
Abstract
Objectives
The ongoing COVID-19 pandemic has led to an unprecedented loss of life and a severe economic downturn across the globe. Countries have adopted various social distancing and vaccination policies to reduce the spread of the disease and lessen the impact on healthcare systems. The world should work together to confront the disaster and challenge of COVID-19.
Methods
This study uses stochastic frontier analysis to measure the efficiency and influencing factors of the global response to COVID-19 epidemics and to provide follow-up strategies and reference guidelines.
Results
The results of this study show that (1) the average efficiency of the global response to COVID-19 is not good, with significant space for improvement of up to 60%; (2) adequate medical supplies and equipment can reduce mortality; (3) the initial implementation of social distancing policies and wearing masks can effectively reduce the infection rate; and (4) as infection rates and vaccination rates increase so that most people have basic immunity to COVID-19, the epidemic will gradually be reduced.
Conclusions
As the world becomes more aware of the COVID-19 disease, humans will gradually return to normal social interaction and lifestyles. The results of this study are expected to provide a reference for the future direction of the global fight against epidemics and the improvement of public health policies.
Introduction
In December 2019, a highly contagious virus was first detected in Wuhan, China. The virus was named “SARS-CoV-2,” and the infectious disease was named “COVID-19.” On 11 January 2020, China announced that the first man to contract the new virus had died on 9 January. Countries worldwide were made aware of the COVID-19 epidemic because Wuhan, China, reported its second death to the World Health Organization (WHO) on 17 January 2020. The United States health service announced that three major domestic airports had started screening passengers from Wuhan. Airports across Asia also enforced mandatory screening of passengers arriving from high-risk areas of China. On 23 January, China declared a lockdown of Wuhan, imposed a nationwide quarantine, and suspended flights and trains. The WHO stated the COVID-19 outbreak was not a global emergency, and there was “no evidence yet” of human-to-human virus transmission outside China. After two days of debate at the meeting of the WHO emergency committee, the committee decided not to declare the rising COVID-19 outbreak a Public Health Emergency of International Concern (PHEIC) for the time being. 1
However, on 30 January 2020, one month after the first case, the WHO did declare COVID-19 a PHEIC. It was confirmed as a pandemic by the WHO on 11 March 2020. Within months of the first COVID-19 outbreak, cases appeared on every continent and in most countries. On 4 April 2020, the WHO reported that more than 1 million COVID-19 cases had been confirmed globally, a more than 10-fold increase in less than a month. The COVID-19 pandemic has led to unprecedented loss of life and severe economic recession worldwide.2–4 Globally, a cumulative 760,897,555 confirmed cases of COVID-19, including 6,874,585 deaths, have been reported to the WHO as of 15 March 2023. The global distribution of confirmed COVID-19 cases is shown in Figure 1. The United States has the highest number of confirmed deaths at 1,113,229, followed by Brazil with 699,310, and India with 530,789 deaths. 5
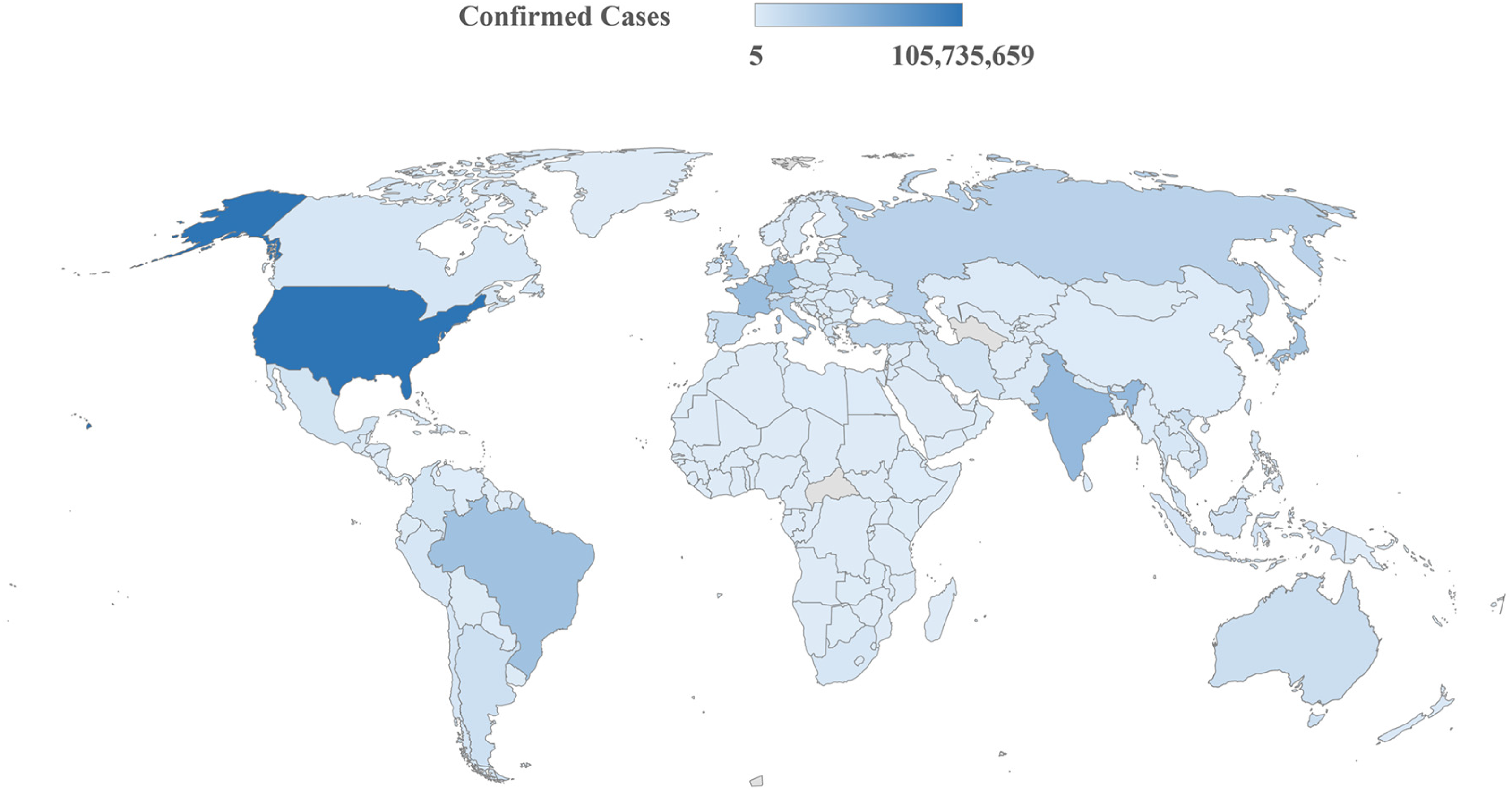
Global distribution of confirmed COVID-19 cases (through March 2023). 6
The early days of the COVID-19 pandemic have led to a variety of prevention and mitigation measures around the world, from the closure of international borders to various social distancing and isolation measures at the local level, to reduce the spread of the disease and reduce the burden and impact on healthcare systems. China locked down Wuhan, a metropolis of 12 million people, on 23 January 2020 to contain the COVID-19 outbreak. Similar lockdowns and clearances followed in all 15 other cities in Hubei province, which was home to approximately 57 million people, while other Chinese cities followed with varying degrees of restrictions. Wenzhou in Zhejiang province, for example, limited one person per household to one outing every two days. Restrictions and lockdowns in China appeared to curb the spread of COVID-19 effectively. However, these measures have greatly disrupted people's work and lifestyle and may also have a significant impact on their health and well-being. 