
Abstract
Background:
The COVID-19 pandemic posed an unprecedented challenge for the healthcare system worldwide and led to high levels of psychosocial stress, particularly among nursing staff working in special COVID-19 wards. As previous studies have shown, this stress has had a profound impact on mental health, underscoring the need for further research to deepen our understanding of these effects.
Objectives:
To investigate the experiences of nursing staff working on special COVID-19 wards during the COVID-19 pandemic with regard to the death and dying of patients.
Methods:
To uncover aspects that might have remained unobserved in a quantitative survey, a qualitative research design was chosen for data collection. Using a semi-structured interview guide, we interviewed 14 nurses about their experiences. The data was then analysed using a qualitative content analysis according to Mayring.
Results:
Nursing staff were exposed to a particularly high level of stress. The reasons for this included the lack of opportunities for end-of-life care, patients dying alone, an above-average level of confrontation with death and serious disease progression and finally, limited treatment options and specialised care for deceased patients. These factors led to moral injuries.
Conclusion:
The results emphasise the urgency of better preparing nursing staff for future crises, providing psychosocial support and developing preventive strategies against moral distress. The promotion of resilience and the creation of conditions that prevent moral injury are essential to minimise the long-term effects of such stress and to protect the mental health of nursing staff in the long term.
Trial registration:
Registered in the German Register of Clinical Studies under the number DRKS00030425.
Introduction
According to the World Health Organisation (WHO), the impact of the COVID-19 pandemic on the mental health of the population is concerning. 1 The pandemic has posed considerable challenges not only to the private lives of many people around the world, but also to the healthcare system, leading to a high level of physical, mental and psychological stress for healthcare professionals. In particular, the pandemic had a significant negative impact on the mental health of nurses caring for COVID-19 patients, as shown by the increased prevalence of mental illness in this occupational group.2 –5 Many hospital and care facility staff reached their limits during the COVID-19 pandemic.
Previous experience with epidemics such as SARS in 2003 and Ebola in 2014 showed that healthcare workers in such situations are prone to post-traumatic stress symptoms, anxiety, depression and frustration.6,7 These findings have also been confirmed during the COVID-19 pandemic, particularly with regard to the moral and psychosocial stress experienced by caregivers working directly with COVID-19 patients. 8 To ensure appropriate care for all COVID-positive patients with severe symptoms, and to protect other non-COVID-19 patients, special wards for COVID-19 patients have been set up in many hospitals, which are referred to below as special COVID-19 wards. As these wards were not intensive care units, COVID-19 patients who did not require ventilation but were still seriously ill and in need of intensive care were accommodated and treated there. In very severe or even life-threatening cases that required more intensive monitoring and treatment and where a treatment goal could be set, the patients were transferred to the intensive care unit. Despite all these measures, many of the patients died in such COVID-19 wards. The care of dying and deceased COVID-19 patients, which is a central and important task for nursing staff, could often not be provided to the desired extent during the pandemic. This led to moral injuries for many nurses, which can have long-term effects on their mental health.
Against this background, it is of central importance to investigate the impact of the pandemic on the mental health of carers. Following a phenomenological approach, which focuses on understanding lived experiences, the aim of this study was to collect the experiences of carers in special COVID-19 wards in connection with the death and dying of COVID-19 patients. This should contribute to the development of targeted support strategies that can prevent moral injury and strengthen the resilience of healthcare staff.
Methods
Study design and setting
To uncover aspects that might have remained unobserved in a quantitative survey, a qualitative research design was chosen for data collection. 9 The study was conducted at the University Hospitals of Marburg (Hesse) and Ulm (Baden-Wurttemberg) in Germany, both of which had specialised COVID-19 wards during the pandemic.
The ethics committees of the medical faculties of the University of Marburg (reference number: 93/22) and the University of Ulm (reference number: 131/23) gave their approval to conduct the study, which was also registered in the German Register of Clinical Studies under the number DRKS00030425 on 6 October 2022.
