
Abstract
Background:
Dignity is a cornerstone of end-of-life (EoL) care, particularly in Home Hospice (HH) settings, where most patients wish to spend their final days. Despite HH staff’s crucial role in preserving EoL dignity and their unique challenges, their views of EoL dignity remain underexplored. Moreover, the limited research draws on declarative descriptions, failing to capture the dynamic nature of EoL dignity as embedded in daily practice.
Objectives:
To address these gaps, we aimed to identify EoL dignity values and strategies embedded in HH staff’s narratives on (in)dignity in their daily practice, that is, dignity-in-action.
Design:
Qualitative research using narrative methodology.
Methods:
Drawing on the narrative research paradigm, 17 multidisciplinary HH staff members recounted cases of dignity or indignity in HH. An inductive, holistic content analysis of 32 narratives identified 48 endpoints illustrating (in)dignity incidents. These endpoints were analyzed to determine dignity values and the strategies used to uphold them. Finally, the endpoints were categorized by dignity values, strategies, and relations—who provided (in)dignity to whom.
Results:
The narratives presented HH staff as primary dignity providers, often identifying family members as sources of dignity violations. Dignity was framed around two core values, each upheld by three strategies. Autonomy was maintained by respecting patients’ and families’ preferences regarding care, staff–patient relationships, and coping strategies. Individuality was upheld by acknowledging and respecting the person beyond their patient status, honoring patients’ and families’ unique identities, and acknowledging and respecting patients’ body image.
Conclusion:
HH care presents unique challenges in preserving EoL dignity but also offers opportunities for dignity-centered care. Respecting patients’ and families’ autonomy and individuality through targeted strategies can enhance dignified care. These insights underscore the need to embed dignity-preserving strategies into HH protocols and promote reflective training to heighten staff awareness of dignity violations while reinforcing their strengths in upholding patient and family dignity.
Plain language summary
Dignity is a key part of end-of-life care, especially for people receiving care at home through hospice services. Many patients prefer to spend their final days at home, and home hospice (HH) staff play a crucial role in making sure they are treated with respect. However, we know little about how HH staff understand and uphold dignity in their daily work. This study explored the experiences of HH staff in Israel, focusing on what dignity means to them and how they support it. Seventeen HH professionals from different fields shared real-life stories about dignity and dignity violations. They described 32 cases, which were analyzed to identify patterns. The findings revealed two main values that define dignity: autonomy (allowing patients and families to make choices) and individuality (treating the patient as a whole person, not just someone who is sick). HH staff used three key strategies to support autonomy, such as respecting patient and family preferences, maintaining strong relationships, and helping them cope. They also used three strategies to uphold individuality, including acknowledging the patient beyond their illness, honoring their unique identity, and being mindful of their body image. One important insight was that while HH staff are often the ones protecting dignity, family members sometimes unintentionally violate it. The study highlights the need for training programs that help HH staff recognize dignity violations and reinforce their ability to provide respectful, person-centered care. By embedding dignity-preserving strategies into hospice care, we can ensure that patients and their families receive the compassionate support they deserve in their final days.
Background
In the last decades, Home Hospice (HH) has emerged as an increasingly prevalent palliative care framework in Western countries, responding to most people’s preference to spend their final life phase at home.1,2 A significant characteristic of HH is its effort to maintain end-of-life (EoL) dignity. 3 Dignity, a multifaceted concept encompassing identity, human value, social stance, and ethical action 4 has gained increasing attention in EoL healthcare policy and practice. EoL dignity is considered crucial for maintaining the quality of life and well-being of patients with life-threatening diseases,5,6 given their loss of independence, exclusion from life roles, and damage to self-worth and body image.7 –9
The significance of EoL dignity is varied, depending on demographic characteristics, factors concerning disease and care, 9 religious belief, 10 personhood, spirituality, and culture. 11 Typically, EoL dignity is perceived as a dying process characterized by minimal symptom distress, while maintaining autonomy and independence, being human and being yourself, achieving spiritual goals, having privacy, having self-respect and being respected by others, maintaining meaningful relationships, and receiving dignified care in a calm and safe environment. 9 The latter attributes highlight that EoL dignity is relational and constructed within relationships with others, particularly family members and healthcare professionals.12,13
Palliative care is the primary approach striving to preserve EoL dignity, 9 considering it a fundamental human right for those nearing EoL. 14 Palliative care advocates active, holistic care for individuals facing severe health-related suffering. It aims to improve their quality of life and that of their families and caregivers by alleviating their physical and mental suffering 8 while maintaining their dignity and autonomy. 15 Hospice care, which operates under the broader umbrella of palliative care, focuses on EoL care. The main framework for implementing palliative care is the hospice, which provides medical care, pain and symptom management, and emotional and spiritual support for people at EoL and their loved ones. 16 In the past, hospices existed mainly as inpatient frameworks, but in recent decades, the HH model has expanded in Western countries. 17 This expansion is supported by studies indicating that at EoL the home environment offers unique opportunities for promoting existential and spiritual goals, 18 sustaining hope, 19 facilitating better communication and privacy, 20 and enabling patient involvement in decision-making while supporting daily activities.21,22 At the same time, HH care introduces a unique relational dynamic: professional staff members, unlike in institutional settings, must navigate their dual role as both medical experts and “professional guests” in the patient’s private domain—an interaction that reshapes power dynamics and care boundaries. 23