7 New Zealand implemented the strictest lockdown measures in the world, raising COVID-19 prevention measures to the highest level of alert level 4 on 25 March 2020 and initiating a nationwide lockdown, border controls, and a complete halt to international travel. New Zealand's national lockdown and clearance policy was once the poster child for the COVID-19 response, as the government's rapid response to the pandemic and geographic isolation kept the country out of the pandemic until the end of 2021. However, due to this strict blockade, its economy suffered a huge loss of approximately US$10 billion. 8 Japan issued measures for COVID-19 on 25 February 2020, urging people not to rush into hospitals without consultation to reduce the risk of exposure and cross-infection in healthcare facilities. In order to prevent large gatherings and crowded areas, measures such as telecommuting, staggering commuting times, leaves of absence when someone has cold-like symptoms, and closure of primary, middle, and high schools were advocated. 9 Some countries declared a public health emergency due to shortages of protective gear, medical supplies, and equipment but did not consider lockdowns or quarantines as options for responding to the spread of COVID-19 in order to avoid severe economic impacts, which led to increasing COVID-19 cases and deaths. 10 The Singapore government was among the first to close borders, quarantine all overseas travelers, and actively trace contacts. Singapore introduced a mandatory mask policy in April 2020, requiring everyone to record their movements by scanning bar codes. 10
The United States began implementing various social distancing policies in mid-April 2020 to reduce the burden of COVID-19 on the healthcare system and reduce its spread. These included shelter-in-place orders (SIPO), remote offices, school closures, a ban on large gatherings, closure of entertainment venues, seating restrictions in bars and restaurants, and mask mandates.9,11,12 Without vaccines and drug treatments at the onset of the pandemic, the aforementioned social distancing policies became a first-line response. 12 However, the literature on the effectiveness of social distancing and control policies in curbing the spread of COVID-19 was unclear and unconfirmed at this early stage. Some studies have suggested that early social distancing policies, especially the ban on large gatherings, can indeed reduce the transmission and diagnosis of COVID-19, but do not have a significant impact on mortality and cause significant losses to the overall economy.8,12,13 Other studies, such as by Friedson et al., 14 who focused on the impact of the 29-day SIPO policy in California, found that the control policy was effective and reduced the number of confirmed COVID-19 cases per 100,000 people by 125.5–219.7 despite the economic cost and reduced the number of COVID-19-related deaths by 1661, with the largest reduction in COVID-19-positive cases in countries that introduced lockdowns earlier. 14 The above studies show that COVID-19 epidemics could be slowed by an aggressive lockdown policy in the early days of the pandemic without a vaccine. 10
The relatively high admission rate of patients infected with COVID-19, especially those requiring treatment in intensive care units (ICU), has resulted in a significant impact on medical services and medical personnel, as well as on medical services for other diseases.15–18 Countries such as Germany, Austria, Portugal, Spain, Switzerland, and Italy had strong public and universal health services but had suffered health budget cuts in recent years due to the 2008 financial crisis, which reduced gross domestic product. They had a particularly successful response to the COVID-19 pandemic and low fatality rates in early 2020, but health services would become overstretched. By the end of 2020, the situation had rapidly transformed into a shortage of ICU beds, a surge in infection and fatality rates, and one of the most serious COVID-19 hotspots in the world.19–22
Three years after the start of the COVID-19 pandemic, the world has implemented countermeasures and mitigation policies. The early social distancing and lockdown control policies did work but, in the long run, they caused great losses to countries, societies, and economies, while the reduction of interpersonal contact impacted physical and mental health. 