have different preferences. Some might like it, and others might not” (Geriatrician from Colombia). Additionally, it is common not to talk about these topics because “the culture doesn’t allow us to address topics like death, even though the patient with dementia may still have much cognitive ability” (Primary care physician from El Salvador).
Participants’ interventions highlighted the emotional complexities and cultural differences surrounding caregiving and end-of-life decisions. These include preferences for home death, shaped by cultural values. An expert highlighted that in some Latin American cultures, caring for a loved one at home is seen as a moral responsibility and a demonstration of familial love and respect. On the other hand, guilt is often experienced when considering professional care settings, although this factor varies among countries. For example, an expert mentioned, “Argentine society is very blameful about this. So, leaving their family members in someone else’s care, at least speaking from my perspective as a psychiatrist, is a very. . . guilty, very painful experience” (Psychiatrist from Argentina).
A similar situation is present in Guatemala: The fact that the person dies outside of the home also implies that there are certain feelings of guilt within the family. So, they feel more at ease having them there [at home] because they don’t know how things will go when they’re away, as they won’t be able to visit them. Even in the public system, visits are very limited with strict hours; it’s not daily, it’s at certain times. There are a number of operational limitations that lead people to decide it’s better to keep the patients at home. (Community representative [volunteer] from Guatemala)
However, in Uruguay, the situation tends to change, There isn’t much guilt in institutionalizing patients. Once patients have advanced dementia, CLPMs [long-term care facilities for the elderly] are also a very commonly used resource. Both in my professional practice and among most of my colleagues, I believe we have a tendency to absolve families when the patient becomes very dependent, and the families become exhausted. In such cases, institutions are a resource, and they are used frequently. It’s not uncommon. (Primary care physician from Uruguay)
The dementia trajectory itself presents challenges
Dementia trajectory (subtheme)
Characteristics of the dementia-trajectory pose many challenges for individuals affected, their caregivers, and health systems alike, especially at the end of life. Participants highlighted the progression, fluctuation, timing, complexity, and incapacity to communicate that generate uncertainty and challenges in managing these patients at home. However, when delving into the place of death of someone with dementia, the hospital was not always considered the best setting: “Their [nurses’] support at times isn’t the most appropriate. I think they lack training in handling the human aspect—not to the one who’s sick, but to the one who’s there providing the support” (Bereaved caregiver from Colombia).
Our experts mentioned how medical complications, comorbidities, and direct causes of death can also influence the type of care required and decisions about care, and how comorbidities, such as respiratory and urinary tract infections or episodes of delirium, can compound the underlying condition.
In advanced stages, infections, pneumonia, and complications from pressure ulcers become frequent, alongside the natural progression of dementia. These lead to hospitalization needs in most cases. (Geriatrician and internist from Mexico). In most Alzheimer’s cases, it progresses more slowly, while vascular dementia sometimes has more. . . ups and downs, and this can determine hospitalizations. (Primary care physician from Uruguay)
These medical complications or “downs” depend on the stage of dementia and the trajectory of the types of dementia. Participants emphasized the inadequacies of in-home care without additional specialized support that may lead to suffering: “People find it very distressing to see their loved one die, choking, in the midst of pain, screams, and suffering” (Psychiatrist from Colombia). It was clear to our participants that people with dementia often require additional medical attention and, at times, hospitalizations: “When something happened to my mom, the only final solution I had, because I didn’t have a direct phone number, was to go to the emergency room” (Bereaved caregiver from Colombia).
The suffering of people with dementia (subtheme)
Besides, dementia, as a chronic, incurable, and progressive illness, involves existential and physical suffering of people with dementia. This could be due to many factors, such as cognitive decline, loss of abilities, independence, comorbidities such as fractures from falls, and treatments. However, given the characteristics of the illness, especially as communication becomes more challenging, caregivers and patients may struggle to understand and correctly address this suffering: “You find patients with benzodiazepines, with a very dangerous polypharmacy, and with a lot of existential suffering, because we know that in dementias (. . .) there is a point of tremendous suffering” (Psychiatrist from Argentina).
Inadequate assurance of policies, skilled workforce, and services for end-of-life dementia care limits options
Legal and policy frameworks (subtheme)
The characteristics of the healthcare system, along with its frameworks, play a crucial role in organizing end-of-life care. Despite variations across countries, common factors that affect end-of-life care include inadequate healthcare policies, system fragmentation, limited or lacking support structures, and low public awareness of these legal frameworks. These factors shape/affect how people can navigate those systems.
