
Abstract
Background:
The need to improve equity of access to palliative care is well recognized; however, much less is known about how new models of hospice community services can be successfully introduced.
Aim:
We aimed to capture learning from the implementation experiences of hospice stakeholders during the first 12 months of a hospice community services redesign.
Design:
Qualitative research using individual semi-structured interviews (n = 38) and follow-up focus groups (n = 8).
Methods:
Participants were clinical and non-clinical staff, hospice leaders, volunteers, and external stakeholders. Interviews were analysed with framework analysis using Normalisation Process Theory. Focus groups were used to confirm and prioritise recommendations.
Results:
Implementation is more likely to be successful where hospice personnel are enabled to work together in understanding and adapting to new ways of working. Participants gave examples of being supported to plan activities, to form networks of participation, to pilot new ways of working, and to appraise and improve their work. Receiving feedback on progress is beneficial. Implementation strategies that are tailored to each context could be effective if they engage with hospice stakeholders to ensure that strategic aims are well-understood and that the necessary resources are available. Positive experiences of implementation are more likely where stakeholders understand the changes and can participate in planning. Where necessary, changes to human resources and technology support systems would ideally be adopted prior to making changes to patient-facing services.
Conclusion:
This study contributes knowledge from a charitable provider of specialist palliative care during the implementation of a hospice community service redesign. We identified opportunities for future improvement, particularly regarding communication, planning, prioritisation, and feedback. Investment of time and reflection during implementation can support the ambition of hospices to become integrated within a place-based system, to improve access to palliative care within the communities they serve. We report key implementation recommendations for organisations considering service redesign.
Plain language summary
This research explores the process of introducing service changes with the intention of achieving more equitable access to palliative care. The need to improve access to palliative care is well-recognised, however much less is known about how new models of hospice community services can be successfully introduced in practice. This paper is therefore relevant to contemporary issues within the hospice sector, such as movements towards asset-based community development and partnership working. Our study aimed to understand the experiences of hospice personnel during the first twelve months of an ambitious hospice community services redesign. We used qualitative methods to collect data from clinical staff, non-clinical staff, volunteers, the hospice leadership team, and external stakeholders. Analysis was informed by an established theory from implementation science – Normalisation Process Theory (NPT). The findings and recommendations contribute valuable learning on how the four mechanisms of implementation can be achieved (or not); these are coherence building, cognitive participation, collective action, and reflexive monitoring. Successful implementation happens when hospice teams can collaborate, adapt to changes, and receive support and feedback. Tailored strategies that ensure clear communication and proper resources help staff to understand and embrace the changes. We consider this research to be of interest to palliative care providers, especially those who are considering or engaging in service improvement.
Introduction
The United Kingdom’s population is ageing, 1 with increasing demand for palliative and end-of-life care. 2 Disease prevalence models have suggested the palliative and end-of-life care needs in England and Wales may increase by between 25% and 42% by 2040. 3 Within 20 years, over 100,000 more people will be dying each year in the United Kingdom. 4
Due to increasing healthcare pressures and inequalities, the National Health Service (NHS) Long Term Plan (2019) advocates that care should move ‘to a new service model in which patients get more options, better support and properly joined-up care at the right time in the optimal setting’, 5 outlining how a place-based system of care could be provided by NHS Integrated Care Alliances across England. 6
Personalisation of patient care within different community contexts is challenging and requires careful planning. Every community has its own unique context, including geography, history, population demographics, and its own asset-based community strengths, such as resources, voluntary organisations, charities, and community groups. 6 Hospices play a vital role, leading the provision of palliative care in the community and improving access within a place-based system. However, for many, this requires a rethink of current care models and service delivery.