23 Earlier studies by Karako et al. 9 suggested that, in Japan, reducing the time spent in crowded areas to less than 4 hours could suppress the spread of infection, and so they suggested that the countermeasures to control the spread of COVID-19 should include avoiding crowded places as much as possible. Hâncean et al. 24 conducted a study involving 6895 patients in Bucharest, Romania, from August to October 2020, along with 13,272 individuals who interacted with them. They recorded the participants’ gender, age, and occupation and constructed a statistical model on the network effects of human-to-human transmission in order to investigate potential infection routes of COVID-19. Their findings indicated that a medical occupation had no significant effect on the spread of the virus. Instead, a transmission chain was observed among private sector workers, as well as between spouses, siblings, and older relatives. Some studies have shown a positive correlation between population density and mortality because a high population density facilitates the spread of the virus through close person-to-person contact. Transmission of COVID-19 is more likely to occur in areas with higher population density.25–28
When someone infected with COVID-19 coughs, sneezes, talks, sings, or breathes, the virus may be transmitted from the mouth or nose of the infected person in the form of small liquid particles, which range from larger respiratory droplets to smaller aerosols. 29 Guidelines from the Centers for Disease Control and Prevention (CDC) and the WHO recommend wearing masks to prevent the spread of COVID-19. 30 According to the epidemiological data, the universal mask measures implemented in Japan, Hong Kong, Singapore, South Korea, and Taiwan were most effective in initially reducing the spread of COVID-19. 16
On 5 January 2021, the WHO's Strategic Advisory Group of Experts on Immunization (SAGE) met to discuss the Pfizer/BioNTech vaccine, and it became the first vaccine to receive WHO validation for emergency use for COVID-19. 1 Several studies and observations have shown that vaccines are the most effective and cost-effective way to prevent and control infection, but herd immunity is still needed to end the COVID-19 pandemic.31,32 In addition, patients who are fully vaccinated (FV) against COVID-19 reduced length of hospital stay, risk of ICU admission, and risk of death compared to those who are not vaccinate, and these vaccines protect against SARS-CoV-2 infection.33,34 However, the risk of a breakthrough case of severe COVID-19 following vaccination remains, especially among people at higher risk of severe disease.35,36
Historically, there have been few studies utilizing techniques like stochastic frontier analysis (SFA) to investigate the association between disease occurrence and mortality. In 2000, Sindo et al. 37 used SFA to construct an estimation model for pneumonia and influenza mortality in Japan. They aimed to mitigate the underestimation of actual death counts by utilizing excess deaths as a measure. The numerical findings revealed a substantial increase in influenza-related mortality compared to previous estimates. It is hoped that this mortality rate estimation model has the potential to enable timely prediction of influenza outbreaks in the future. Over the past three years, much literature has explored the impact of the COVID-19 pandemic on various global conditions. However, thus far, most have focused on the effectiveness of medical treatment of the virus, while only a few studies of short-term durations of several months to one year have addressed the topic of global effectiveness in combating the COVID-19 pandemic. 22 Gearhart et al. 12 used order-m efficiency estimates to investigate the efficiency of the COVID-19 social distancing policy in the United States during the first 100 days of 2020 and found that a more effective strategy would have been to implement the policy in densely populated areas. While banning large gatherings is the most effective policy, shelter-in-place orders have less impact than nonessential business closures. The preliminary indications are that early withdrawal of social distancing policies can lead to surges in COVID-19 cases. Breitenbach et al. 38 applied data envelopment analysis (DEA) to explore the adverse output of mortality and infection rates in 220 countries by November 2020 and took the numbers of doctors and nurses and healthcare spending per 100,000 people as inputs. Their findings found that most countries were inefficient in fighting the COVID-19 pandemic. Pereira et al. 22 explored 55 member states, associate members, partners, and other countries of the Organization for Economic Cooperation and Development (OECD) with DEA. The outputs of the study included population, infectious diseases, triage, hospitalizations, and ICU admissions, and the inputs included health expenditure and cost. Estonia, Iceland, Latvia, Luxembourg, the Netherlands, and New Zealand were found to be efficient countries. Lupu and Tiganasu 39 used DEA to assess the effectiveness of the European health system in combating COVID-19 during 2020, with inputs including