
Abstract
Background:
Community-based palliative care (CBPC) shows promise for supporting patients with advanced noncommunicable diseases, yet implementation remains inconsistent. Most research focuses on organizational and provider perspectives, with limited understanding of patient and caregiver views on service acceptability and implementation.
Objectives:
To understand barriers and facilitators to implementing CBPC services from the perspectives of patients with advanced congestive heart failure, chronic obstructive pulmonary disease and end-stage renal failure, and their primary caregivers.
Design:
Qualitative study using focused open-ended interviews conducted over four-monthly intervals. Data were analysed using reflexive thematic analysis within a critical realist paradigm.
Methods:
Twenty-five patients (11 male, 14 female; 13 CHF, 8 ESRF, 4 COPD) and 9 caregivers (1 male, 9 female) were recruited from the Segamat district in Malaysia. Participants met inclusion criteria using the Supportive and Palliative Care Indicators Tool. One-on-one open-ended qualitative interviews using the reflexive thematic analysis approach explored experiences of living with advanced illness, perceived needs and perspectives on establishing CBPC services.
Results:
Four key themes emerged: “What they offer is not what we need” revealed skepticism towards new healthcare services based on negative past experiences; “Supportive relationships over support services” demonstrated preference for care from trusted community members rather than outsiders; “The myriad cares of family” highlighted the valued role of family caregivers in providing companionship and maintaining patient identity; and “How to care for us” identified unmet needs including transportation, financial support and social connection. Participants emphasized that trust-building through community engagement must precede service implementation.
Conclusion:
Successful CBPC implementation requires fundamental shifts from expert-driven service delivery towards relationship-centred, community-engaged approaches. Services must be co-developed with communities, prioritize trust-building and address social determinants of health alongside clinical needs. Traditional “build it and they will come” approaches are insufficient for achieving community acceptance and sustainable implementation.
Plain language summary
Many people living with serious long-term illnesses like heart failure, lung disease, and kidney failure need extra support to manage their symptoms and improve their quality of life. Healthcare systems are trying to provide this support through community services that help people stay at home rather than going to hospital. However, these services often struggle to get started or don’t work well in practice. We wanted to understand why this happens by talking directly to patients and their family caregivers. We interviewed 25 patients and 9 family members in rural Malaysia over several months to learn about their experiences and what they thought about having new healthcare services in their community. What we found was surprising. Even though these families clearly needed help, many were skeptical about new healthcare services. This wasn’t because they didn’t want support, but because they had bad experiences with healthcare in the past. They felt that doctors and nurses didn’t understand their daily struggles and offered advice that wasn’t practical for their real lives. Instead of wanting professional services, people preferred help from family members, friends, and neighbors they already knew and trusted. They valued relationships over services. Family caregivers didn’t want to be replaced by professionals – they wanted support so they could continue caring for their loved ones. The families told us that if healthcare providers want to help, they need to first build trust in the community. This means getting to know people, participating in community events, and working with local leaders. They also need to address practical problems like transportation to medical appointments and financial struggles, not just medical symptoms. Our research shows that successful healthcare services must be built with communities, not just for them. Trust and relationships matter more than professional expertise alone.