The “Standards for Reporting Qualitative Research” served as a reporting guideline, enabling a structured and transparent presentation of our results. 10
Sample and study participants
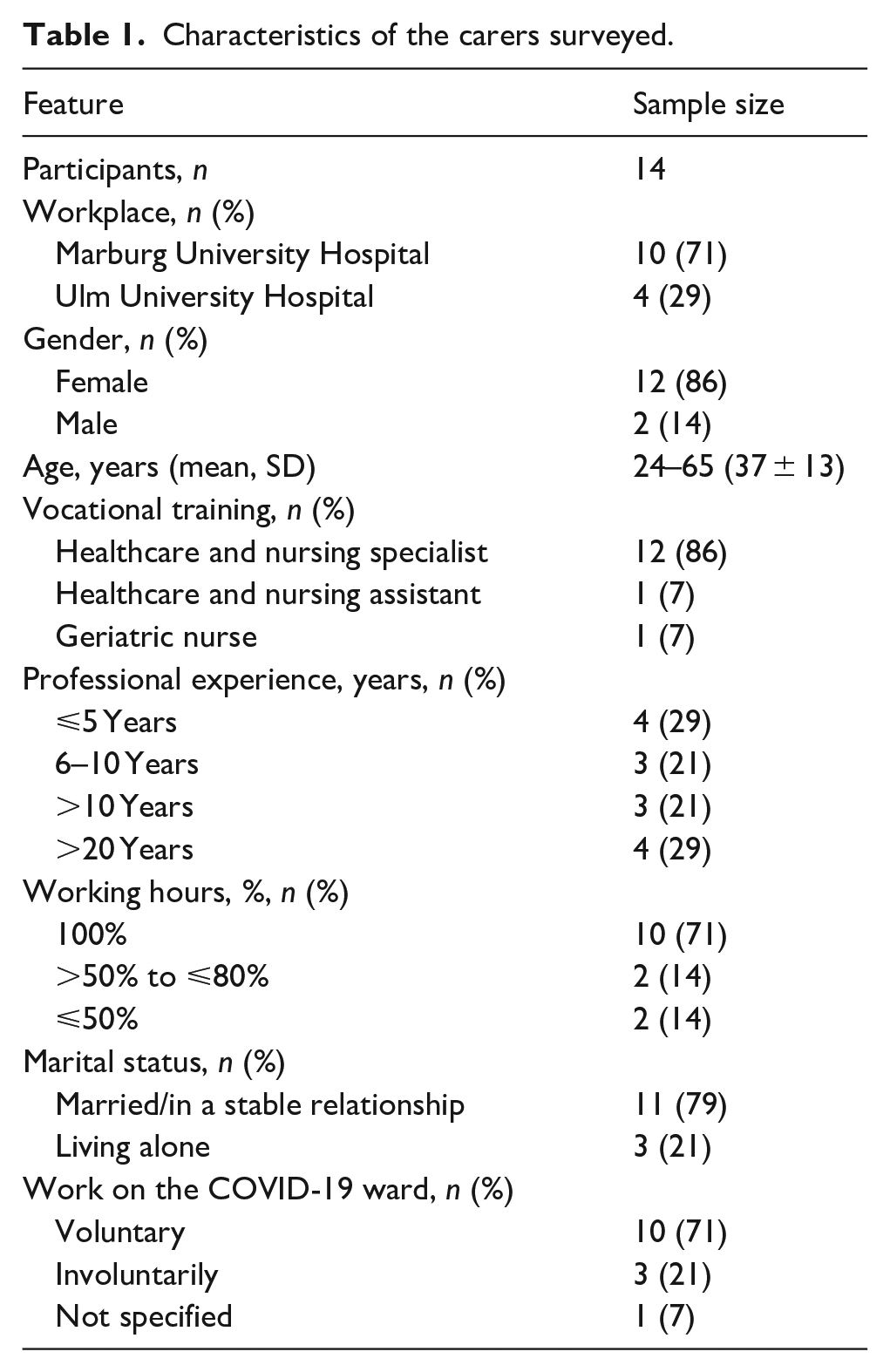
We specifically surveyed nursing staff who worked on specialised COVID-19 wards during the COVID-19 pandemic. The majority of respondents worked on these COVID-19 wards during the first two waves of the pandemic, which lasted in Germany from March to May 2020 and from September 2020 to February 2021. 11 All participants had to be at least 18 years old, have a good command of German and give written consent to take part in the study. The selection of participants was based on the methodological approach of “theoretical sampling” of grounded theory to ensure a representative sample and sufficient thematic saturation. Among other things, this means that data collection and data analysis run in parallel. As part of “theoretical sampling,” data collection is continued until theoretical saturation and contrast are reached and no new information or insights are gained. At this point, the data collection process is complete. We also followed this procedure in our study.12,13 Finally, we interviewed nurses from different hospitals and wards, from different age groups and genders, with varying years of professional experience and different professional training (specialised nurses, nursing assistants, geriatric nurses). Table 1 presents a comprehensive summary of the study participants’ characteristics.