COVID-19 cases, doctors, nurses, hospital beds, health expenditures, and outputs including COVID-19 deaths. They found that Italy, Belgium, Spain, and the United Kingdom were less efficient than other countries in the first phase of the pandemic. Ahmad et al. 40 used SFA to explore the efficiency of countries in Southeast Asia in response COVID-19, finding them to be Thailand, Malaysia, India, and the Philippines in order of least to most efficient. Maity et al. 41 used SFA to explore the efficiency of combating COVID-19 in the states of India. The outputs included the recovery rate of COVID-19, and the inputs included the numbers of doctors, nurses, and isolation beds and exogenous variables such as the elderly population, gender, literacy rate, and urbanization rate. The results showed that investments in health infrastructure, such as doctors, nurses, police, isolation beds, and ICU beds, contributed to increased rates of COVID-19 recovery. An aging population can lead to inefficiency and population density hurts efficiency. Kınacı et al. 42 used DEA and SFA to discuss a study period from 3 March 2020 after the first detected case in Turkey by using the numbers of COVID-19 cases, deaths, and beds in ICU and other efficiency analyses. Their analysis showed that efficiency in the early epidemic stage was not good, but there has been a gradual improvement since then. However, due to the study's short period for data collection, the change was very different from the actual epidemic.
In conclusion, the outputs used in studies on COVID-19 efficiency have been primarily the numbers of deaths or confirmed cases, while the inputs have been primarily the numbers of doctors, nurses, hospital beds, and beds in the ICU. Most methods used to study efficiency have been DEA or SFA. Both used the production frontier (efficiency frontier) to measure efficiency. DEA is a nonparametric method that uses linear programming to estimate frontier production functions, measure multiple inputs and outputs, and calculate the relative efficiency of each evaluated unit. SFA is a parametric approach involving a theory of econometric models and microeconomics that requires combining data to estimate production functions regarding hypotheses or statistical tests. 43 This study used SFA because the estimation results adopt absolute efficiency, which is more stable than DEA. SFA can also consider random error terms, which are more suitable for situations with large differences in sample data size, and it is not susceptible to the influence of outliers, which may cause calculation results to deviate from the actual situation. The results of SFA will not have the same efficiency value, that is, 1, of multiple decision-making units (DMUs) as the results of DEA. 44 SFA is more suitable for exploring the changing trend of global efficiency in combating COVID-19 year by year. In addition, this research will take the number of COVID-19 deaths as undesirable output and divides the three years of the COVID-19 pandemic (the time of data collection is from January 2020 to December 2022) into two stages for analysis. The first phase is 2020 when the COVID-19 vaccine was not yet completed. The second phase is 2021–2022, when the vaccine had begun to be administered. This study measures the effectiveness and impact factors of the global response to the COVID-19 pandemic over three years. This study aims to measure which strategies or policies are most effective in combating the COVID-19 pandemic in countries and regions worldwide and which need to be improved in terms of their performance to address and mitigate the ongoing COVID-19 disease and mortality. The study results are also expected to provide a reference for the community to consider how to reduce and propose appropriate measures to improve their public health policies to eliminate the PHEIC of COVID-19. In the future, it can also be used as a reference and effective guide for policymakers and health units in countries worldwide in case of epidemics or health crises.
Methodology
SFA method
Efficiency evaluation measures the operational performance of a DMU against the operational space that the DMU can improve. Efficiency is the problem of measuring the optimal efficiency of input and output under the goal of maximum output or minimum cost. Farrell 45 argued that nonparametric and parametric methods can be used to measure efficiency and proposed an efficiency measurement method that has become the pioneering technique boundary analysis. 46 DEA is the most commonly used nonparametric method, while SFA is the most representative parametric method. Both methods are commonly used to measure various performances.