This study was conducted at a hospice that provides specialist palliative and end-of-life care across a 700 square mile region in South-West England. The mission of this hospice is ‘to ensure everyone has access to outstanding palliative and end-of-life care’. 7 In 2019, the hospice identified that it was unlikely to meet this aim with its existing service model. Using the Marie Curie End of Life Care Atlas, 8 it was estimated that the hospice could be reaching only half of the people with palliative care needs in the region. The experience of the hospice echoes palliative and end-of-life care nationally and internationally – access to palliative care often falls short of the level of palliative care need.4,9 –12
With integrated care systems (ICSs) and place-based partnerships, hospices are encouraged ‘to do things differently’. 13 Thus, the hospice set out to re-imagine its model of care, implementing a multi-faceted redesign of hospice services to strengthen specialist palliative care provision within the communities they serve. Translating the new model of care into operational reality required substantial procedural and social changes, involving people at all levels of the hospice organisation. NHS system-level restructures during the formulation of the ICSs, coinciding with the COVID-19 pandemic, magnified both the urgency of change and the complexity of change management. Existing research indicates that implementation could have challenges, including difficulties in keeping both staff and volunteers informed and ‘bought-in’ when services are changing. However, such research is sparse, and there are limited insights about the experiences and processes through which a hospice can successfully manage the change required to redesign its services.14 –16
This study aimed to explore and understand the experiences of hospice stakeholders (hospice leadership, clinical staff, non-clinical staff, volunteers, and external stakeholders) when implementing the redesign of community services. The research question asked: what worked well and less well during the implementation of the hospice service redesign, and why?
Methods
Methodology
This study sought to explore and understand the experiences of hospice stakeholders. Whilst quantitative data can describe implementation outcomes (e.g. number of patients cared for), exploring and understanding experiences required qualitative inquiry that engaged with the people involved ‘on the ground’. Using a qualitative approach, this research was conducted within a realist paradigm, which appreciates that individual knowledge is subjective, while recognising a stratified reality in which events are caused by mechanisms leading to identifiable patterns across society. 17
Normalisation Process Theory (NPT) is a theory from implementation science, which ‘identifies, characterises, and explains mechanisms that have been empirically demonstrated to motivate and shape implementation processes and affect their outcome’. 18 NPT therefore explains the ‘work’ involved in implementation. 19 NPT has been applied to implementation challenges in palliative care20 –22 and is widely used in other healthcare settings. 23
Research characteristics
The research team included expertise from nursing, health psychology, and organisational psychology. K.S. was initially employed for project activities, and N.B. was based at an external university, neither had existing relationships with study participants. These team members led on data collection to minimise the potential impact of social desirability on participant experience.
Study context
The hospice is an independent charitable provider of specialist palliative and end-of-life care in a mostly rural region of South-West England. Following on from a 2-year service review (‘The Listening Project’), a new and decentralised model of care was designed to achieve five specific goals: care for more people; closer to home; provide earlier support; easier access; and enable compassionate communities.
Implementation was planned to occur in two phases, with phase I commencing in April 2022. Phase I involved eight discrete projects (Table 1). Each project was managed by a Task and Finish Group, the leads of which also contributed to an Operational Delivery Group. A Vision Delivery Programme Board oversaw the programme. Implementation began in April 2022, and this study explored stakeholders’ experiences over the following 12 months.
Project streams comprising phase I of the hospice community services redesign, aims, and brief description of how this differed from the previous service model.

NHS: National Health Service.
Stakeholder engagement
The research team collaborated with the hospice user group (HUG), consisting of four hospice volunteers, with various roles including driver, administration, and organisational support, bereavement support, and companion. HUG meetings introduced the research project, explored the appropriateness of the research question, and engaged in an open discussion around the research project’s aims, design, scope, and proposed timeline. The HUG provided insights which informed the recruitment strategy (e.g. diversity in perspectives), qualitative data collection (e.g. importance of confidentiality and sensitivity addressed through one-to-one interviewing format), and endorsed the potential benefits the research findings could bring for the hospice and its wider community.
Participant selection
Recruitment began in January 2023. We used purposive sampling to incorporate a range of perspectives on the implementation, for example, variety of professional roles, across different managerial levels, working in different geographical locations, and delivering different hospice services. Potential staff participants were approached directly by K.S. and N.B. via professional work email addresses. The research team also publicised the study and invited participants interest via a written news feature published on internal communications and a presentation during a monthly ‘Coffee break’ meeting for all staff and volunteers.