Characteristics of the carers surveyed.
Recruitment
Persons were primarily recruited by the study team, who directly approached potential study participants. If interest was shown, the study information was distributed in the form of a prepared information sheet. E-mails with information about the study were also sent to ward managers and flyers with details about the study were distributed and displayed in the clinics. In addition, we used the “snowball system” and asked participants who had already been interviewed to motivate their colleagues to take part in an interview. 14 If potential interviewees agreed to be contacted, we contacted them by telephone, answered questions and arranged an interview date.
Data collection and interviews
The data collection took place between November 2022 and November 2023. At the beginning, all participants received both written and verbal study information and then gave their written consent. Participants were then asked to complete a form to collect socio-demographic data. 14 The interview started afterwards. Semi-structured face-to-face interviews were conducted with nurses in which they were asked about stressful events and experiences related to working on COVID-19 wards. 15 During the interview process, the participants were offered a supportive environment. They were encouraged to seek professional help or to continue therapeutic measures that had already begun. In cases where emotional distress became apparent during the interview, for example through crying, short breaks were taken and the participants were given space to talk about their reaction. The questions and structure of the interview guide were discussed and finalised in advance in the Qualitative Research Working Group of the Institute of General Practice and Family Medicine at the Philipps University of Marburg.14,16 The first interview served as a pilot interview. The interview guide and the form for recording the socio-demographic data were then revised. As numerous relevant aspects had already been mentioned, the data from the pilot interview were included in the analysis.
All interviews were recorded, then transcribed verbatim using MAXQDA 2022 software and pseudonymised.17,18
Data analysis
The data was analysed using qualitative content analysis according to Mayring.19,20 In view of the multi-layered nature of the topic under investigation, qualitative content analysis offers a suitable methodology for the systematic and detailed evaluation and interpretation of the interviews conducted. 21 In this way, new aspects and correlations could be identified, which enable a comprehensive understanding of the stress factors mentioned and their effects on carers.
Firstly, the transcripts were read to gain a basic understanding of the experiences described. Subsequently, the main categories were determined deductively based on the interview guide. Within each main category, sub-categories were formed by identifying the main themes. From new aspects that were mentioned independently of the questions asked, we inductively created further categories, whereby the category system was continuously expanded until all interviews were fully coded.20,22 To ensure the validity and reliability of the analyses, we continuously reviewed our categories, discussed them with the research team (L.K., S.B. and C.V.) and made appropriate adjustments where necessary.20,23
Results
Study participants
A total of 14 participants were interviewed in this qualitative study. Of these, 10 worked at Marburg University Hospital and 4 at Ulm University Hospital. The participants were between 24 and 65 years old and had different professional qualifications and variable work experience. The interviews, which took place at the interviewees’ place of work, lasted between 18 and 64 min (mean 38.64; SD 5.31). Table 1 provides a detailed overview of the characteristics of the study participants.
Key findings
Our survey revealed four main stress factors that were perceived as particularly stressful by the nursing staff surveyed in connection with the death and dying of patients on COVID-19 wards. The categorisation of the stress factors is shown in Figure 1.