Inpatient and HHs are operated by a multidisciplinary team, including doctors, nurses, social workers, and often additional professionals and volunteers. Staff in both hospices face complicated challenges in their daily practice, partly involving EoL dignity dilemmas. For example, respecting patients’ wishes when they are against their best medical interest 24 or conflict with family members’ wishes, 25 or when patients’ interpretations of their condition conflict with staff members’ perceptions and dignity-preserving intentions. 26 Alongside challenges faced by both hospices’ staff, HH staff cope with unique challenges and dilemmas embedded in the distinctive characteristics of HH care. Some difficulties stem from HH care being supplied in the patients’ homes, which positions staff members as “professional guests,” entering a foreign territory.17,23 Other challenges pertain to family members constituting clients alongside the patient. The commitment to several clients with different needs and sometimes conflicting care perceptions 27 often results in staff members struggling to accommodate their different expectations. 17 Thus, despite assumptions regarding HH care’s enhanced capacity for preserving dignity, research indicates that maintaining dignity in this setting presents unique challenges. 28
Despite the distinctive challenges and dilemmas involved in HH staff’s efforts to safeguard EoL dignity, their perspectives have not been explored systematically. The few studies on HH dignity have focused on patients’ perspectives,19,29 echoing the general empirical focus on patient perceptions in the study of EoL dignity. The few studies examining professionals’ perceptions found that they relate EoL dignity to preserving patients’ autonomy by respecting their needs, wishes, and independence15,30; providing opportunities for self-definition and expression 30 ; being heard 31 ; and providing physical comfort, respect for privacy, and social relations and communication.30,31 However, these studies do not address how professionals’ perceptions of EoL dignity are embedded in specific care models. Notably, HH staff perceptions of EoL dignity have not been explored.
The present study contributes to filling this lacuna by examining how staff members of an Israeli HH perceive EoL dignity. Understanding the perspectives of HH staff members is essential, given their crucial role in preserving EoL dignity in HH and the unique challenges involved in this effort. This nuanced knowledge is vital to developing appropriate interventions to assist staff in dealing with the difficulties in maintaining EoL dignity in home-based palliative care. The study’s contribution is also embedded in its narrative methodology. By inviting HH staff members to recount stories of (in)dignity openly, we tapped into their emic perspective on EoL dignity, complementing the etic understanding achieved in studies employing predesigned dignity measures. 31 Moreover, unlike qualitative studies that directly asked professionals how they understand the concept of dignity (e.g., Bovero et al. 30 ), we invited participants to tell stories about (in)dignity. Thus, unlike the declarative and more controlled knowledge typically emerging in studies of EoL dignity, our participants’ spontaneous accounts about dignity-in-action 27 inform how dignity is embedded in the staff members’ daily practice.
Methods
Design
The study employs the narrative interpretive paradigm, 28 which underscores the manifold functions of narratives in human life. Narratives (stories) are a unique type of discourse that includes characters, plot-connecting events, temporality or sequence, and consequence, that is, a message or an endpoint. 32 Through storytelling, we assign significance to occurrences, interact with others, and construct our identities.32,33 The reporting of this study conforms to the Consolidated criteria for reporting qualitative research (COREQ) statements (Supplemental Material). 34
Sample
Participants were staff members of an Israeli HH located in a multicultural rural area, which provides care for people with terminal illnesses of different religions in their homes and is funded by health insurance funds. Twenty-one staff members provide weekly symptom management and support visits and are available 24/7 for patients and their families. A request letter was emailed to all staff members, inviting them to participate in the study (Purposeful sampling). Two staff members could not participate in the study due to personal challenges, and 2 of the 19 staff members interviewed did not recount narratives (but, instead, argumentations, such as: “For me, dignity is. . .”), and were thus excluded from the dataset, leaving 17 participants comprising our sample: 5 nurses, 4 social workers, 3 psychologists, 2 physicians, 2 administrators, and 1 thanatologist. The participants were Jews aged 35–81, with diverse professional backgrounds and work experience, primarily women and mostly working part-time (see Table 1).
Participants’ characteristics (n = 17).

Data collection
Individual narrative interviews were conducted by a research assistant with a master’s degree and extensive experience in qualitative interviewing. She was trained and closely supervised by the research team, who developed the interview guide and monitored the interview process throughout. The research team comprised academic experts in qualitative research, ethics, and EoL care, with no prior relationship with the participants.