Ethical considerations
Eligible participants were English-speaking, aged 18 years or older, willing and able to give informed consent for participation, and either previously or presently aligned with one of the stakeholder groups (hospice leadership, clinical staff, non-clinical staff, volunteers, external stakeholders). The hospice is a small organisation, as such, personally identifiable details and demographics are not reported to protect participant anonymity.
Participants were provided with a participant information sheet, privacy notice, and consent form, and given the opportunity to consider this information and ask questions before agreeing to participate. Participation was entirely voluntary, and informed consent was obtained from all participants prior to the interview. Ethical approval for this project was granted by the University of the West of England’s Faculty Research Ethics Committee.
Data collection
Data collection occurred between January and June 2023. For the qualitative interviews, a semi-structured interview guide was developed, informed by the domains of NPT, and tailored to different hospice stakeholder groups (Supplemental File 1). This included open-ended questions relating to participants’ experiences of the implementation and their ideas about how and why this happened for them and their team.
Interview guides were pilot tested with two clinical and one non-clinical staff, and revisions were made to enhance clarity. Interviews were conducted by K.S. and N.B., either in-person or via video call, according to participant preference. Subsequently, participants were invited to optional focus groups, which aimed to involve stakeholders in the process of interpreting our findings and prioritising recommendations.
Data processing and analysis
Interviews were recorded and transcribed verbatim using a professional transcription service. Transcripts were anonymised by K.S. prior to data analysis in Lumivero NVivo V.12. NVivo ‘memos’ were used to capture reflections on how the hospice context shaped implementation mechanisms, and how this led to outcomes based on the participants’ direct and indirect experiences
We used NPT as a theoretical framework to explain the process of implementation and applied a coding manual developed for the application of NPT to qualitative data. 19 The coding manual provided a rigorous and consistent analytical approach for the conceptualisation of mechanisms within this study, by defining 4 core constructs (coherence building, cognitive participation, collective action, and reflexive monitoring) and 16 secondary constructs.
Data analysis and researcher reflections were discussed in weekly meetings with the research team. The researchers (K.S., N.B., A.L., C.P., C.S., C.M.) also held two team workshops in April and May 2023, using interview excerpts to interrogate developing insights into the interaction between hospice context and implementation mechanisms. Additionally, three follow-up focus groups were then conducted with participants (led by K.S. and C.S.) to validate our interpretation of the data and to prioritise areas for improvement (recommendations).
Results
Fifty individuals were approached for interview, 38 participated (n = 38). Reasons for non-participation were no response, retirement, and workload. An overview of participants is shown in Table 2. Interviews were conducted online (n = 25) and in-person (n = 13). Additionally, eight participants attended one of the follow-up focus groups, these were hospice leaders (n = 4), clinical staff (n = 1), and non-clinical staff (n = 3).
Interview participants.

Those marked with an asterisk (*) also participated in a focus group.
Implementation mechanisms are defined as ‘the work that people do when they participate in implementation processes’, they include coherence building, cognitive participation, collective action, and reflexive monitoring (p. 1)’. 19 Findings are presented below, to explain how each of these four implementation mechanisms relate to the hospice context, accompanied by tables with extracts from interview data.
Coherence building
Coherence building considers how people work together in everyday situations to understand and plan the activities that need to be accomplished for implementation of the service redesign 19 (Table 3). Findings support the importance of differentiation (distinguishability of new ways from current ways of working) and specification (agreement about the purpose of the intervention and each individual’s role) as important components in building coherence.
Extracts from interviews related to coherence building (working together to understand and plan activities).

Most participants indicated that the goals of the community service redesign, especially ‘caring for more people’, were well-understood and could be differentiated from earlier, more centralised, approaches to care – this aspect of the implementation worked well for these individuals. However, at the time of data collection, there was occasional inconsistency in the understanding of the driving forces behind the changes (e.g. current unmet need, future population challenges, changes to commissioning structures). The purpose and efficacy of the proposed changes were therefore ambiguous for some participants, who were also unclear on the derivation of strategic targets (e.g. to care for 5500 patients per annum by 2025), the specific details of how the service redesign would be delivered in practice, and how this would lead to targets being achieved. Staff who were uncertain about the pragmatic utility of these targets were less able to internalise the value of the new service model.