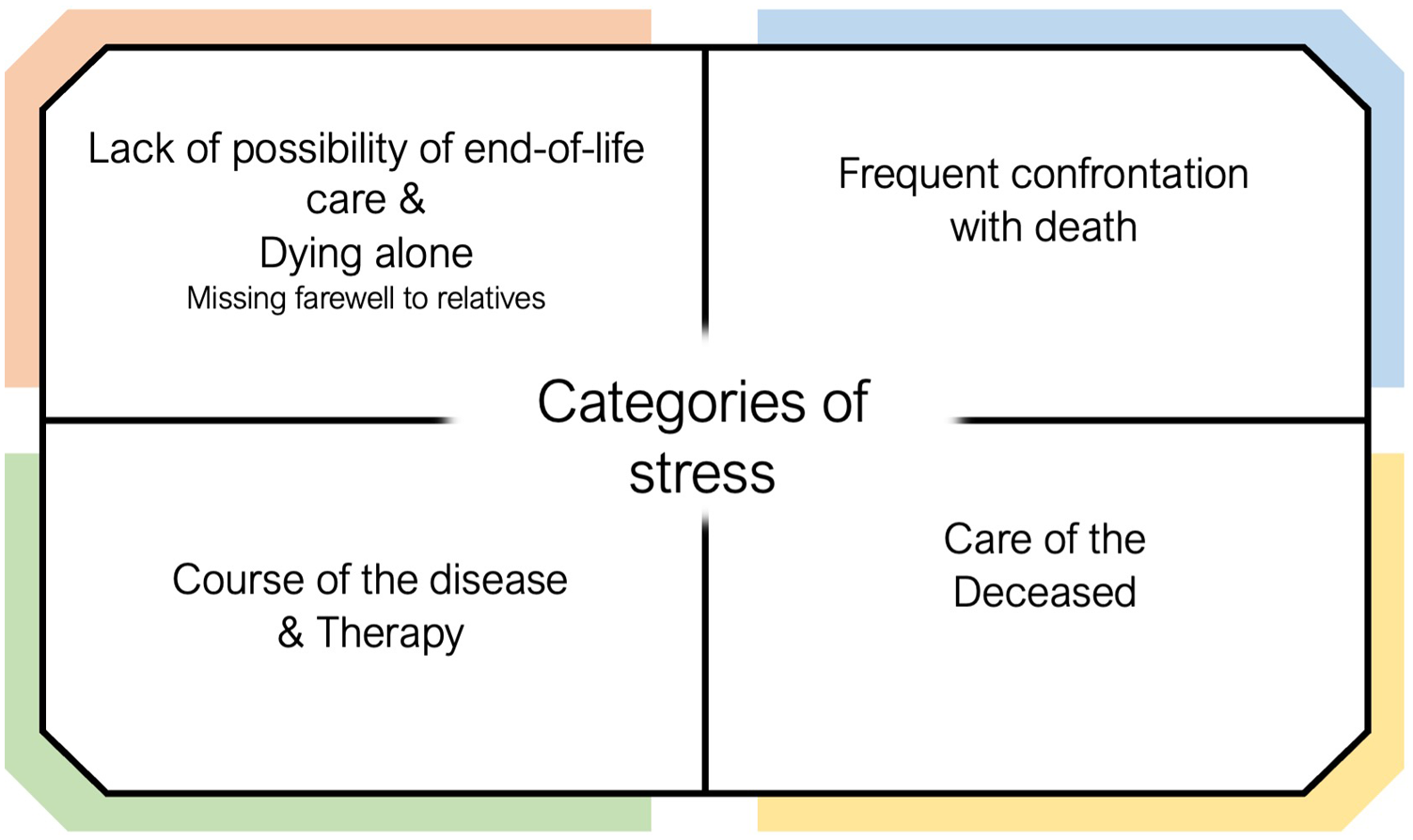
Overview of the four categories, including sub-categories.
In the following, the abbreviation R stands for respondent and the abbreviation I for interviewer.
Burden due to lack of possibility of end-of-life care and lonely dying of patients
The nursing staff surveyed reported considerable stress due to the limited opportunity to provide end-of-life care on COVID-19 wards. In particular, the lack of opportunity to actively assist dying patients and accompany them in their final journey was perceived as stressful.
But it wasn’t possible to really hold hands and be there for the patients. That took a bit of a toll on me [. . .]. (Interview 5)
A key aspect of the stress was the fact that the nursing staff were unable to give patients the attention they needed due to the high workload and were therefore unable to care for patients as much as they would have liked.