In Peru, for example, complications related to dying at home often lead families to opt for hospital death due to bureaucratic and medical challenges: While it’s true that fewer cases involve the family wanting and having the support for the patient to die at home, the vast majority tend to pass away in the hospital due to the need to provide the death certificate on time, complete the necessary paperwork, hold the wake, etc. (Geriatrician and palliative care physician from Peru)
Public awareness and education (subtheme)
The lack of Information is another barrier that “needs to be broken down, through psychoeducation, dissemination of data, and research, so that government services in their various forms, create policies” (Psychiatrist from Argentina). The information mentioned by the experts in this regard includes public awareness and education among both professionals and the general public. For example, in Colombia, there is a lack of knowledge of the existing law on advance directives; “therefore, families wouldn’t know what their loved one would want, or where they would want to die” (Geriatrician from Colombia).
Additionally, participants consistently emphasized the insufficient knowledge of healthcare providers about dementia progression, symptom management, and palliative care. This knowledge gap often leads to suboptimal guidance and care because “many [health professionals] don’t understand the needs of people with dementia, let alone how to address them in the advanced stage” (General physician and neuroscientist from Costa Rica). Thus, as our participants mentioned, people with dementia often receive aggressive medical interventions as they approach the end of life, increasing unnecessary treatments and interventions that add financial burdens for healthcare systems or out-of-pocket costs for families. For instance, prolonged hospitalizations, inappropriate medications, or invasive procedures may contribute little to the quality of life while significantly straining limited resources, suggesting an inadequate allocation of resources: During that hospitalization, they gave her platelets, they hydrated her because she was completely dehydrated, inserted a [nasogastric] tube because she wasn’t eating, and they used it to feed her. I think her potassium was low, so they raised it. I mean, all her signs, everything was wrong, and they started working on everything to try to stabilize her. (Bereaved Caregiver from Colombia).
On the other hand, education and training are seen as a source of empowerment. The participants suggested that the guidance provided by the medical team plays a crucial role in decision-making during dementia and end-of-life care. In many countries, proper guidance helps caregivers and patients during caregiving and helps them make fundamental decisions on time. For example, The clinic was responsible for training the [paid] caregivers. They trained us on how to change the bed to avoid harming the person and how to move her to another place. That was truly fortunate, and I think it was really good because it helped a lot during the process. (Bereaved caregiver from Colombia) The truth is that when they [the family] have contact with palliative care teams, they can decide to keep them at home because they receive guidance, the right care at home as it should be until the end. But they make that decision. However, it depends a lot on when they have contact with the palliative care team. (Primary care physician from El Salvador) The family may be scared and have little information about what they need to do. They might be terrified by the moment of death because they don’t know what to do or how to react. They don’t feel capable of taking care of their patient. But that fear disappears when they are provided with the necessary information and support. The family is given the tools to feel at peace. (Geriatrician and internist from Mexico)
Support and instruments provided by the healthcare system (subtheme)
Only sometimes is an expert team available to deliver guidance and information. In fact, the formal support and instruments provided by the healthcare system, such as programs, interventions, treatment equipment, tools, and the availability of palliative care, among others, are vital in helping this population. Our experts emphasized that healthcare systems must strengthen primary care to meet patients’ basic needs through primary-level care teams and identify those with complex needs, referring them to specialty care when necessary. As an expert explains: Expecting palliative care to be exclusively provided by specialized palliative care teams is impossible and unfeasible at the level of any country due to the number [of patients]. I think the key to making sure these patients can die at home, if they wish to, is to involve primary care in palliative care for patients with low-complexity needs. The advanced dementia patient, in general, faces complications like bedsores or some infections, but they typically reach the end of life with needs that are manageable by primary care teams—by a doctor or nurse with basic training. (Primary care physician from Uruguay)
Community involvement and informal support systems (subtheme)
Given the relevance of this additional help and the lack of official resources, participants highlighted the importance of community involvement and informal support systems in collaborating with the healthcare system. The participants stressed that the solution to caregiving issues goes beyond the official healthcare system and involves community support and state resources, such as housing and caregiver training. They also focused on the importance of addressing death and caregiving in community settings, especially by engaging primary health physicians and fostering conversations about care, illness, and death. In Colombia, for example, an expert explained that “many of us are doing campaigns, talking everywhere to the community and doctors about this [the law on advanced directives]” (Geriatrician from Colombia).
Discussion
Summary of main findings
The place of death of people with dementia in Latin America varies significantly across countries. 19 This study complements these quantitative data by offering a qualitative understanding of the challenges associated with organizing end-of-life care for individuals with dementia in 12 Latin American countries. It identified five main themes: (1) socioeconomic contexts create important barriers for (equitable) access to healthcare services; (2) the potential of and support for informal caregivers is under-tapped, (3) societal norms and cultural expectations shape the practices and expectations around care and informal caregiving, (4) the dementia-trajectory itself presents challenges, and (5) inadequate assurance of policies, skilled workforce, and services for end-of-life dementia care limits options.