Keywords
Introduction
The global burden of chronic, life-limiting illnesses continues to grow at an unprecedented rate, creating new challenges for healthcare systems worldwide. Noncommunicable diseases (NCDs) such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD) and end-stage renal failure (ESRF) account for a significant proportion of mortality and morbidity, particularly among ageing populations. 1 These progressive, non-malignant conditions present complex symptom burdens that often rival those experienced in cancer, yet historically have received less attention in palliative care research and service provision.2,3 As healthcare systems evolve to address these changing demographics and disease patterns, there has been increasing recognition of the need to shift care delivery from traditional hospital-centric models towards community-based approaches that better align with patient preferences and system sustainability. 4
Community-based palliative care (CBPC) has emerged as a promising model to address these challenges, offering specialized support focused on quality of life, symptom management and psychosocial well-being for individuals with serious illness while they remain in their home environments. 5 The potential benefits of such services are well documented: reduced emergency department visits, decreased hospitalizations, improved symptom management, enhanced quality of life and greater alignment with patient preferences regarding place of care and death.6,7 Despite these advantages, the implementation of CBPC services remains inconsistent and fragmented across healthcare systems, with significant variations in access, quality and integration with existing healthcare services.8,9
Current state of CBPC
Research examining CBPC has grown substantially over the past decade, with increasing evidence supporting its clinical and cost-effectiveness.6,7,10–12 From a health system perspective, well-implemented CBPC programs have shown potential for reducing healthcare utilization and costs, particularly through decreasing hospital admissions and emergency department visits in the last months of life.13,14
However, the successful implementation of CBPC services has proven challenging across diverse healthcare contexts. Barriers identified in the literature include workforce limitations, funding constraints, inadequate referral processes, limited specialist knowledge about non-malignant conditions and difficulties integrating palliative approaches within existing care models.15,16 These implementation challenges are further complicated by the heterogeneity of CBPC models, which range from specialist palliative care teams to primary care-led approaches with specialist support.9,11,17
Significantly, the majority of implementation research to date has focused predominantly on organizational, clinical and system-level factors influencing CBPC delivery.18–21 While these perspectives are valuable, they represent only part of the implementation equation. There remains a notable gap in understanding how patients and their caregivers—the intended recipients of these services—perceive and experience the implementation of CBPC, particularly in the context of non-malignant conditions with unpredictable disease trajectories.22,23
This research imbalance is particularly problematic given that implementation science frameworks consistently emphasize the critical importance of stakeholder perspectives in determining intervention success or failure.24,25 The perspectives of patients and caregivers are not merely supplementary but fundamental to understanding the complex social processes that influence how healthcare innovations are adopted, adapted or rejected within communities. 26
The need for patient and caregiver perspectives of living with advanced NCDs
The experiences and perspectives of individuals living with advanced CHF, COPD and ESRF—and those who care for them—are particularly important to understanding CBPC implementation for several compelling reasons. First, these conditions follow distinctly different illness trajectories than cancer, often characterized by unpredictable exacerbations, prolonged decline and uncertain prognosis.27–29 This unpredictability creates unique challenges for palliative care provision that may not be adequately addressed by models developed primarily for cancer populations.28,30
Second, patients with these conditions often experience significant symptom burdens comparable to advanced cancer, including dyspnea, fatigue, pain, anxiety and depression, yet historically have had limited access to specialized palliative services.31,32 Their caregivers similarly face substantial burdens, often managing complex care regimens with inadequate support over extended periods. 33 Understanding how these stakeholders perceive and engage with palliative care initiatives is crucial for developing services that effectively address their needs.
Third, research suggests that patients with non-malignant conditions and their caregivers may conceptualize palliative care differently than healthcare providers, often associating it exclusively with imminent death rather than as an approach focused on quality of life throughout serious illness.34–37 These perceptual differences can significantly influence receptivity to CBPC services and highlight the importance of incorporating patient and caregiver perspectives into implementation planning.
Despite these compelling rationales, research examining CBPC implementation from the perspectives of patients with non-malignant conditions and their caregivers remains limited. This knowledge gap undermines our ability to develop and implement CBPC services that are truly responsive to the needs, preferences and lived realities of those they are intended to serve.
Theoretical framework
This study is grounded in implementation science frameworks that emphasize the importance of stakeholder perspectives in understanding the complex processes through which healthcare innovations are integrated into practice. Specifically, we draw upon the Consolidated Framework for Implementation Research (CFIR) and the Normalization Process Theory (NPT) to examine the multifaceted factors influencing CBPC implementation.24,26
The CFIR provides a comprehensive taxonomy of constructs that influence implementation success, including intervention characteristics, outer setting (the economic, political and social context), inner setting (the structural and cultural contexts), characteristics of individuals involved and the implementation process itself. Notably, this framework recognizes that the perspectives and needs of service recipients are crucial determinants of implementation outcomes, particularly through the constructs of “patient needs and resources” and “adaptability.” 24
Complementing this approach, NPT offers insights into how new practices become normalized (or fail to normalize) within social contexts. This theory emphasizes that successful implementation requires stakeholders to engage in sense-making work (coherence), relationship-building work (cognitive participation), enacting work (collective action) and appraisal work (reflexive monitoring). 26 By applying these theoretical lenses, we examine not only structural and organizational barriers to CBPC implementation but also the social and relational dimensions that profoundly influence how services are received and integrated into community settings.
Research aims and objectives
The primary aim of this study was to understand the barriers and facilitators of implementing CBPC services from the perspectives of patients with advanced CHF, COPD and ESRF, as well as their primary caregivers. We sought to address the following research questions:
RQ1. How do patients with advanced non-malignant conditions and their caregivers perceive the need for and potential value of CBPC services?