And because you simply can’t give them what they deserve. That was the terrible thing. This dying alone. You knew: “If I have time to look in there again in two hours, she might be dead.” I just felt sorry for the people. (Interview 6)
Some statements illustrate the emotional distress of carers who were concerned about not being able to provide patients with the appropriate care. They felt that they could not fully address patients’ needs, reflected intensively on these experiences and felt that they could not offer the patients the necessary dignity and support in their final moments.
So we don’t let anyone die alone. That’s a basic principle in nursing care. It just wasn’t possible. [. . .] These circumstances were bad. (Interview 3)
Finding deceased patients who had died alone and unaccompanied was perceived as particularly stressful by the nurses surveyed. This situation was described as a “loss of control,” among other things, and emphasises the emotionally challenging time working on COVID-19 wards.
And this loss of control and finding these people who had somehow died and no longer had anyone. That was very stressful for me. (Interview 1)
Lack of farewell between relatives and patients
The opportunity for family members to support dying patients in their final moments of life and provide them with dignified care was severely restricted by the pandemic-related ban on hospital visits. Patients’ relatives were not allowed to enter the hospital and say goodbye to their family members. This situation placed a considerable burden on the patients and was extremely difficult for the nursing staff to observe.
So no relative could say goodbye, the patient couldn’t say goodbye. You could no longer accompany the patient the way you wanted to. It went from “It’s nice to be able to accompany the patient” to “It’s absolutely horrible that patients have to die all alone.” Nobody should do that. (Interview 1) So it burdened me that it wasn’t possible to provide end-of-life care. That the relatives couldn’t go there. (Interview 6) And then you have the relatives there, begging and pleading to be allowed to see their loved one. That was bad. That was bad. Yes (R starts to cry). (Interview 3)
Stress caused by frequent confrontation with death
The frequent confrontation with dying patients and death was a noticeable emotional burden for the nursing staff. Many of the carers were not used to the frequency or the resulting intensity of the confrontation with death, which led to a high level of stress.
Unfortunately, there were a lot of them. So five or six died every day.
Do you feel that you were confronted more with death?
YES! Clearly. (Interview 2)
Also the emotional strain that came our way. Sometimes we really had to endure complete shifts with two or three corpses next to us. (Interview 3)
The daily experiences and emotional challenges of constantly witnessing the death of patients were a recurring theme in the interviews. The nursing staff described the constant proximity to dying or deceased patients on the COVID-19 wards as an extreme situation that led to considerable psychological stress.
For example, you were confronted with death every day. [. . .] And that wasn’t easy. [. . .] It wasn’t nice.
Have you been confronted with death more than in your work here now?
YES, MUCH MORE. Much more. (Interview 9)
[. . .] we met in the car park and hoped that ANYWAY today wouldn’t be as chaotic as the day before. That not so many people would die. (Interview 1)
For some of the interviewees, the stress led to excessive demands, as they did not know how to deal with the experiences adequately.
No one even asked how we dealt with it. It didn’t matter at all. And it was simply disturbing. We didn’t even know how to deal with it. (Interview 3)
To better cope with and process the situations experienced, several of the nurses surveyed expressed a desire for professional support, for example in the form of supervision. The fact that no questions were asked about the carers’ well-being and the required support was not provided led to disappointment and frustration among the employees.
We asked for supervision and didn’t get it. We said we all needed it. To work through things and so on. But nobody was interested. (Interview 2)
Burden due to disease progression and therapy
Our data analysis showed that the study participants were exposed to considerable stress, which was particularly related to the often serious course of the disease in COVID-19 patients. In particular, the apparently painful suffocation of many patients was perceived as traumatic by the nursing staff surveyed and impaired their mental well-being.
That people sometimes suffocated in agony. That was the kind of thing where you sometimes had a bit of a struggle. (Interview 13)
The burden was further increased by the unpredictable and often sudden deterioration in the health of COVID-19 patients. This often changed from seemingly stable to life-threatening within a very short space of time. The rapid change caused concern and stress among the nursing staff and gave them food for thought.
Because COVID is an arsehole. So the patient is sitting on the edge of the bed, smiling cheerfully at you, still eating, and from one moment to the next the oxygen saturation collapses. And then he suffocates. That’s bad. (Interview 11) I also experienced this on night duty. A relatively young woman, fifty years old. And it got massively worse within hours. Let’s put it this way, it makes you think. (Interview 8)
Nursing staff were often confronted with difficult and stressful decisions at the end of patients’ lives, which were not only emotionally draining but also posed major ethical challenges. Particularly in the context of the pandemic and the resulting overload of the healthcare system, it was unavoidable to make prioritisation decisions about which patients should be cared for next or whether there was enough time to accompany dying patients.