SFA is a method proposed by Aigner et al.
47
and Meeusen and van den Broeck.
48
The main concept of SFA is to connect the most efficient input–output combination points to form a production efficiency boundary. Only the enterprises at the leading edge of efficiency have technical efficiency. Battese and Coelli
49
proposed a Cobb–Douglas stochastic boundary production function model for continuous intertemporal data. Considering that environmental characteristics influence COVID-19, exogenous variables are included to estimate the efficiency of the global response to COVID-19 and analyze the impact of exogenous variables on COVID-19 deaths. The Cobb–Douglas stochastic frontier model takes the form
46
:


Samples and data sources
The samples and data used in this study are from the University of Washington's School of Medicine. The Institute for Health Metrics and Evaluation (IHME) 50 provides the data on COVID-19 modeling estimates. The IHME collected COVID-19 data from various sources provided by more than 200 countries and territories, including local and national governments, hospital networks and associations, the WHO, and the data reports from Our World. Most came from a Johns Hopkins University (JHU) data repository. Data on COVID-19, including cumulative (or daily) cases, deaths, etc., were collected by JHU as a free repository and were verified by the CDC. One reason the number of COVID-19 deaths and confirmed cases observed in the data provided by the IHME may differ from the figures reported by governments is the differences in how data are estimated and identified by various countries and regions. The IHME is designed to address irregularities in daily data on deaths or confirmed cases of COVID-19. IHME uses a hybrid modeling approach to generate our forecasts, which incorporates elements of statistical and disease transmission models. IHME estimate past daily infections in a modeling framework that leverages data from seroprevalence surveys, daily cases, daily deaths, and, where available, daily hospitalizations. 50
This study collated data on COVID-19 from countries and regions worldwide from 2020 to 2022 in IHME's COVID-19 database. After deleting countries and regions with incomplete data, data from 136 countries and autonomous regions were obtained, as shown in Table 1.
136 countries and autonomous regions.

Variables and empirical model
Based on the severity of the risk of illness and death caused by COVID-19 over the past three years and the issue of how to reduce the characteristics related to diagnosis and death, this study selected data of inputs, outputs, and exogenous variables to explore the effectiveness of the global fight against SARS-CoV-2 infection and treatment. The research results are expected to serve as a reference for all fields of research to study the direction and strategy of reducing or relieving the PHEIC of SARS-CoV-2.
This study collated data from 2020 to 2022 from the COVID-19 database of IHME. Cumulative deaths (CD; raw data with an excess mortality scalar applied) from COVID-19 were used as undesirable output. The WHO
51
proposed that measuring excess mortality is essential for understanding the pandemic's impact. The changes in mortality trends can provide information for policymakers to reduce excess mortality and effectively prevent future crises. Excess mortality can be used as an indicator of disease prevalence to estimate an epidemic's duration, region, and scale. The true extent of excess deaths is often obscured because of the limited investment in data systems in many countries. These new estimates use the best available data and are generated with a sound methodology and in fully transparent manner. Therefore, the cumulative number of COVID-19 deaths due to adverse outcomes adopted in this study is the excess mortality rate measured from the original data, which can better reflect the actual situation of COVID-19 deaths. Inputs in this study include cumulative infections (CI; mean estimate), cumulative COVID-19 hospital beds needed (bed; mean estimate), and cumulative COVID-19 ICU beds needed (ICU; mean estimate). The undesirable outputs and inputs above can be substituted into Equation (1) to obtain Equation (3):


Descriptive statistics of variables.

Results
Table 3 and Figure 2 show that the average inefficiencies of various countries and regions in the global fight against the COVID-19 pandemic in 2020, 2021, 2022, and 2020–2022 are 0.602, 0.666, 0.530, and 0.599, respectively. These values indicate considerable room for improvement by up to approximately 60%. The top 10 countries in the three-year average efficiency ranking (with their inefficiency value) from 2020 to 2022 are Venezuela (0.107), China (0.108), Qatar (0.127), Singapore (0.128), Kuwait (0.223), Mongolia (0.250), Sri Lanka (0.264), Taiwan (0.287), Thailand (0.304), and Saudi Arabia (0.308). The bottom five countries are Finland (0.867), Mozambique (0.867), Denmark (0.845), Bolivia (0.844), and Zambia (0.810) in order. The average inefficiency value was 0.599, which indicated a poor global response to the COVID-19 pandemic, with 59.9% room for improvement. The top 10 in terms of efficiency in 2022 were China (0.006), Myanmar (0.054), Venezuela (0.054), Kuwait (0.093), Qatar (0.101), Saudi Arabia (0.133), Singapore (0.133), Sri Lanka (0.151), United Arab Emirates (0.171), and Chad (0.199). The last five were Malawi (0.893), Madagascar (0.883), Finland (0.860), Bahamas (0.852), and Mozambique (0.846) in order. The average inefficiency value was 0.530, indicating poor global effectiveness in combating the COVID-19 pandemic, with 53% room for improvement. The inefficiency values and efficiency rankings of all the countries and regions in 2020 and 2021 are shown in Table 3.