Staff who had already experienced a significant amount of change in their team, or who were in new roles, appeared to have a greater sense of coherence and understanding of the potential benefits of new ways of working. For example, clinical staff specified how their work assessing self-referrals, booking patients into palliative care clinics in the community, and participating in the joint specialty clinic was widening palliative care access, and therefore benefitting patients. Volunteers recognised how their input to strengthening relationships with social prescribing in the community was releasing capacity for clinical staff to deliver their work. There were instances in which specification (both individual and communal) was less apparent, which had ramifications for some staff being less able to collectively agree with the changes and understand what its components required of them.
Some participants had a well-developed sense of coherence and had internalised the value of the new ways of working. Others had experienced instances in which communication was perceived to be intermittent, rushed, or vague. This could be related to an organisational strategy that involved a top-down cascading of information, and as such did not work well for everyone. One of the most cited examples of disconnect was from a small number of established staff who described not understanding the new roles and skill mix introduced to community teams.
Cognitive participation
Cognitive participation considers how people work together to create networks of participation 19 for the implementation of the community service redesign (Table 4). Findings suggest ways in which initiation (how key individuals drive change forward) influenced the degree of enrolment (how others join in). Legitimation and activation (how people agree with the intervention and continue to support it) were constrained by aspects of the organisational and wider context (e.g. limited meeting rooms and a backdrop of intense pressure on the healthcare system may have reduced the space and time available for cognitive participation).
Extracts from interviews related to cognitive participation (working together to create networks of participation).

MDT: multi-disciplinary team.
There was a mixed response from participants about how they had experienced initiating the community service redesign. Delivering critical community services alongside the implementation of the service redesign introduced conflicting priorities for some participants. Participants worked collaboratively, relying on close working relationships within their teams to understand and adapt to new ways of working. Some of these individuals reported that a lack of time and headspace impacted their ability to continuously focus on and enrol others in delivering a new community service.
Most participants agreed that aspects of the training that had been introduced to initiate the community services redesign had not worked well. Undertaking additional professional development tasks, such as lengthy training sessions and assignments, was associated with challenges in fulfilling commitments to clinical care. These individuals perceived professional and moral obligations to prioritise high-quality patient care in a context of increasing patient referrals, which held them back from legitimising the new ways of working.
Cognitive participation may have been disadvantaged by a shortage of physical spaces for in-person meetings, because of the closure of community outreach centres and low availability of meeting rooms in the main office building. The lack of physical spaces impeded supervision sessions, professional development reviews, recruitment, and training activities, which are essential for onboarding and supporting new or less experienced staff. This created extra work due to the time and effort spent locating, communicating, and co-ordinating spaces to meet. Volunteers also described frustration that they were unable to find a physical space at the hospice.
When physical spaces were available, these enabled activation and legitimisation. For example, staff without a healthcare background had no formal training to understand clinical roles and medical language, which occasionally hindered communication between clinical and non-clinical staff. However, multi-disciplinary team (MDT) meetings provided beneficial learning opportunities for bridging knowledge gaps between clinical and non-clinical staff (e.g. clarifying policies around help with medication when supporting patients in their homes). Physical spaces can function as a ‘home’, offering staff opportunities for knowledge sharing, team bonding, and social support.
Collective action
Collective action considers how people work together to enact the community services redesign 19 (Table 5). Findings indicate that interactional workability and relational integration were especially relevant to the hospice teams, underpinned by a high degree of respect for each other and a shared moral impetus to care for patients and families.
Extracts from interviews related to collective action (working together to enact the components of the redesign).