And this sorting out of patients like: “We could still do something about that, we might be able to save something. But it’s hopeless here anyway,” because you also had to do a triage for yourself. . . . Yes, that’s just not nice. When someone died, it was just: “Oh FINALLY a bed again.” (Interview 2)
They described how decisions had to be made regularly on the COVID-19 wards regarding the continuation or termination of treatment for seriously ill patients based on the predicted prospects of success. The carers did not always agree with these decisions. Some were of the opinion that such decisions were sometimes made prematurely and expressed the wish to fight more intensively for the patient’s survival. The frequency of decisions regarding the continuation or termination of treatment and the associated responsibility led to considerable psychological strain.
When the patient was visited and it was determined that his condition had deteriorated abruptly and he was dying, he was then switched to palliative care. And that bothered me. I would like to fight even more. (Interview 9) Until you realised that they were getting worse and worse and that you couldn’t help some of them any more, that you had to put more and more morphine on them. Yes, that was a bit difficult at times. (Interview 4)
The interviews showed that during their work on the COVID-19 wards, the study participants were repeatedly faced with situations in which they had to cope with profound emotional stress and ethical dilemmas in connection with the course of the COVID-19 infection.
Sometimes you could hear people shouting: “I’m dying. Help! Help!.” And by the time you had changed your clothes and got from one room to another, the person was lying there dead. And those were tough scenarios that made you sad. (Interview 3)
These experiences illustrate the enormous physical and emotional challenges faced by the nursing staff during this extraordinary time.
Burden of caring for the deceased
To minimise further infections, special measures were mandatory in the care of the deceased even after the death of patients infected with COVID-19. These included wrapping the deceased in body bags and comprehensive and thorough disinfection measures.
Yes, so [. . .] to put these people in this bin and put them in a bag and wipe them off and turn them round. [. . .] I think that’s inhumane. That has nothing to do with dignity. [. . .] I really didn’t want to do that. However, I knew it had to be done. So I thought that was really bad. (Interview 7)
This procedure was perceived by the interviewees as “inhumane” and “undignified” and described as the “worst” way of dealing with the deceased patients. The memories of these distressing experiences remain with some of the study participants to this day.
But the worst thing, that’s what I remember most from that time: driving the patients to the pathological ward, packing them in the bag beforehand and putting them in that iron container there. I thought that was the worst thing. [. . .] I really had the feeling that I was desecrating corpses because you had to squeeze them in there somehow. (Interview 6) So the worst thing for me was putting the people in the sacks. And the sound of them [the bodies in the body bags] banging on the metal coffins. [. . .] I often still think about that today. (Interview 4)
The interviews with the nursing staff revealed a deep emotional impact and considerable psychological stress caused by these exceptional circumstances during their work on the COVID-19 wards. In several cases, the interviews had to be briefly interrupted as the interviewees were confronted with the painful memories of their experiences while answering the interview questions, and either burst into tears or were on the verge of tears and needed a short break to collect themselves.
Discussion
Most important results
The results of our study clearly show that nursing staff working on COVID-19 wards during the COVID-19 pandemic were exposed to considerable challenges and stress, particularly when dealing with dying and deceased patients.