Distribution of three-year mean inefficiencies in the global response to the COVID-19 pandemic in 2020–2022.
Estimates of the COVID-19 pandemic inefficiencies of SFA for 136 countries and regions.

From Table 3, the top countries with a better efficiency ranking over the three years (2020–2022) were mostly able to maintain that ranking. High-ranked countries such as China, Qatar, and Singapore implemented strict and comprehensive quarantine measures in early 2020 and implemented a national COVID-19 vaccination policy in 2021. China implemented a zero-clearance policy from the early stage of the COVID-19 outbreak in 2020 until the public demonstrations in December 2022 due to the people's frustration in the three-year fight against COVID-19. After China ended its policy under pressure from economic recession and the public, it caused a shortfall in medical services, a sharp rise in deaths, and shortages of medicines. The number of confirmed cases surged for a short term as a result of the sudden lifting of lockdown measures before gradually decreasing. Therefore, strict infectious disease prevention and control measures against COVID-19 have been lifted since January 2023.53,54 The number of reported deaths from COVID-19 in Qatar has been low, likely because of the robust healthcare system and the average age of its young and healthy residents. In the beginning, the Qatari government also implemented lockdown measures; closed mosques, shops, restaurants, and other places; and strictly enforced the mandatory wearing of masks in public places. People who test positive for COVID-19 have immediate, free access to quality health care. 55
In January 2020, Singapore set up an interministerial anti-epidemic task force in response to the epidemic. In the beginning, strict clearance policies, wearing masks, and entry and exit tracking and control measures were implemented. Singapore understands the importance of early access to internationally certified vaccines and vaccination to reduce deaths and contain the spread of COVID-19. However, after the outbreak of the Omicron variant in September 2021, the number of confirmed cases and deaths increased significantly. Nevertheless, with the high vaccination rates for COVID-19 and estimates that nearly 90% or more of the population has contracted COVID-19, Singapore has achieved a strong “mixed immunity.” In March 2022, Singaporean authorities announced that social control measures would be further relaxed, and Singapore would enter the final phase of the plan to live with COVID-19. 56 Singapore's policy is to transition from eliminating COVID-19 to living with COVID-19. This policy requires high vaccination rates and well-communicated transition plans, with a gradual reduction of mitigation measures over time. 57 Slowing the spread of the disease, maintaining functioning healthcare systems, and vaccination to reduce severe illnesses and deaths are the main policies and goals of the COVID-19 response in these countries, which show good results.
Maximum-likelihood estimation (MLE) is used for the SFA analysis for the two phases of this study. The estimated results of the first phase in 2020 are shown in Table 4. The second phase is 2021–2022. The difference between the two phases was addition of the exogenous variable of the cumulative all FV. The estimation results are shown in Table 5. Table 4 shows that in the first year of the COVID-19 pandemic in 2020, cumulative infections (estimate: 0.335155) and the cumulative number of hospital beds required (estimate: 0.712924) are both very significantly positively correlated with the efficiency of cumulative deaths. In other words, the higher the number of cases and hospitalizations, the higher the number of deaths from COVID-19. In terms of exogenous variables in 2020, there is a significant positive correlation between cumulative death inefficiency and population density (estimate: 1.211623), indicating that a higher population density is likely to lead to more deaths from COVID-19. Reducing the risk of close contacts, such as at large gatherings, can reduce the infection rate. Second, cumulative death inefficiencies showed a very significant positive correlation with the number of ICU beds available (estimate: 1.979876), suggesting that sufficient and improved access to care and equipment could reduce the mortality of COVID-19. Third, cumulative death inefficiency showed a significant positive correlation with the percentage of people who wore masks outside the home (estimate: 3.475606), suggesting that wearing masks outside the home in the early stages of COVID-19 could indeed reduce confirmed deaths. Fourth, there was a significant negative correlation between cumulative death inefficiency and the number of hospital beds available (estimate: −2.09578), indicating that countries that are unable to provide a sound public health system and adequate medical services to combat COVID-19 suffered an increased number of deaths.
Estimates of the stochastic frontier function of 2020.