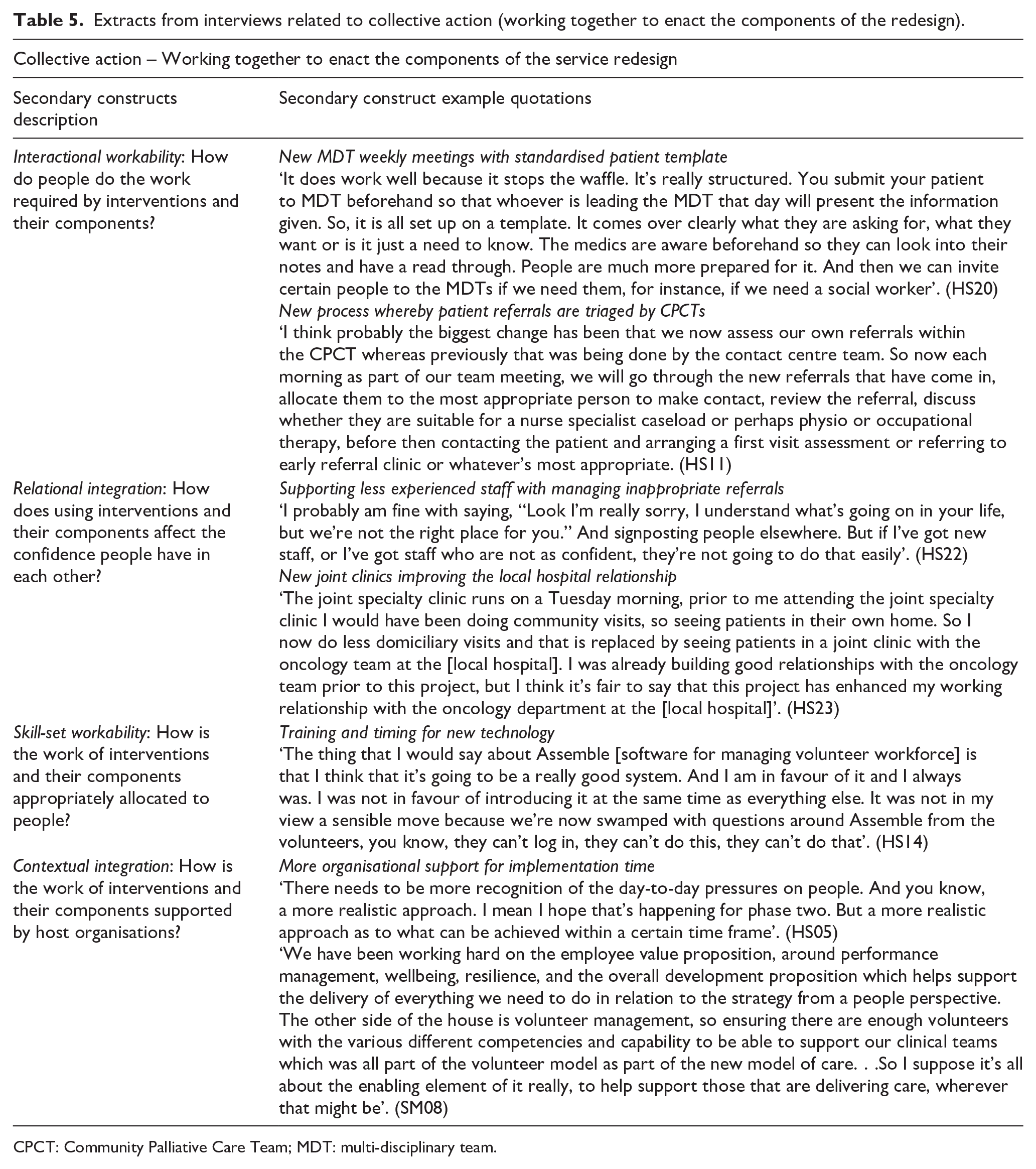
CPCT: Community Palliative Care Team; MDT: multi-disciplinary team.
Collective action relies on close teamwork, both within and across hospice teams. Successful examples of interactional workability included the introduction of multi-disciplinary team meetings for the assessment of new and complex patients, alongside a standardised template for presenting patient information. This allowed staff to communicate and prepare for patient assessment in a structured and efficient manner.