During the pandemic, the healthcare system was confronted with an unprecedented burden. In particular, the workload of healthcare staff increased to an unprecedentedly high level.2,24,25 The high volume of patients, their poor state of health, the often dramatic course of the disease with a high mortality rate and the frequent lack of opportunity to accompany patients as they died were identified as decisive factors in the burden, and not only in our study.26,27 The loss of the right of relatives to visit also meant that significant support for carers and assistance for patients was lost, which further contributed to the increasing burden.28 –30
Our findings are consistent with the literature, which shows that palliative care and end-of-life care were urgently needed at this time, but could not often be provided.30 –32 The lack of opportunity to provide end-of-life care due to the high workload was a great burden for the nursing staff interviewed. Studies show that carers often report emotional stress, moral injury and trauma. These experiences result from the inability to act according to their own ethical and moral values, such as not allowing anyone to die alone and providing the care that carers want to provide.33 –35
Moral injury, defined as the violation of one’s ethical compass, can lead to profound psychological problems such as depression and post-traumatic stress disorder. 36 Finding patients who had died unaccompanied and in solitude and having to witness how patients suffered from the lack of contact with and farewell to their loved ones was a particularly stressful experience for the carers interviewed.28,30 International studies illustrate the connection between this situation, described as a “loss of control,” the feeling of helplessness and being overwhelmed, other unfavourable working conditions during the pandemic and the psychosocial strain on staff.25,26,37 Research shows that such a working environment contributes to psychological stress and significantly increases the risk of burnout.2,27,38 The expectation of having to suppress one’s own feelings to remain fit for work could represent an additional burden and have a negative impact on mental health. 28
Nursing staff without specialised palliative care experience often had to adapt quickly to the new requirements under challenging conditions.30,32 As early as 2021, Oluyase et al. found that nurses with previous experience in palliative care were able to adapt better and faster to the situation during the pandemic. Some of the respondents in our study had previously had little experience with end-of-life care, palliative care and an increased frequency of dying patients on their home wards, which also explains the stressful feeling of more frequent confrontation with death and the difficulties in coping with the emotional burden. 31
Palliative care, the importance of which was already emphasised in a WHO resolution from 2013, is still insufficiently integrated into the healthcare system. 39 The international literature also points out that non-oncological nurses in particular often have poorer training in palliative care, which makes it even more difficult to deal with dying COVID-19 patients. 40 This suggests that more comprehensive training in palliative care for all nurses, regardless of their speciality, is urgently needed to better manage such situations in the future.
During their work on the COVID-19 wards, the carers were confronted with complex ethical and emotional challenges as well as serious decisions, especially in connection with the often serious course of the disease and the planning of further treatment steps. 30 In everyday clinical practice, it was often unavoidable to make prioritisation and treatment decisions that were difficult for the carers. 41 Some reported feeling that these decisions were made too quickly or were not optimal. The recurring feeling of not being able to adequately support or save patients despite intensive efforts led to frustration and a sense of futility for many, further increasing the feeling of loss of control. 27 Studies show that the feeling of futility can increase the moral and psychological burden on carers, increasing the risk of negative mental effects and the intention to leave the profession.19,26,33
Infection with SARS-CoV-2 cannot be completely ruled out even after the death of the patients, so special safety measures are required to prevent a risk to the nursing staff when caring for the deceased. 42 These measures include disinfectant washing and the use of body bags. 43 This handling of the deceased posed a considerable challenge for many of the carers, which arose in the context of the pandemic and in some cases forced them to act against their moral principles again. 44 In this context, the interviewees reported that they found the handling of the deceased in body bags “inhumane” and “undignified” and that they still remember this experience as the “worst” during the pandemic. 34
Although four overarching categories of stress were identified during the analysis, some study participants reported little or no perceived stress. In contrast to those people who seemed clearly shaken in the interview and sometimes reacted emotionally, for example by crying, these interviewees were characterised by a remarkably relaxed and calm attitude. Although they named individual aspects of their everyday working life that they found disturbing, these were described less intensively and appeared to be less serious in their subjective impact. In addition, it was noticeable that these people tended to talk about functioning routines, good teamwork and work that was perceived as meaningful. One possible explanation for the low level of stress experienced lies in the structural and social framework conditions: The people in question all worked in a team with a stable staff composition and in familiar spatial structures. Such constant and reliable working conditions can be seen as protective factors that help to reduce or prevent the perception of stress.45,46 In addition, compared to participants from other wards, it was observed more frequently that these people explicitly named their free time as a resource that helped them to recover and restore their mental resilience. The active use of opportunities for regeneration outside of work could therefore make a further contribution to stabilising the subjective experience of stress.
Nevertheless, the statements of the interviewees make it clear that traumatic events, moral injuries and the recurring mental reliving of stressful situations represent a profound emotional and psychological burden for carers, significantly increasing the risk of long-term psychological impairment.35,44,47 These experiences emphasise the need for comprehensive support in dealing with ethically challenging situations in times of crisis. Psychological support for carers has been inadequate during the pandemic. Many participants in our study felt mentally overwhelmed and stated that systematic psychological support was lacking.