RQ2. What factors influence their willingness to engage with new CBPC initiatives?
RQ3. What approaches to service implementation do patients and caregivers believe would enhance acceptability and effectiveness in their communities?
RQ4. How do previous healthcare experiences shape expectations and receptivity towards new community-based services?
By addressing these questions, our research aimed to fill critical gaps in understanding regarding how CBPC services can be implemented in ways that respond meaningfully to the lived experiences and preferences of those they are intended to serve.
Methods
Study design
This study was designed to use qualitative, open-ended in-depth interviews of patients with advanced CHF, COPD and ESRF, and their primary caregivers, and reflexive thematic analysis of the interview data to understand the barriers and facilitators of implementing CBPC services.
Research setting
This study was conducted in five sub-districts (Segamat, Gemereh, Chaah, Bekok and Jambi) of the district of Segamat, in the state of Johor, Malaysia. Collectively, these five sub-districts have a population of approximately 10,400 households (47,000 persons) living in rural, semi-rural and plantation areas. The population ethnically diverse comprises60% ethnic Malays, 23% Malaysian Chinese, 7% Malaysian Indian, with the remaining 10% from other ethnicities. The unemployment rate in Segamat is 2.7% with 29.1% of the population out of the labour force.
Malaysia’s healthcare system comprised a tax revenue-funded public healthcare system and a private healthcare market. Healthcare in Segamat is mainly provided through primary and secondary healthcare facilities operated by the public healthcare system under the Ministry of Health Malaysia, and to a lesser extent, private for-profit primary care providers and alternative medicine practitioners. Conditions such as CHF, COPD and ESRF are mainly managed in the public healthcare facilities; however, patients requiring more specialized diagnostics or treatments often need to travel to either the state capital of Johor Bahru or to Selangor and Kuala Lumpur. At the time of the study, there were no providers of palliative care services or hospices operating in the Segamat district.
Sample population
The study sample population was identified from the South East Asia Community Observatory (SEACO), which is a demographic and health surveillance site operating in Segamat. SEACO was established to study cultural, social, economic, physical and geographical relationships between individuals, households and the broader community, as well as the occurrence of life events such as births, deaths, morbidity, marriage and migration (in and out). As such, SEACO compiles a database of 40,000 persons living in the aforementioned five sub-districts of Segamat that includes their health status and general medical information. 38
We utilized SEACO’s database of inhabitants to identify individuals who met the following inclusion criteria: (1) aged 18 and above, (2) diagnosed with either CHF, COPD or asthma, or ESRF and (3) had two or more specific indicators and at least one general indicator of poor or declining health using the Supportive and Palliative Care Indicators Tool (SPICT). 39
The exclusion criteria were (1) inability to participate in interviews independently due to cognitive impairments, for example, due to dementia, (2) diagnosed with cancer and (3) was currently receiving palliative or hospice care.
Each eligible individual identified from the database was contacted by staff researchers employed by SEACO by telephone and invited to participate in the study. Consenting individuals were asked to nominate an informal primary caregiver (e.g. a family member, friend or neighbour) whom they regarded as important to their care or who provided the majority of their daily care. Caregivers nominated by the patient participant were asked to independently consent to participate in the study. The individual patient participant and the nominated primary caregiver were interviewed at multiple time points throughout the study period. If the nominated caregiver, however, refused to participate in the study, the patient participant was still enrolled in the study and interviewed. Twenty-five of 98 eligible patients and 9 of 25 nominated primary caregivers agreed to participate in the study.
Data collection
All the participants took part in at least one face-to-face, focused open-ended interview, with other interviews taking place through telephone. Decisions on the mode of interview whether face-to-face or telephone were made prioritizing the comfort, convenience and ease of the patient participant. In-person interview locations were also organized based on the preference of the participant, to facilitate their ease of participation. The length of the interviews was guided by the participants but was on average between 45 and 60 min long. Both patient and caregiver participants were interviewed between two and three times in four-monthly intervals throughout the data collection period. Multiple interviews were conducted over the study duration with each participant to observe for changes and variation in their experiences of living with or caring for a person with CHF, ESRF and COPD, as well as any changes in their perceptions towards CBPC. This longitudinal approach provided us with the opportunity to identify and explore new needs and challenges as they developed and to revisit participant perceptions regarding CBPC.