Each participant took part in a single, face-to-face interview, with no repeat sessions required. All interviews were recorded and transcribed verbatim. At the start of each interview, participants were invited to introduce themselves and describe their role within the hospice. They were then asked to recount a case they had witnessed or experienced that exemplified either dignity or indignity in patient care. If the initial account focused on dignity, they were encouraged to share a contrasting story of indignity, and vice versa. The interviewer maintained a nondirective stance throughout the storytelling process, allowing participants to share rich and uninterrupted narratives. 35 Sociodemographic data were collected following the narrative section.
The interviews lasted between 45 and 60 min. Based on participants’ preferences, 15 interviews were conducted at the hospice office, 1 at the participant’s home, and 1 at a hospital where the participant worked part-time. All interviews were conducted in private, with only the participant and interviewer present.
Data analysis
In the initial stage, we identified 40 narratives in the transcribed interviews. We omitted eight narratives dealing with organizational issues that did not pertain to dignity, thus reaching a dataset including 32 narratives of (in)dignity vis-à-vis patients and/or family members. In the second stage, we conducted an inductive, holistic content analysis 35 of each narrative, identifying its central endpoint(s), 36 for example, I respected the patient’s wishes although they were against my medical appraisal; We changed our intake protocol to accommodate the patient’s wife’s preferences. Most narratives recounted one incident of providing (in)dignity, but some included two incidents, correspondingly presenting two endpoints. Overall, we reached 48 endpoints, each addressing an incident of providing (in)dignity.
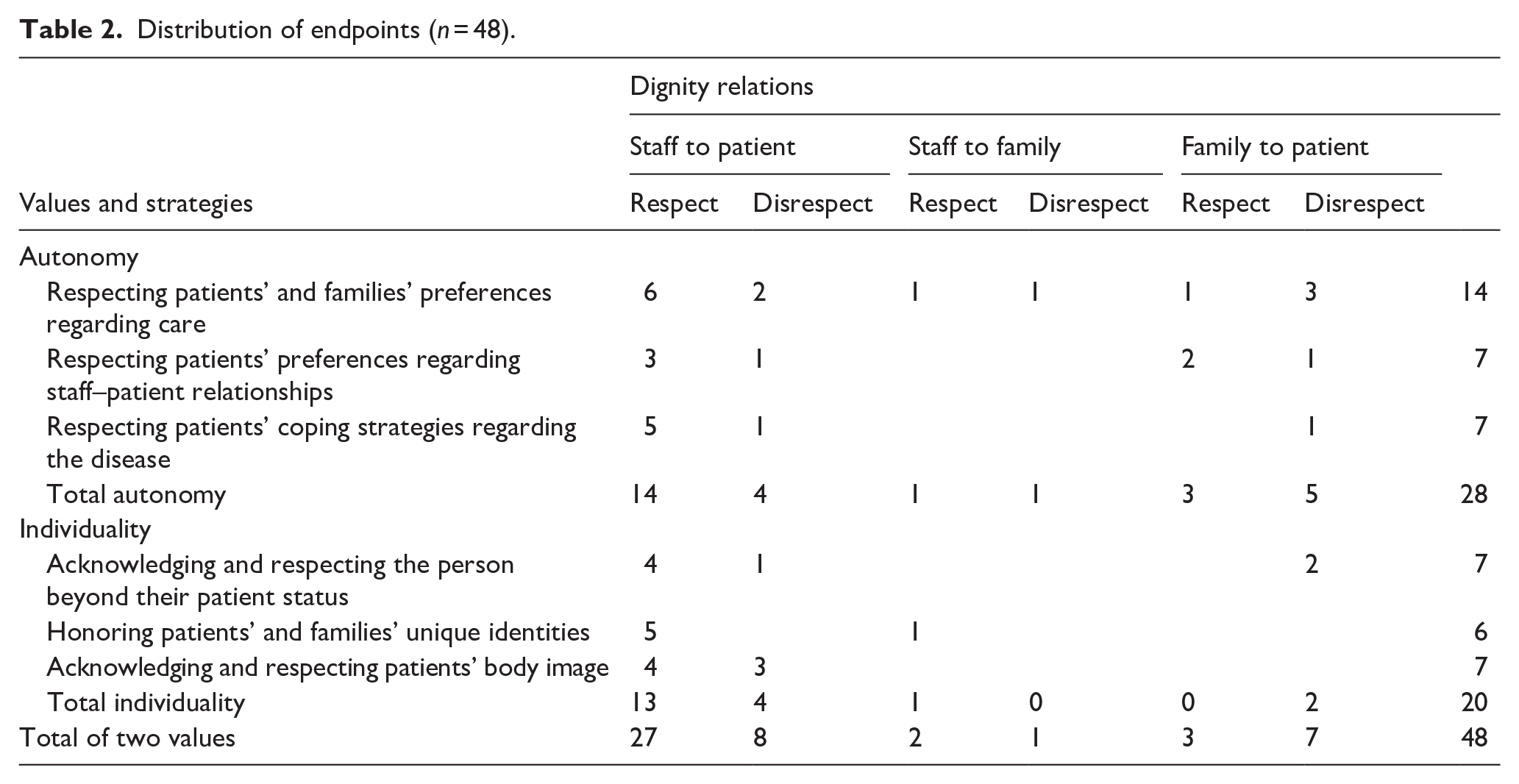
In the third stage, we identified the dignity values and the strategies employed to respect them, as implied by the endpoints. This process resulted in two central values, each comprising three strategies. In the last phase, we categorized the 48 endpoints according to the dignity values and strategies, based on (1) whether dignity was respected or disrespected, and (2) the dignity relations, that is, who provided (in)dignity to whom: staff member(s) to the patient, staff member(s) to the family member(s), or family member(s) to the patient (see Table 2).