The process for triaging new referrals was also changed, so that this assessment was now being carried out by the Community Palliative Care Team (CPCT) operating in the same locality as the patient being referred. The CPCTs would allocate referrals to different staff according to their skills, availability, and locality; supported by a process to safely redirect inappropriate patient referrals and to discharge patients. This worked well for some clinical staff. Less experienced or new team members were not as confident in redirecting referrals to alternative organisations, requiring support from their wider team to make and communicate these decisions. This suggests that relational integration and skill-set workability can be interconnected and developed over time, particularly as new staff roles are becoming established.
The introduction of new information technology as a component of the service redesign was challenging in some situations (e.g. volunteer workforce management software ‘Assemble’). The aim of Assemble was to assist with collective actions such as onboarding new volunteers, allocating tasks, managing expenses, and communicating. Despite acknowledging the value of this tool, volunteers and non-clinical staff reported investing significant effort towards the workability of the new software. Challenges were experienced when training others and sustaining practices around Assemble, especially when this technology did not function as expected.
Hospice leaders were keen for the organisation to support all clinical and non-clinical staff and volunteers, enabling them to deliver palliative care to more patients in the community through substantial investment in new roles and staff. Participants emphasised the significance of ensuring sufficient resources, for example, by having realistic apportioned staff time allocated to focus on and enact the implementation work in addition to clinical service delivery. Responding to healthcare system pressures while allowing for the time taken to develop new staff skills contributed to contextual integration (e.g. by adapting implementation timelines).
Reflexive monitoring
Reflexive monitoring considers how people work together to appraise the community services redesign 19 (Table 6). Reflexive monitoring, where present, was indicated by a feedback loop that helped to drive continuous improvement; however, this construct was the least well-developed in our findings, possibly due to the timing of our investigation.
Extracts from interviews related to reflexive monitoring (working together to appraise the service redesign).

Staff and volunteers engaged in reflexive monitoring during everyday conversations and were keen to hear how implementation was being evaluated at the organisational level. Hospice leaders recognised the importance of sharing the progress of the community service redesign ‘journey’ with clinical and non-clinical staff, volunteers, patients and families, and trustees and commissioners. Experiences during the first phases of implementation led to an intended reconfiguration of some activities in the future, including an increased focus on pilot testing and the provision of project management training.
Available outcome data (e.g. number of patients cared for) were included in hospice communications to demonstrate the benefits of the community services redesign and bolster confidence that progress was being made. Participants described how new technologies (Microsoft Power BI) for monitoring and reporting outcome data also enabled systemisation of reflexive monitoring of the community services redesign. Power BI would track team outcome data against set targets highlighting where targets had not 100% been achieved. However, for some clinical staff, achieving an 80% target was interpreted as ‘poor’ team performance and this experience was demotivating, leading them to question whether targets were realistic.
Outcomes evidenced an increase in investment expenditure for the community services redesign and an increase in total patients cared for, but not yet at the rate necessary to meet strategic targets. However, hospice leaders and clinical and non-clinical staff held a degree of uncertainty concerning the appropriateness of outcome measures instituted, which reduced their confidence in them as a tool for appraisals. For example, they reported they had been unsure whether outcome measures were sufficiently able to capture patients being reached through the extended settings in which they were now delivering services (e.g. joint specialty clinics within an NHS hospital), or on the extent of cultural changes within the organisation.
Discussion
This research explored what worked well and less well during the first 12 months of implementation of a hospice community services redesign. The project took place in a single hospice organisation, which was disrupted during the study period by the ongoing COVID-19 pandemic, financial pressures, NHS system-level restructures, and a challenging labour market. However, it is unlikely that any implementation of service redesign would occur in a wider context that was resolutely stable. We therefore conducted a ‘deep dive’ into this single hospice to reveal useful insights. The following paragraphs discuss these insights which other organisations may wish to consider when contemplating significant change to service design. These relate to communication, planning, prioritisation, and feedback.
We utilised NPT as a theoretical framework to identify implementation mechanisms. In line with previous findings,20,24 the use of NPT helped to reveal that collective action depends on coherence-building and cognitive participation. Existing implementation research of relevant models, such as compassionate communities, tend to focus on the later stages of implementation but stakeholder engagement and mobilisation are essential development stages. 25 An increased emphasis on coherence building and cognitive participation might have alleviated some of the challenges experienced during the community services redesign, in that these constructs could provide a fundamental foundation for the collective action required to create new ways of working.