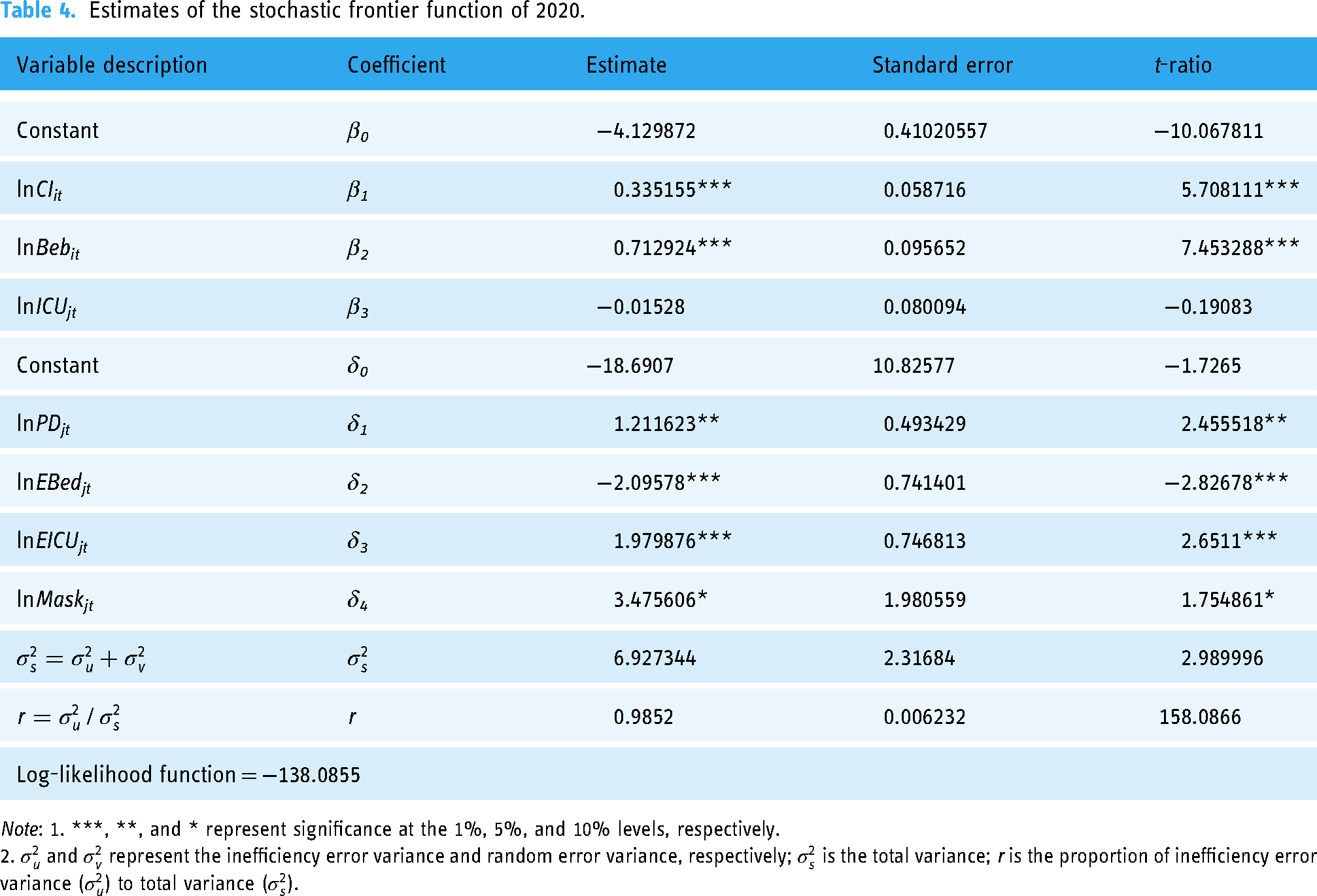
Note: 1. ***, **, and * represent significance at the 1%, 5%, and 10% levels, respectively.
2.
Estimates of the stochastic frontier function of 2021–2022.

Note: 1. *** and ** represent significance at the 1%, and 5% levels, respectively.
2.
Table 5 shows that both cumulative infections (estimate: 0.228937) and the cumulative number of hospital beds required (estimate: 0.596755) during the COVID-19 pandemic in the second phase (2021–2022) are very significantly positively correlated with the efficiency of cumulative deaths. In other words, the higher the number of cases and hospitalizations, the higher the number of deaths from COVID-19. Secondly, the cumulative number of ICU beds required (estimate: 0.18662) showed a significant positive correlation with the efficiency of cumulative deaths. The higher the number of confirmed ICU patients required, the higher the number of COVID-19 deaths. In addition, exogenous variables such as population density, number of inpatient beds available, number of ICU beds available, the wearing of masks outside the home, and full vaccination were not significantly associated with cumulative deaths in the second phase (2021–2022), possibly due to the increased duration of the epidemic resulting in higher rates of confirmed COVID-19 cases and vaccinations. Most people have basic immunity to COVID-19. Because population density promotes the spread of the virus through close contact between people, lockdown policies, school closures, and wearing masks are used to reduce the spread of close contact, so the findings are consistent with related studies. However, relevant studies9,23 also pointed out that the blockade policy would cause social and economic losses, impact interpersonal relations, and affect physical and mental health. The results of this study are similar to those speculated by Kim et al. 56 and Owens and Parry 57 and are similar to the recent situation in Singapore, China, and many other countries, where most people have obtained a good “mixed immunity.” The current stage is important for the world to gradually relax COVID-19 control measures over time and to transition to living with COVID-19.