Distribution of endpoints (n = 48).
The data collected from staff members provided a comprehensive basis for analysis. Two researchers independently coded the data, and all three researchers contributed to developing the final thematic structure. The analysis was conducted manually, without the use of specialized software. Transcripts were not returned to participants for review, and participants did not provide feedback on the findings.
Rigor and ethics
To enhance trustworthiness, the researchers analyzed data individually and then discussed it to reach a consensus. We applied reflectivity throughout the study to separate our personal experiences and values regarding EoL care and dignity from the findings. The researchers are all women with PhDs, working as researchers and lecturers with expertise in qualitative research, ethics, and EoL care. They have published numerous qualitative research articles and have experience managing complete qualitative research projects on these topics.
Findings
As seen in Table 2, the narratives recounted by the participants reported mainly incidents of respect (32 out of 48 endpoints). This implies that the participants view HH as a setting that respects EoL dignity. Also worth noting is that of the 38 endpoints addressing the staff as (in)dignity providers, 29 showed respect, mainly toward the patient (27), and only 9 demonstrated disrespect. The opposite relationship existed regarding endpoints referring to the family as (in)dignity provider: of 10 endpoints, 3 showed respect and 7 disrespect. These proportions indicate the staff members’ perception of themselves as the primary providers of EoL dignity in the HH, and of the family members as more often disrespecting patients’ dignity. In terms of content, the participants’ narratives depicted HH dignity as comprising two central values: autonomy and individuality, with three strategies supporting (dis)respect each (see Figure 1).

Core values and strategies of end-of-life dignity.
Autonomy
More than half of the total endpoints (28 out of 48) addressed the patient’s autonomy (26), and, to a much lesser degree, that of family members (2). Autonomy is recounted as a central EoL dignity value which concerns patients’ and family members’ right to decide the most appropriate ways to receive care, interact with the staff, and cope with their illness. Of these 28 endpoints, 18 demonstrated respect for autonomy, mainly by the staff (15), and 10 displayed disrespect—5 by the staff and 5 by family members. The narratives in this group expressed three strategies to (dis)respect autonomy: respecting patients’ and families’ preferences regarding care, respecting patients’ preferences regarding their relationship with staff members, and respecting patients’ coping strategies with the disease. A prevalent message of the narratives in this group was that maintaining autonomy often required flexibility and ongoing negotiation, and sometimes creative solutions to balance professional judgment with patients’ and family members’ wishes.
Respecting patients’ and families’ preferences regarding care
Of the six strategies used to respect EoL dignity values identified in the narratives, respecting patients’ and to a lesser degree family members’ preferences regarding patient care was the most frequently addressed (14 endpoints). This reveals its centrality in the staff’s view regarding preserving HH dignity and, possibly, the difficulties and dilemmas often involved in implementing it. Indeed, the three narratives in this group recounted situations when patients’ preferences conflicted with the staff members’ views regarding appropriate medical treatment. These narratives emphasized that respecting patients’ choices often required compromising their professional judgment. For example, one physician noted: “We had to accept her choices and adapt to her way, even though it contradicted all medical logic. She insisted on not using medication that would alleviate her suffering.” Several narratives addressed the emotional difficulty entailed in respecting patients’ preferences in those situations. A nurse described: We experienced a certain conflict because, on the one hand, she was asking for help, but on the other hand, she refused all treatment. At first, it was difficult because we felt helpless seeing someone struggling to breathe and not willing to accept help. But eventually, we understood that these were her decisions.
Despite the challenges entailed in respecting patients’ and families’ preferences regarding care, the narrative’s message was that the staff succeeded in this task (seven endpoints demonstrated respect and only three disrespects). In contrast, family members were portrayed as less able to respect patients’ preferences regarding care, as evident in three endpoints of disrespect and only one of respect. The team described behaviors that did not respect the patient’s wishes by family members. For example, the disrespect that was expressed through not listening to the patient’s wish to die at home and transferring the patient to the hospital, or neglect by family members, and the lack of involvement in care.