Effective organisation-wide communication is essential – even fully staffed and skilled teams cannot ‘hit the ground running’ without first understanding the new services. Consistent communication could prevent misunderstandings emerging via the ‘rumour mill’. Conflicting attitudes within an organisation indicate that sense of coherence was insufficiently established. 26 Findings from elsewhere indicate that hospice staff can be apprehensive towards change, because strategic shifts away from a traditional service model may be contentious, without a shared agreement on what is feasible or desirable to achieve with the new model. 27
Collective action is facilitated through careful prioritisation of activities. The availability and adequacy of human resources and the technology required during the implementation period are commonly reported factors influencing successful change in healthcare. 28 Implementation and adoption of support systems required for new care models and community services (e.g. new technologies, upskilling staff) should occur prior to the introduction of the ‘patient-facing’ changes to service delivery. Sufficient time could be designed into implementation timelines to allow for a comprehensive understanding of necessary processes, including informal or ‘workaround’ processes that might not be obvious to those outside the team.
Findings highlight that the provision of in-person opportunities to conduct collaborative work encourages participation in change programmes. A dedicated online space to provide information, news, achievements, and feedback about the change programme could also have been valuable. These aspects became more apparent when reflecting on the impact of disruption related to COVID-19. Informal support between hospice team members and formal support from NHS clinical teams were interrupted during the pandemic, increasing the pressure on individuals. The timeline of service reorganisation after this experience could have contributed to reluctance from some staff to participate in the change process.
Decision-makers should aim to balance pace of change and capacity for change, recognising that resilience and leadership are important characteristics for those being asked to adapt their daily practices and professional roles. Implementation activities can become sidelined when working environments or team composition are unstable, because staff may prioritise ‘just getting through the day’. 29 The psychosocial challenges of change management can be anticipated and planned for to some extent, for example, considering when and how individuals can gain support from peers.
Working relationships with external organisations are crucial to place-based care and take time to develop. Sustainable and balanced partnerships with community organisations are enabled through shared ownership of projects, but this can be challenging to some service providers who are less familiar with a facilitator role. 25 Hospice volunteers can strengthen links to local communities, forging stronger community involvement where this aspect of their role is adequately supported and recognised. 30
The appraisals made by hospice staff about a particular programme will inform their current and future attitudes to change. These may not be immediately visible to hospice leaders and decision-makers, underscoring the importance of two-way communication. Leaders who demonstrate they are receptive to feedback will maintain opportunities to listen to, learn from, and in some cases resolve concerns. Identifying and resourcing formal ‘change champions’ 31 within teams may be helpful for maximising the exchange of information and proactively engaging with staff and volunteers. Others report actions to recognise and reveal ‘brilliance’ within palliative care teams as helpful to encourage continued engagement in quality improvement. 32
This investigation was conducted after the first year of an ambitious service redesign. Coherence-building, cognitive participation, and collective action were highly relevant to the data collected. The primary construct of reflexive monitoring was less frequently indicated. This could be due to the context of continued change captured in the study period, in that it was too early for teams to feel the benefit of their efforts because the implementation was not fully complete at the time of this research.
It appears that the four primary constructs in NPT are more important at different times – coherence and participation ‘set the scene’ for understanding and changing ways of working. As a new intervention becomes embedded and normalisation is underway, the work involved becomes more about refining plans and assessing progress. We interpret this as a cycle, rather than a linear process, because reflexive monitoring of existing ways of working underscores the perceived value of change. In this example, the challenge of achieving coherence towards the service redesign was amplified in situations where staff were not fully cognizant of the limitations of the existing model of caring services.
Key recommendations
Staff need to have the capacity (time and mental energy) to engage with internal communications before they can understand the change programme and how it affects their role.
Consistent communication about how the change will be implemented enables different stakeholders to share an understanding of what is happening, why it is happening, and when it is happening.