Each interview was focused on four key topic areas but allowed for participants and the researcher to explore certain subjects in varying length and detail (see Topic Guide in Supplemental Material). While successive interviews with each participant used the same four key topic areas, there were variations in the discussion’s length and depth for each key topic area. A pilot test was conducted with three community members living in the Segamat district to test and refine the interview topics. The topics included (1) the experience of living with advanced illness in the community, (2) the needs experienced by patients and their caregivers with regards to their quality of life and care, (3) the perception of establishing a community-based palliative and supportive care to support patients and caregivers and (4) suggestions for how to provide support to patients and caregivers in the community. With regard to topic (3), participants were provided with examples and descriptions of how CBPC was implemented in the United Kingdom and Australia. These descriptions were provided to help participants imagine and conceptualize CBPC, especially after an initial pilot test of the interviews revealed that some participants may not have had any knowledge or awareness of these services. The descriptions were provided to them after an initial check of their awareness of CBPC services. For participants who had any level of awareness of CBPC, the descriptions were provided as additional service models that they could consider and comment on. For participants who had no awareness of CBPC, the descriptions were used to explore their perceptions of such services and their thoughts on having similar service models implemented in their community. The interviews were audio-recorded and transcribed verbatim. Transcription was done manually by the lead researchers (M.W.L.C. and N.A.).
Interviews were conducted by N.A. and M.W.L.C. who are experienced healthcare researchers and have conducted prior studies using qualitative methods. The qualitative data collection was also designed and refined by N.W. who is an academic researcher and expert in qualitative research methods including ethnography and anthropology.
Consistent with reflexive thematic analysis approaches, we did not employ traditional saturation criteria, as our critical realist epistemology recognizes that themes are constructed through interpretation rather than discovered as pre-existing entities. The decision to conclude data collection was made through team discussion considering the richness of data gathered, adequate representation of diverse participant perspectives and pragmatic research timeline constraints.
Analysis
A reflexive thematic analysis approach was employed in this study. 40 A critical realist paradigm was adopted which assumes the existence of an independent reality alongside individual interpretations of that reality which are influenced by their respective experiences, language, culture, social backgrounds and context.
All de-identified transcripts of the interviews were coded by the lead authors (M.W.L.C. and N.A.—N.A. is a health researcher and M.W.L.C. is a senior palliative care researcher, both with training and experience in qualitative research). The coding of the interview transcripts was conducted using the NVivo 12 Pro software (Lumivero). Throughout the coding process, implied views and meanings were taken into consideration and analytical memos were made to complement the data analysis process. The codes as well as the raw data were deliberated between the researchers. Constant comparative techniques were employed throughout the entire coding process for the development of categories and themes that described the participant’s lived experiences, perspectives, attitudes and needs from living with advanced NCDs as well as the provision of caregiving.
The analytical process used was based on Braun and Clarke’s six steps of systematic thematic analysis, beginning with familiarization, and subsequently, keyword selection, coding, theme development, conceptualization and model development. 41 Throughout the analytical process, the CFIR and NPT were used as sensitizing frameworks, even though the thematic analysis approach was primarily inductive. These frameworks provided theoretical lenses during coding that helped us recognize the broader implementation significance of emerging patterns, though they did not predetermine our coding categories. Once themes were established inductively through the iterative coding process, CFIR and NPT were used to interpret and contextualize the findings within implementation science literature, examining how participants’ perspectives related to key constructs such as “patient needs and resources” and “adaptability” (CFIR), and the social processes of coherence, cognitive participation, collective action and reflexive monitoring (NPT). This approach allowed us to remain grounded in participants’ lived experiences while situating our findings within established implementation science theory.
Several strategies ensured methodological rigor and trustworthiness. We maintained notes documenting analytical decisions, code development and theme refinement. Both lead authors kept diaries throughout data collection and analysis. All transcripts were independently coded by two researchers with regular deliberation sessions to discuss coding decisions and resolve discrepancies. The broader research team provided critical input through review of coded data and preliminary themes. Our longitudinal design, with participants interviewed up to three times, allowed us to explore emerging themes in subsequent interviews and verify interpretations over time.
Results
Participant demographics
Twenty-five patients and nine caregivers were recruited and participated in this study. The demographics of the patient and caregiver participants are described in Table 1.
Demographics of study participants.