Various sources, therefore, urgently call for the systematic introduction of psychological interventions for healthcare workers to cope with both the short-term and long-term psychological consequences of the pandemic and to protect carers.33,36,41,48 These interventions could include supervision and psychological counselling services to enable caregivers to process their experiences.49,50 The support provided should not only be used after the fact to alleviate psychological stress, but should be implemented before or during the situations described to proactively counteract overload. 51
The results suggest that a higher level of professional expertise and practical experience in dealing with dying and seriously ill patients can help to better cope with stressful situations – such as those that have occurred frequently during the COVID-19 pandemic. More comprehensive training in end-of-life and palliative care and in dealing with dying patients could prepare nurses to deal with challenges such as those posed by the pandemic, for example a higher number of deaths and serious illnesses, and improve their ability to cope with stressful situations and strengthen their adaptability in critical and emotionally challenging scenario.31,40 Therefore, well-founded training not only contributes to the quality of care but also strengthens the mental well-being of staff in the long term.
Strengths and limitations
Our study makes it possible to gain in-depth insights into the perspectives and experiences of carers. Given the complexity of the topic, the use of a qualitative research design was considered appropriate to shed light on aspects that might not have been captured in quantitative surveys. Our data analysis was both deductive and inductive. This allowed us to identify stress factors that may not have been explicitly covered by the interview guide. The pseudonymisation of the data may have encouraged participants to be open and honest about their experiences, as they were confident that their identity would remain protected and they had no fear of negative consequences.
A limitation of our study is that some study participants only mentioned a few stress factors, which made it difficult to conduct the interview, as the interview guide was not designed to deal with the perception of little or no stress. One reason for low stress could be that these interviewees all came from a team that was constant and worked in familiar premises.45,46
Another limitation of our study lies in the recruitment process. Although we endeavoured to compile a broad and representative sample, the motivation to participate in the study among the carers was limited. This also extended the recruitment period. The results are based on the experience reports of 14 carers from Ulm and Marburg. Expanding the sample to include more hospitals, regions and a larger number of participants could make the results more generalisable. The predominantly female sample reflects the gender distribution in the nursing sector.
The continuous exchange within our research team and our qualitative research group about the methodology used and the data collected allowed us to minimise subjective interpretations and strengthen the validity of the results.
Conclusion
The COVID-19 pandemic posed major challenges for the healthcare system. Our findings show that working on COVID-19 wards and caring for COVID-19 patients placed considerable psychological strain on carers, some of which continues today. The deployment scenarios, which often go beyond their experience and training, pose a risk of moral injury and the development of mental illness for carers. Our study confirms existing findings on the psychological stress of nursing staff during the COVID-19 pandemic and supplements them with the specific finding that dealing with dying and deceased patients, experiencing moral conflicts and the feeling of having to act against one’s own ethical values are key stress factors. The identification of our categories of stress highlights the need for psychosocial support systems, such as regular supervision and training in palliative care and end-of-life care. Such services could not only help to relieve the burden but also promote the long-term mental health of staff.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524251355655 – Supplemental material for Death and dying during the COVID-19-pandemic – A qualitative evaluation of stress factors for nursing staff
Supplemental material, sj-pdf-1-pcr-10.1177_26323524251355655 for Death and dying during the COVID-19-pandemic – A qualitative evaluation of stress factors for nursing staff by Lea Kiefer, Stefan Bösner, Jan Adriaan Graw and Christian Volberg in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank all nursing staff members who were willing to share their experiences with us.
Ethical considerations
The ethics committees of the medical faculties of the University of Marburg (93/22) and the University of Ulm (131/23) authorised the conduct of the study and the study was registered in the German Clinical Trials Register (DRKS00030425) on 6th October 2022.
Consent to participate
Informed consent was obtained from all participants.
Consent for publication
All participants have given their written consent to the pseudonymised publication of the results.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open Access funding provided by the Open Access Publishing Fund of Philipps-Universität Marburg.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
To protect the privacy of the study participants, no original data could be published. The data supporting the results of this study and additional material are available upon request from the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.