Staff who have physical spaces to bond with their team have more opportunities for knowledge exchange, experience sharing, and social support, to build their identity within the change programme.
New technologies or work processes should be piloted prior to widespread launch, establishing a clear process and contact person for technical assistance.
Leaders who recognise and celebrate staff progress, and who listen to negative feedback, contribute to supporting a culture of learning and continuous improvement.
Strengths and limitations
Participants were recruited from a single hospice providing specialist palliative and end-of-life care in England. We recruited a heterogeneous cohort of participants with a diverse range of experiences, across all the hospice teams directly affected by the community services redesign. Recruitment was partly impeded by the availability of clinical staff operating during winter pressures. The number of external stakeholders (n = 2) was also limited due to difficulty in identifying and engaging with relevant individuals during the study timeframe.
Whilst we set out to understand the impact on hospice staff, volunteers, and external stakeholders, we did not seek out the views of patients. The patient group receiving care during the implementation of the services redesign would be unlikely to be familiar with the organisation of care prior to this implementation, and not exposed to the activities designed to instigate changes. As a hospice, we routinely collect patient satisfaction data to monitor patient and client satisfaction, which could provide additional insights once the service redesign is established.
The study demonstrates the utility of NPT for implementation research in this sector. NPT was used as a framework for coding the primary data, but our methods also allowed for unexpected concepts to emerge in the interviews and during reflective discussions with the research team.
This study focuses on the early stages of implementation (first 12 months), which might not have allowed adequate time to capture normalisation in everyday practice. Future investigations into the later stages of the implementation could substantiate or extend current findings. Further research could extend the application of implementation science to hospice care by developing and evaluating effective implementation strategies. Participatory action research could also be valuable in bringing about large-scale change by developing the capacity of stakeholders to participate in the process. 31
Conclusion
In this research, we aimed to learn more about how and why the implementation has impacted on stakeholders and to capture learning about how hospices can transform their services to reach more people. Our findings identified the challenges of implementing change within a hospice setting but importantly also highlighted opportunities to improve in future initiatives. We recommend particular attention to communication, planning, prioritisation, and feedback. Reflexive monitoring of existing service models could be the starting point of building coherence towards proposed changes. Implementation strategies should be designed with an understanding of the unique contexts of service provision and recognise the substantial and varied ‘work’ involved in making changes.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251349839 – Supplemental material for Implementation of a hospice community service redesign: Qualitative research identifying lessons learned
Supplemental material, sj-docx-1-pcr-10.1177_26323524251349839 for Implementation of a hospice community service redesign: Qualitative research identifying lessons learned by Kate Sugar, Candy McCabe, Alison Llewellyn, Wayne de Leeuw, Maggie Crowe, Claire Prendergast, Charlotte Spence and Natasha Bradley in Palliative Care and Social Practice
Footnotes
Acknowledgements
We wish to acknowledge the valuable contribution from all the participants and the Hospice User Group who supported this research – thank you. Preliminary findings have been presented as posters at the Hospice UK Conference 2023 and Marie Curie Research Conference 2024, abstracts were published in BMJ Supportive & Palliative Care Nov 2023, 13 (Suppl 5), A96, DOI: 10.1136/spcare-2023-HUNC.249 and BMJ Supportive & Palliative Care Jan 2024, 14 (Suppl 1), A3–A4, DOI: 10.1136/spcare-2024-MCR.7.
Ethical considerations
Ethical approval for this project was granted by the University of the West of England’s Faculty Research Ethics Committee on 16th December 2022 (Reference number: HAS.22.11.034).
Consent to participate
All participants provided written informed consent prior to participating.
Consent for publication
Written consent obtained directly from participants.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Education & Research team at Dorothy House Hospice obtained internal funding for this research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors except N.B. were employed by the organisation which conducted the research. K.S. was employed to carry out the research and had no prior involvement with the organisation.
Data availability statement
The data supporting the findings of this study are not expected to be made publicly available – due to the qualitative nature of the study it would not be possible to ensure anonymity of the data. The authors do not have ethical approval or participant consent to share the full dataset.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.