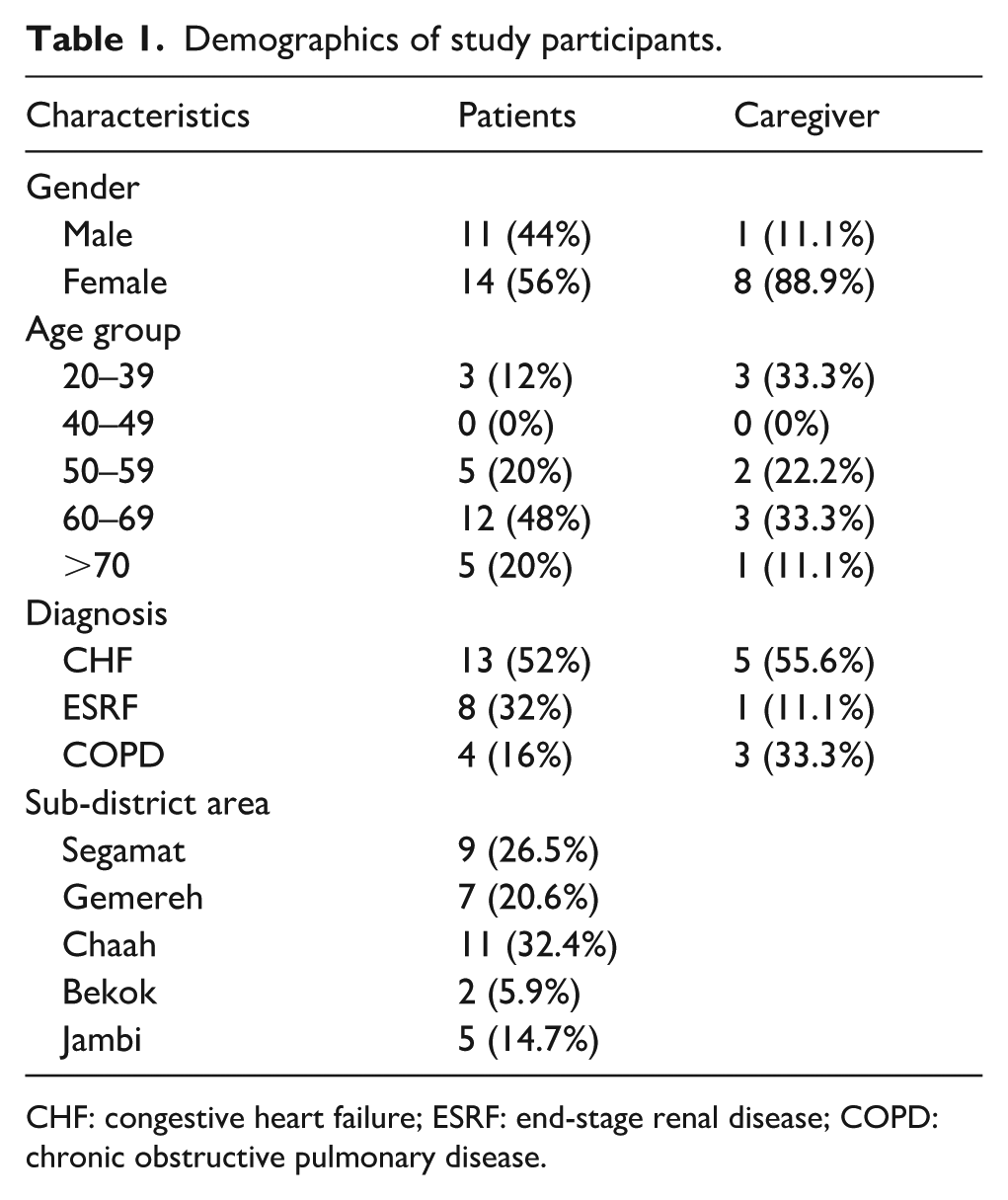
CHF: congestive heart failure; ESRF: end-stage renal disease; COPD: chronic obstructive pulmonary disease.
Key themes
The coding and analysis led to the development of four major themes that collectively address our research questions (R1 to R4). Theme 1 (“What they offer is not what we need”) and Theme 2 (“Supportive relationships over support services”) primarily address RQ1, RQ2 and RQ4, revealing how past healthcare experiences shaped participants’ skepticism towards new services and their preference for relationship-based care. Theme 2 also addresses RQ3 by articulating participants’ suggestions for trust-building and community engagement approaches. Theme 3 (“The myriad cares of family”) further elaborates on RQ1 and RQ3 by illuminating why family-based care was valued and what this implies for service design. Theme 4 (“How to care for us”) addresses RQ1 by identifying unmet needs that community-based services might address. Table 2 summarizes the key barriers and facilitators identified within each theme and their relationship to our research questions.