Respecting patients’ preferences regarding staff–patient relationships
Five endpoints addressed how staff (3) and family members (2) fulfilled patients’ wishes regarding their relationship with the staff. A single endpoint referred to a situation where family members disrespected such patient preferences. Four narratives in this group recounted situations where patients’ preferences regarding their relationship with the staff could create significant challenges in care delivery, requiring the staff’s creative solutions and adaptations to standard care practices. A nurse recounted a challenging situation where a patient needed treatment but refused to allow the staff to enter his home: The wife was very insistent that we come and provide care. He (the patient) needed us, and she needed us, but he wouldn’t allow us inside the house. Still, it was clear that we had to respect his wishes, and we couldn’t simply say, “Well, if that’s the case, we won’t treat him.” It’s about respecting every person in every situation, even when it makes it very challenging to provide care.
The nurse recounted how the staff created an alternative procedure to the regular intake at the patient’s home by meeting the patient’s wife at a secluded restaurant nearby. This adaptation allowed the staff to provide care while respecting the patient’s preference regarding not having staff members in his home, demonstrating how the staff worked to find solutions that balanced care needs with patient preferences.
Like the staff, family members were portrayed in the narratives as respecting patients’ preferences regarding their relationship with the staff. Two endpoints demonstrate this by describing respect in the decision-making process, characterized by open communication between the family and the care team during treatment in the patient’s home.
Respecting patients’ coping strategies with the disease
Seven endpoints addressed patients’ ways of coping with their illness as a central consideration in maintaining their autonomy. In five endpoints, the staff accommodated these strategies. For example, an athletic patient whose self-image was defined by his athleticism. Due to the illness, he became thin, and his body deteriorated, and he was not willing to let others see him in this situation. The social worker who treated him respected this isolation despite recognizing the social and familial prices the patient was paying, but it was very difficult to respect this choice.
A very athletic patient and suddenly he became thin because of the illness . . . and he wasn’t willing to let people see him, and he essentially isolated himself, even from family members and friends . . . he didn’t want people to see him like that, so we managed here and there a little bit, but it was very difficult.
Another example of this was a patient who hid her body injury due to illness from her family members. The team that treated her respected her wishes by maintaining her privacy. In one endpoint, a patient’s way of coping was disrespected by the staff—a patient who was embarrassed by a mouth deformity caused by the illness chose to cover his mouth with a mask. The team did not respect his choice and asked him to remove the mask because they could not understand what he said when it covered his mouth.
Individuality
The second EoL dignity value that emerged from the staff’s narratives is individuality, which refers to the patient as a whole person with a unique identity and body image. Except for two endpoints where family members disrespected patients’ individuality, all the other endpoints (18) in this group addressed the staff, mainly by providing dignity (13 toward patients; 1 toward family), and, in 4 endpoints, disrespecting patients’ dignity. Through the narratives in this group, staff members confirmed how they consistently worked to respect patients’ and, less frequently, families’ individuality, through acknowledging the person beyond the patient’s status, patients’ and families’ unique identity, and patients’ body image and privacy.
Acknowledging and respecting the person beyond their patient status
Four endpoints demonstrated situations where staff members related to patients as whole persons rather than merely recipients of medical care. This message was evident in a psychologist’s narrative about a patient who suffered genital injury due to illness and refused to receive psychological treatment: I said, what you see as denial, what you see as “doesn’t he understand his condition?,” this is a decision! Truly, an existential decision. You can feel something working there, and if you don’t connect with him, he could shatter into pieces, complete humiliation.
This narrative demonstrates the psychologist’s reframing of what might conventionally be seen as a problematic patient into expressions of individual agency and existential choice. Although this example can be seen as a strategy for coping with the illness, the interviewee describes the patient’s identity component, demonstrating their ability to respect this masculine identity of the patient as a person.
The message regarding the staff’s commitment to seeing patients and families as whole people was evident in narratives of interventions to support family members or mediate between patients and family members. For example, a social worker told a story about the tense relationship between a patient and his children: The father was very opinionated, and the children were very assertive with him. This was the relationship between the children and their father. The staff was very accommodating and tried to mediate while also acknowledging the children’s pain and the father’s demanding nature.
Perhaps most poignantly, the staff’s commitment to acknowledging personhood was demonstrated in narratives about their physical and emotional expressions of care when patients were no longer conscious. An administrative worker recounts an incident she witnessed: The nurse stroked her [the patient’s] face, and everyone around her said, “Mom, they’re going to help you now” . . . She didn’t know what was happening anymore. And the nurse said to her, “Look how much they love you; I can see how much you are loved here.”
This touching account illustrates how staff members maintained human connection through physical touch and verbal affirmation, recognizing that the need for acknowledgment and emotional connection persists even when consciousness fades. These actions reflect a deep understanding that dignity is preserved through maintaining human connections and acknowledging the person’s place within their network of relationships.