Interpretation of main findings
Some of the identified challenges in this study share commonalities across the region, while other barriers may differ in each country. One of the shared challenges includes the influence of socioeconomic factors, social determinants of health, and structural inequities that create significant barriers to equitable access to healthcare services. Results indicate that these directly affected the caregivers’ burden and were crucial factors shaping healthcare access and end-of-life decisions. The complexity of addressing the socioeconomic contexts adds to the second shared challenge, the dementia-trajectory itself. The variability of severity and symptomatology increases the burdens that people with dementia and their caregivers experience in the emotional, physical, and psychological realms, and makes end-of-life care particularly difficult.
Other barriers identified by this study may have different implications in each country. Our analysis reveals that the potential of informal caregivers is underutilized, and there are considerable unmet needs among caregivers who often assume full responsibility for care and decision-making without adequate knowledge. Additionally, there is a pressing need to substantially strengthen both formal and informal support systems for people with dementia and their caregivers in each Latin American country. Community-driven initiatives and awareness-building efforts should involve, but do not rely solely on, government structures. This holistic, integrated approach aims to provide comprehensive support for families from the healthcare system and the broader social infrastructure. It includes the need to address societal attitudes toward dementia, death, and caregiving to normalize the topic and reduce stigma. 28 Other researchers have also emphasized the importance of normalizing discussions around these topics and increasing education about them. 29
Cultural aspects also impact healthcare access, advanced care planning, and end-of-life care and decisions, underscoring the importance of open communication and early involvement of patients and their families in end-of-life decision-making. 30 Our experts showed how some countries have cultural, health literacy, linguistic factors, and profound structural inequities that hinder healthcare access for people with dementia due to resource allocation, especially in rural areas. These findings support previous research in countries such as Peru, where low-income, rural, and Indigenous communities are unevenly impacted by public health disparities and underinsurance among older adults. 29
The results of this study align with research indicating that inadequate healthcare coverage, limited access to resources, cultural norms, and unstable political dynamics all influence a country’s ability to manage and overcome the burden of neurological diseases. 31 There have been advancements in the region to provide better care for people with dementia and their caregivers; however, there is still a significant lack of education among health professionals regarding dementia, end-of-life care, and the programs available for the population. For example, in Costa Rica and Colombia, although laws and programs are in place for elderly care, the lack of awareness about these resources creates a knowledge gap that hinders their proper utilization. This issue is worsened by the limited availability of support services, leaving people with dementia and their caregivers struggling to manage their needs without sufficient guidance. Additionally, previous research suggests that information sharing should not only occur within a country but also involve sharing data, best practices, and policy approaches on a regional and global scale. 32
Our study also suggests that the availability of professional support for caregivers and people with dementia needs to be increased in Latin America. A proper allocation of resources and the enhancement of education curricula are required to improve this support. Previous research also suggests specific strategies to integrate a palliative approach with dementia care in long-term care facilities that could also be applied to other settings; these include adopting a palliative approach, educating and training the workforce (including support workers and care aids), and adopting tools and policies that enhance care and support staff. 33 Other research also highlights that health disparities, scarce geriatrics training in medical schools, low awareness, and stigma about dementia affect care. 29 Adequate training of healthcare professionals in the care of individuals with dementia, including improved symptom management, avoidance of unnecessary interventions, and a focus on patient-centered care, as well as support and education for family members, is essential for reducing the burden on caregivers, enhancing patient outcomes, and lowering healthcare costs.
Beyond corroborating themes raised by professionals, the bereaved caregiver contributed unique first-person insights into the micro-practices of home care (e.g., monitoring medication, risks with untrained paid caregivers, resorting to surveillance to prevent theft), the need for validation and reassurance from clinicians, reliance on emergency departments when direct support was unavailable, and perceived deficits in the human dimension of hospital nursing care.
Strengths and limitations
This study employed focus groups and interviews, which facilitated an in-depth understanding of the explored themes. The qualitative analysis presented relies on the experiences of experts, caregivers, and professionals involved in dementia care from 12 different countries in Latin America. The comments and examples provided by the participants offered rich insights into end-of-life care for people with dementia, offering a deeper contextual understanding of the reality across most countries in the region. Although national and regional organizations were contacted to participate in this study, only one or two experts per country agreed to take part. Thus, a potential limitation is the characteristics of the participants (i.e., their area of expertise, the setting in which they work, and their own experiences in the field), which might bias their responses. Additionally, one should interpret the results with caution, as the findings may not reflect the perspectives of all Latin American countries, nor important stakeholders, such as representatives of healthcare systems, other professionals involved in caring for people with dementia, and caregivers.