Discussion
This study measured the effectiveness of the global response to the COVID-19 pandemic in 136 countries and territories from 2020 to 2022 and explored the global COVID-19 outbreak and response strategies. In this study, cumulative deaths due to COVID-19 were adopted as undesirable output and excess mortality was applied to measure the data of original cumulative deaths because this data could be closer to and better reflect the actual number of COVID-19 deaths. This study uses the Cobb–Douglas stochastic frontier model and can be divided into two phases to analyze and discuss the COVID-19 pandemic. The first phase was 2020, when there was no vaccine for COVID-19. The second phase was 2021–2022, from when there was a vaccine up until the immediate future. The results of this study show that the global average inefficiencies in combating the COVID-19 pandemic in countries and regions in 2020, 2021, 2022, and 2020–2022 are 0.602, 0.666, 0.530, and 0.599, respectively, with a significant room for improvement of up to 60%. This result shows that the global dilemma in facing the COVID-19 pandemic is the variety of uncertainties about the occurrence, prevention and treatment, and future trend of this disease. Currently, we can only coexist with COVID-19, and the disease cannot be eradicated until a fully effective vaccine or therapeutic drug can be found. Over time, there has been a continuous rise in the number of COVID-19 infection cases alongside increasing vaccination coverage on a global scale. As a result, countries worldwide are gradually easing social restrictions and control measures. However, as anticipated, SARS-CoV-2 variants are still prevalent, posing a significant risk to older adults and individuals with underlying health conditions who, upon infection, may experience severe symptoms or even fatalities. Achieving global success in overcoming the COVID-19 pandemic necessitates the coordination and cooperation of countries worldwide, while striving for low incidence rates and implementing moderate nonpharmaceutical interventions alongside progressive social and economic policies.58–60
Limitations
This study has certain limitations. First, the use of SFA requires assumptions about the functional form prior to estimation and restricts analysis to a single output item. Second, the data obtained from the IHME were provided by each country and region, which may introduce variations due to the different estimation methods employed. Although the IHME utilized a mixed modeling approach to generate estimated data, there may still be deviations from the actual data. Third, the exogenous variables influencing the COVID-19 mortality rate extend beyond the five variables considered in this study. This study did not focus on the biology or the spread of different variants and its impact on mortality. This study did not analyze or discuss various variant viruses, so future research could explore the inclusion or exclusion of variables to gain further insights. Lastly, the current research methodology may possess some statistical biases, and future studies can explore more effective research methods to replicate the findings. It is anticipated that the outcomes of this study will not only contribute to addressing and improving management of the COVID-19 pandemic but also have potential applications in future large-scale outbreaks.
Conclusions
The empirical findings of this study are consistent in both phases: the more COVID-19 infections, the more hospitalizations required, and the more ICU beds required, the higher the number of deaths. The initial results of the COVID-19 epidemic in Phase I (2020) are as follows: (1) mortality can be reduced with adequate medical services and intensive care in an ICU and (2) bans on large gatherings, lockdown measures, and wearing masks outside the home effectively reduced the number of infections initially. In the second phase (2021–2022), the results are as follows: (1) exogenous variables such as population density, mask-wearing outside, and complete vaccination had no significant relationship with cumulative deaths, indicating that most people already had preliminary antibodies for COVID-19, and the policy of opening borders, lifting lockdown measures, and mask exemption should be conducted gradually. (2) As infection and vaccination rates increase, mortality rates decrease. By measuring the effectiveness of the global response to the COVID-19 pandemic and the results of its impact factors, this study is expected to provide a reference for the community to explore how to reduce and propose countermeasures in order to improve public health policies to mitigate the COVID-19 pandemic. In the future, when faced with a sudden pandemic or health crisis, it can provide global and national policymakers and health units with reference indicators and effective guidance. As humanity faces many unprecedented epidemics and challenges in the future, it is hoped that the world will learn from its mistakes and innovate strategies to improve the response and public health policies while it works together to combat the COVID-19 pandemic.
Footnotes
Acknowledgements
The free software “Frontier Version 4.1” can be used to estimate the equations, which was kindly provided by Professor Coelli. 52
Contributorship
Single author JSW researched and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
This article does not contain any studies with human participants.
Guarantor
JSW.