Alongside incidents where patients were treated as persons, three endpoints recounted incidents where they were not. By the staff—a patient who wanted to cover his face, and the team did not see the person in the patient and did not respect this request; and by family members—a female patient whose husband was unfaithful to her during her illness, and a patient’s wife who acted angrily toward him due to past resentments.
Honoring patients’ and families’ unique identities
Six endpoints demonstrated the staff’s commitment to honoring patients’ (5) and families’ (1) identities regarding beliefs, cultural background, and legacy. According to the narratives, this commitment went beyond passive acknowledgment, involving deliberate initiatives to capture and respect patients’ and families’ distinctive characteristics, cultural backgrounds, and personal histories. A clear example is a thanatologist’s account of her long-term narrative work with a patient: My listening allowed him to slowly come to himself . . . Throughout the year I accompanied him, a whole spectrum truly opened, of legacy, of heritage, of thinking about so many aspects of life and death, and truly about the family context and the kibbutz context. I documented all these things and eventually reviewed them with him and printed them.
Assisting the patient in constructing his life story, the most explicit expression of one’s unique identity, demonstrates the participant’s active and constant effort to provide the patient with a sense of individuality at the end of his life. Documenting and printing the life story, allowing it to be passed on to family members after the patient’s death, conveys to the patient that his unique identity is valued and deserves symbolic immortality.
Several narratives showed the staff members’ creativity in finding ways to respect patients’ artistic expressions and personal achievements. A powerful example is a psychologist’s narrative regarding the staff’s use of a patient’s artwork to transform her medical environment: She painted this picture. The painting was in her room in the nursing home, and when she returned from the hospital, we hung the painting above her IV. She fell asleep—died—with the needle in her vein and the painting hanging over the IV, hiding the sedative drops and showing the beautiful pastoral landscape she had dreamed of.
A further example of celebrating patients’ unique identity was initiating a public event to recognize a patient’s artistic photographs: “One of the social workers came up with an idea during treatment. Let’s organize an exhibition for the patient. So we collected the patient’s photographs and displayed them at the gala evening” (Administrative Worker).
One endpoint demonstrated respect for the family’s unique identity. When a dying mother of young children was in care, the social worker conducted the farewell in Arabic, the children’s only language. The children drew messages for their mother, and everyone joined hands for a prayer in Arabic. This approach respected the family’s cultural identity during EoL care.
Acknowledging and respecting patients’ body image
Seven endpoints demonstrated the staff’s sensitivity to patients’ body image as central to EoL dignity. These narratives addressed how physical changes and loss of bodily control could profoundly impact patients’ sense of self and dignity, requiring careful navigation between practical care needs and psychological sensitivities. Patients’ body image and privacy were respected in four instances recounted.
In one narrative, a psychologist talked about a patient who needed to be hospitalized. When the ambulance driver came to take her, “I said, ‘Wait a moment’. I asked her daughter, who worked nearby as a beautician, to bring a headscarf. We tied the scarf around her, and only then did I let them come in and take her.” In this narrative, the participant provided dignity to his patient by anticipating and preventing unwanted bodily exposure. The message here is that bodily dignity must be actively protected, not merely respected.
However, the staff’s accounts also revealed the emotional weight of witnessing situations where loss of bodily control profoundly threatened patients’ dignity. A poignant example came from a thanatologist who described the distress caused by a patient’s condition: He smelled of urine, he was wearing diapers that were leaking onto the floor . . . And the staff’s experience was one of distress, real distress. Because it wasn’t that he was completely dependent, but . . . there was an image there of a person losing his dignity.
In this case, the social worker supported the patient, interviewed him, and documented his legacy with the aim of restoring his dignity. This description highlights the empathetic understanding of the participant, who not only cared for the patient but also grappled with the emotional impact of these moments. Another example relating to cultural respect: We made very significant efforts. We brought someone to cook kosher food . . .. And toward the end of her life, when her head covering would fall, we would fix it because we knew it was important to her. After death, too . . . She passed away on Friday. For religious Jews, they cannot take the body until after the Sabbath . . . we placed the body on the floor until after the Sabbath. I went to do the body cleaning, and it wasn’t pleasant after all those hours. (Nurse)
Several narratives addressed challenging situations, when preserving bodily dignity conflicted with essential care needs, requiring staff to carefully balance competing priorities. A social worker described such an incident in one of the three endpoints that presented failure to respect patients’ body image: It was very difficult to understand what he was saying because his entire mouth area was damaged. But he insisted that we shouldn’t see him without the mask. From his perspective, he experienced it as disrespectful when we asked to see him without it. And there was difficulty there because we needed to understand what he was saying and to see.
Collectively, these narratives paint a vivid picture of bodily dignity as a fundamental aspect of personhood, demanding constant attention and protection in EoL care. They reveal how maintaining dignity involves not only practical care but also deep emotional labor, cultural sensitivity, and the navigation of complex interpersonal dynamics.