Summary of key themes, barriers and facilitators to CBPC implementation, and research question alignment.
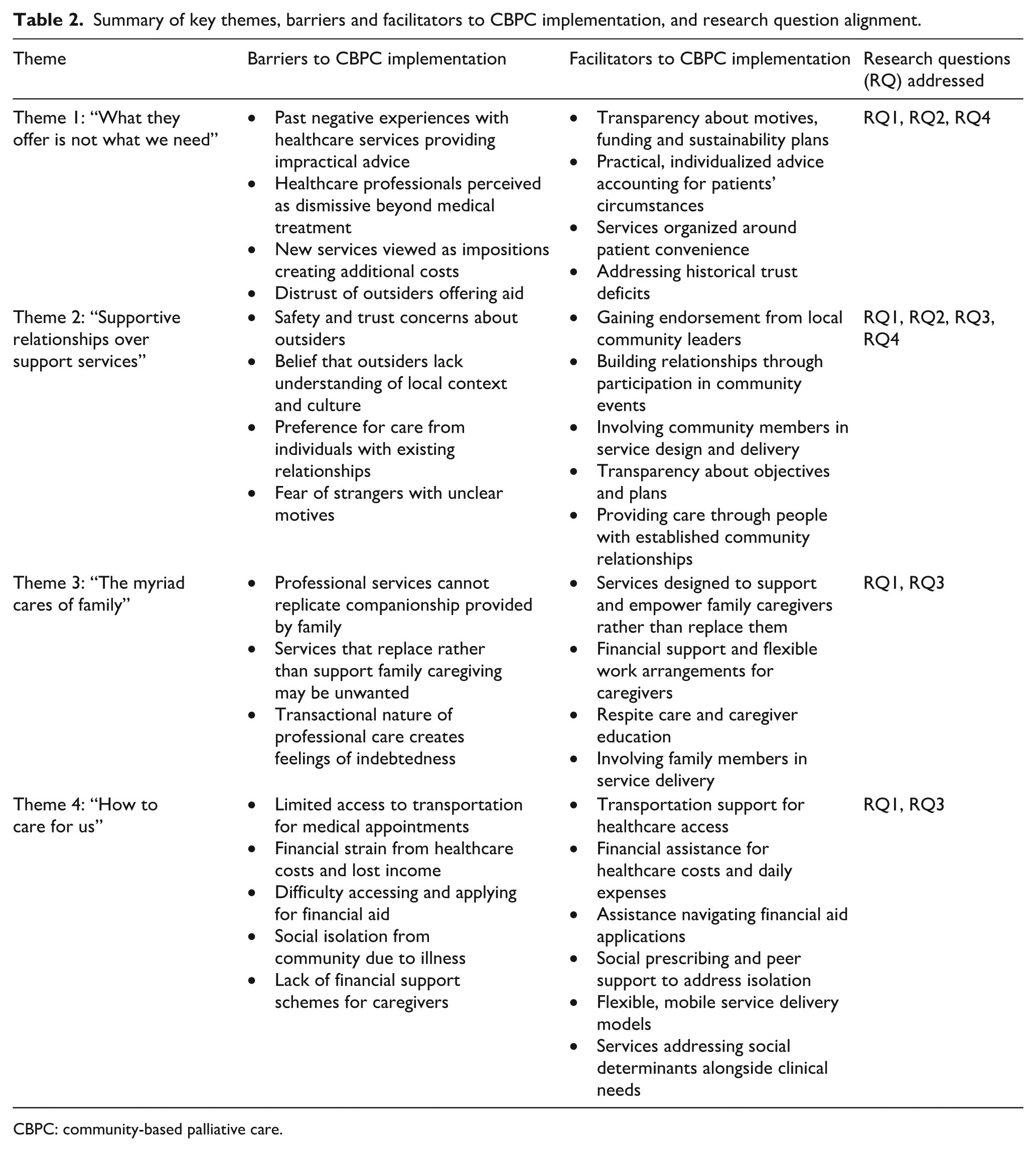
CBPC: community-based palliative care.