Including a bereaved caregiver enriched the analysis with lived, operational details about day-to-day risk management at home, affective needs, and service-use workarounds, thereby sharpening implications for strategic improvement. The study did not consider direct input from people with dementia themselves, which could shed light on other perspectives and challenges particular to them, such as the management of other comorbidities, the stigma they might face, and the quality of support and the organization of care provided by the healthcare system, their family members, and their community.
Implications for policy and practice and suggestions for future research
The results of this study provide clinicians and policymakers with concrete examples of the needs and the many dementia-related challenges in Latin America. When planning policies and interventions for people with dementia, policymakers should consider structural inequality and socioeconomic context, which create barriers to healthcare access. They should also understand the cultural variations present within the country and consider the necessities of rural areas. Due to the complexity of dementia and its trajectory, a multi-stakeholder approach and collaboration are essential to develop evidence-based national plans that consider inequalities and societal norms and expectations.9,34 This approach should include financial and welfare assistance strategies, greater collaboration of multi-disciplinary teams, and advocacy for earlier detection and management strategies. 34
Clinicians should also consider the role of societal norms and the underutilized potential of informal caregivers in their contexts, and incorporate culturally informed open communication into their practice. This could support advanced care planning, which could alleviate burdensome treatment and provide certainty and clarity to medical and care providers, people with dementia, and their caregivers. 35 Future research analyzing subcultures and specific sociocultural and systemic dynamics would add more clarity and nuanced insights into each country’s situation. Additionally, longitudinal studies should be conducted because they can provide valuable insights into disease trajectories and associated needs over time, informing the development of more effective, and culturally sensitive policies and practices.
Last, given that inadequate assurance of policies, skilled workforce, and services for end-of-life dementia care limits options for patients and caregivers, healthcare policymakers and practitioners should consider international frameworks for dementia care, which emphasize the importance of awareness, early diagnosis, quality care, and creating dementia-inclusive communities, because they can facilitate the examination of systemic challenges and areas for improvement. 12 Future research should incorporate data from other Latin American countries to explore their characteristics and challenges regarding end-of-life care of people with dementia.
Conclusion
This study reveals that the provision of adequate end-of-life care for individuals with dementia and their caregivers in Latin America is marked by significant challenges and complexity. This complexity is shaped by a combination of cultural, geographic, economic, social, and dementia-specific factors. Specific issues, such as the cultural expectations around care and the challenges inherent to the course of dementia, may be more difficult to change through policies and interventions. However, other factors identified in this study are more amenable to change. They may need to be the attention points for end-of-life care policies and strategies across Latin America. These include ensuring an adequately skilled and diverse workforce for end-of-life care in dementia, empowering and investing in the strengthening of the enormous potential of family caregivers, and addressing significant structural disparities and inequities that impact end-of-life care for individuals with dementia. By identifying these potential routes to improvement, this study can guide countries in Latin America on how to ensure that all people with dementia and their families can navigate the end-of-life process with adequate medical and social support.
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251406286 – Supplemental material for End-of-life care of people with dementia in Latin America: A qualitative analysis
Supplemental material, sj-docx-2-pcr-10.1177_26323524251406286 for End-of-life care of people with dementia in Latin America: A qualitative analysis by Paula Hidalgo-Andrade, Luc Deliens, Joachim Cohen and Tania Pastrana in Palliative Care and Social Practice
Supplemental Material
sj-xlsx-1-pcr-10.1177_26323524251406286 – Supplemental material for End-of-life care of people with dementia in Latin America: A qualitative analysis
Supplemental material, sj-xlsx-1-pcr-10.1177_26323524251406286 for End-of-life care of people with dementia in Latin America: A qualitative analysis by Paula Hidalgo-Andrade, Luc Deliens, Joachim Cohen and Tania Pastrana in Palliative Care and Social Practice
Footnotes
Acknowledgements
We appreciate the time and collaboration of our participants, as well as the feedback received during the writing process of this manuscript from the members of the Bienestar, Salud y Sociedad Research Group.
Ethical considerations
The study was approved by the Ethics Committee of RWTH Aachen University (EK 206/19).
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by a scholarship awarded to the first author in the program “Research Stays for Academics and Scientists, 2023” of the German Academic Exchange Service (DAAD, ID: 57681226). The views and opinions expressed in this study are those of the authors and do not necessarily reflect the official policies or positions of the respective funding organizations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The qualitative data of this study are not publicly available due to privacy concerns and ethical considerations. Access to the data (excluding identifying information) may be granted upon reasonable request, subject to compliance with ethical guidelines and participant consent, by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.