Discussion
In recent decades, there has been a notable shift in EoL care from institutional settings to HH, aligning with the growing preference of individuals to spend their final days at home.1,2 Central to this transition is safeguarding dignity, which plays a pivotal role in EoL care.4,6 While EoL dignity is widely acknowledged as crucial for maintaining patients’ quality of life and well-being,5,8 its preservation in HH introduces unique challenges. These include navigating the dual role of “professional guests” in patients’ homes 23 —on the one hand, having professional authority given its formal role, but on the other hand, being a visitor in the patient’s home—and addressing the potentially conflicting needs of patients and family members.17,38 Given the limited understanding of how HH staff navigate these challenges to maintain EoL dignity, this study examined how staff of an Israeli HH perceive and uphold EoL dignity. Inviting participants to recount narratives about (in)dignity in the HH enabled us to tap into dignity-in-action, 27 as manifested in daily care practices within the home setting.
The analysis of staff narratives identified two central values as foundational to their perception of EoL dignity: autonomy and individuality. Participants primarily recounted incidents in which they upheld dignity, while fewer narratives described similar behaviors by family members. This suggests that staff perceive themselves as the primary providers of EoL dignity in HH, emphasizing respect for patients’ autonomy and individuality in their daily practice. Conversely, family members were often described as disregarding patients’ dignity, which points to potential conflicts or differences in perspectives on care within the HH setting. These findings offer nuanced insights into how EoL dignity is understood and enacted in home-based care.
Autonomy
The findings demonstrate that autonomy is a cornerstone of dignity in HH care, maintained through three distinct strategies: respecting care preferences, respecting patient–staff relationships, and respecting patients’ coping strategies with the disease. This aligns with existing research, which underscores the vital role of autonomy in preserving dignity in EoL care. 15 The unique context of home care offers both opportunities and challenges for autonomy preservation, particularly in navigating the balance between professional judgment and patient preferences. 22 Healthcare professionals face significant complexities in upholding patient autonomy within HH care. These challenges often arise from the need to mediate between the needs and preferences of multiple stakeholders, including patients, families, and the care team, while adhering to professional standards.32,33,37 Our study reveals that staff members frequently navigate tensions between their professional expertise and patient decisions, particularly when these decisions conflict with recommended medical practices. Flexible approaches and ongoing negotiations are essential in resolving these conflicts, as suggested by previous research. 17
Respecting patients’ relationship preferences within the home care environment adds another layer of complexity. Our findings highlight the importance of maintaining professional boundaries while adapting care practices to patients’ unique relational needs. 23 Adapting to these needs is essential for ensuring that care delivery aligns with patients’ preferences, ultimately fostering trust and preserving dignity in the caregiving relationship. The study also underscores the significance of respecting patients’ coping strategies, even when they challenge conventional care practices. The home setting grants patients greater control over their coping mechanisms, 38 reinforcing their sense of personal agency, a key factor in dignity preservation. 28 Supporting these choices aligns with research demonstrating that respecting patients’ autonomy in managing their illness is integral to dignified care. 31
Individuality
The second value emerging from the staff’s narratives is individuality, which is respected by acknowledging patients as whole persons with unique identities and body images. This aligns with existing research emphasizing the importance of maintaining personhood and individual identity in EoL care, 4 reinforcing the principles of dignified care, which prioritize individuality as an essential component of quality of life 39 and human dignity. 14 Our participants’ narratives further demonstrate that the home setting offers distinct opportunities for preserving individuality, which is less feasible in institutional care. 18
Our participants’ narratives highlight the importance of viewing patients as whole individuals rather than merely recipients of medical care. This emphasis aligns with research highlighting the value of personhood in preserving dignity in EoL care. 12 In the home care context, staff members demonstrated nuanced approaches to reframing behaviors typically seen as problematic into expressions of existential choice and agency. This nuanced approach aligns with the emphasis provided by Nordin et al. 40 and Woodward et al., 32 who argue that acknowledging patients’ autonomy in navigating their illness reflects a deeper respect for their individuality and enhances dignity preservation.
Moreover, staff members often navigate complex family dynamics while acknowledging the interconnectedness of patients’ identities within their relational networks. The home environment enabled staff to balance competing needs and mediate family relationships, reflecting the importance of relational dignity. 13 Staff members were also committed to maintaining human connection through physical touch and verbal affirmations, even when patients were no longer fully conscious. These acts underscore that preserving dignity involves recognizing the person’s presence and role within their family and community, even as physical or cognitive decline occurs.
The study highlights HH professionals’ efforts to respect patients’ and families’ unique personal, cultural, and religious identities. This commitment aligns with research emphasizing the centrality of cultural and spiritual dimensions in EoL dignity. 10 For example, staff engaged in narrative work, documenting patients’ life stories, thus demonstrating respect for their identity and legacy. This process reinforces a sense of self-continuity and belonging, preserving identity during an advanced illness. Home care settings provide distinct opportunities for maintaining cultural and personal identities.27,41 Creative initiatives, such as incorporating patients’ artistic expressions into care settings or organizing exhibitions of their work, exemplify how healthcare providers actively support identity preservation. These practices highlight the role of personal achievements and contributions in reinforcing dignity in HH care.
Bodily dignity and privacy emerged as a further critical aspect of individuality in EoL care. Staff members demonstrated sensitivity to the profound impact of physical changes on patients’ self-perception, recognizing the need to protect their bodily dignity and privacy actively. For instance, ensuring that patients’ appearances were preserved before interacting with others highlights the proactive measures required to maintain privacy and respect.
The findings reveal the emotional toll on staff when witnessing compromises on patients’ bodily dignity. These situations required empathetic responses and creative problem-solving to balance medical needs with dignity preservation. For example, a patient’s request to remain masked poses communication challenges. While staff aimed to respect this preference, dignity was sometimes compromised to prioritize medical well-being. This highlights the complex interplay between bodily dignity and medical care in HH settings, aligning with research on the impact of physical changes on dignity at the end of life. 8
The findings reveal that individuality is deeply interwoven with other EoL dignity values, such as autonomy and relational care. The home environment provides a unique setting where these values can be addressed holistically.42,43 However, it also presents challenges, particularly when gaps arise between staff and patients’ perceptions of dignity-preserving care. 22
Staff members recounted sophisticated strategies used to navigate these challenges, including adapting care practices to individual preferences, mediating family dynamics, and respecting cultural and personal identities. 28 These efforts underscore that EoL dignity preservation is a subjective, relational process, shaped by the interplay of patient autonomy, individuality, and the care environment. 11
Strengths and limitations
While this single-site study with its predominantly female, Jewish staff sample presents inherent constraints, it also offers unique advantages. The small scale allowed for an in-depth exploration of the nuanced ways in which dignity is upheld in daily practice, insights often missed in large-scale quantitative studies. Importantly, by drawing on an inductive narrative methodology, our study offers an emic understanding of dignity-in-action in the HH from the staff’s perspectives. Despite its geographical and cultural specificity, the findings resonate with broader research on healthcare providers’ perceptions of EoL dignity,10,12 while shedding light on its uniqueness in home-based care.
Implications
Home-based care offers both challenges and opportunities for dignity preservation, requiring a balance between professional boundaries and personal spaces. The study highlights the need for comprehensive dignity training programs that foster staff reflection and mentorship, as well as personalized care plans that align with patients’ values and preferences.44,45 Regular team discussions and structured forums for sharing experiences are essential to promoting reflective practices, helping staff navigate the ethical complexities inherent in home care. 46
While staff are adept at identifying instances of dignity preservation, there is a need for increased awareness of dignity violations, especially in their actions. Developing reflective processes can help staff recognize and address lapses in dignity, enhancing their ability to provide dignified care in complex situations. 18 By embedding dignity-promoting practices into care protocols, healthcare organizations can better support staff in recognizing their biases and strengthening their capacity to provide individualized, dignified care in home-based settings. Further potential implication involves hospice organizations offering educational sessions for interested family members on how to uphold principles of personal autonomy and individual dignity. These training opportunities help family caregivers develop skills to respect the patient’s independence and unique identity
Conclusion
Home-based hospice care offers unique opportunities and challenges in preserving EoL dignity. This study highlights that HH staff view dignity as rooted in autonomy and individuality, which they preserve through daily practices. The home setting allows for personalized care not always possible in institutional environments, where staff balance professional expertise with sensitivity to patients’ cultural, religious, and individual needs. These findings emphasize the importance of fostering dignity through holistic, individualized care, ensuring patients’ values and preferences are respected even in complex situations.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251349845 – Supplemental material for End-of-life dignity in Home Hospice: Insights from staff members’ narratives
Supplemental material, sj-docx-1-pcr-10.1177_26323524251349845 for End-of-life dignity in Home Hospice: Insights from staff members’ narratives by Gila Yakov, Gabriela Spector-Mersel and Inbal Halevi Hochwald in Palliative Care and Social Practice
Footnotes
Acknowledgements
We thank the Home Hospice staff who generously shared their time and experiences. We also acknowledge the editorial assistance provided by colleagues at Max Stern Yezreel Valley College.
Ethical considerations
The study was approved by the Research Ethics Committee of the Max Stern Yezreel Valley College (Approval No. EMEK YVC 2021-63).
Consent to participate
All participants provided informed consent to take part in the study. Before the interviews began, participants were informed that the study aimed to explore experiences of dignity and indignity in hospice care from the perspective of healthcare professionals. Participation was voluntary, and confidentiality was assured.
Consent for publication
Participants provided consent for the anonymous publication of the data collected during the study.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Minerva Center for the Interdisciplinary Studies of the End of Life at Tel-Aviv University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.