Theme 1: “What they offer is not what we need.”
When asked about establishing CBPC services, many participants expressed scepticism or indifference, both before and after receiving descriptions of how such services operate in the United Kingdom and Australia. While there was enthusiasm among some patient and caregiver participants over the benefits of palliative care, there was doubt about how these services could be provided locally in their community: If they come once in a while just to see how we are, that might be okay. But I don’t think it’s possible to provide regular care and keep us company like what we need, right? [HD04, patient] Why do we need this? The hospital already has doctors, nurses. Anything I need, I can get it there. They do it all there. [KP02, patient]
This scepticism stemmed largely from the negative past experiences that they had had with healthcare services. Patient participants described a common experience where, other than providing medical treatment and laboratory tests, health professionals were rarely able to help them with the actual real-life challenges and needs that they faced in trying to live with their illnesses. Many found the healthcare advice given to be generic, impractical or unhelpful, with some participants also finding healthcare professionals to be patronizing and dismissive of their concerns about daily care challenges: The doctor sees me once a month and they just tell me to eat this [medication], don’t eat this [food] but all they do is talk. It’s not as if they’re going to give me the money to buy the medication or the food that is healthy. . . When I asked for help, all they said is “I cannot help you, I can only treat you.” [KP08, patient]
There was also an unwillingness among some patient participants who viewed additional healthcare services as an imposition on them that they were obliged to accept. Some patient and caregiver participants were troubled by the additional costs that would be incurred if they were obliged to receive additional healthcare services. These costs potentially included the additional costs of time, the effort of organizing travel or the preparation for a home visit by a health professional, as well as any additional costs that might be incurred in order to comply with the instructions of a health professional. Healthcare services were seen as inconvenient, often organized around the provider rather than the patient: Of course, there will be costs, impossible for there not to be. Even if I have to travel nearby for [palliative care], I have to pay for transport, for food, for drinks. Everything hits the wallet. [KP02, patient] Since the [doctor] recommended me to take these supplements. . . I have to pay for them myself at the pharmacy outside. [HD04, patient]
These negative experiences made both patient and caregiver participants hesitant to engage with health professionals beyond necessity. They were also sceptical about how palliative care could support them in areas outside of medical treatment.
Participants also distrusted outsiders claiming to offer aid, perceiving them as providing what was convenient rather than to make the effort to understand what the community needed—which resulted in them repeatedly being offered goods or services that they did not want or need: I don’t want to feel like I’m part of those charity reality shows. I’m uncomfortable being made to feel poor and helpless. . . I value my privacy and my struggles are not meant for show or to make others feel good about themselves. [CP01, patient]
Theme 2: “Supportive relationships over support services.”
Despite their scepticism towards having formal palliative care services established in the community to support their needs, participants were open to receiving support if these were provided to them by people who they knew and trusted in the community.
The preference for being supported by trusted community members, close friends and family was based on the belief that these people better understood their daily lives and the cultural, financial and religious challenges without the need for too much burdensome or embarrassing explanation. The participants felt that this understanding would allow for the “helpers” to provide forms of help that would better meet their needs and preferences: If it is other people, I will feel shy. They will want to know everything, whether we are doing things correctly or not, and it feels like someone is judging. Especially as a patient, especially as a sick person there are a lot of secret things. Makes it awkward. It’s not easy. [KP06, patient]
Safety and trust concerns were frequently mentioned, particularly regarding home visits or with leaving family members in the care of strangers. Both patient and caregiver participants felt safer with known individuals or those endorsed by local community leaders or members. The doubts about the unclear motives of volunteers or strangers mentioned in Theme 1 were also part of these fears: Yeah, because we don’t know what they—I mean, the outsiders, what they’re all about. . . and that makes me uncomfortable. I mean, obviously because we don’t know them. And if the outsiders come to the house, we don’t know them, we’re afraid it might disturb the rest of the family, so no, I don’t have problems for them to help me with. [HD12, patient]
Crucially, patient participants valued companionship from people who knew them personally, such as family members, which helped combat loneliness and isolation—something they believed outsiders could not provide. Care by family members was exemplified as ideal care and was offered by the participants as a contrast to the negative experiences they had with healthcare professionals. Family members provided multiple forms of support including household help, transportation, financial assistance, and most importantly, companionship. To many of the participants, these were the kind of support that they needed but were unlikely to get from healthcare workers: With them, I have support, supportive messages. They support my emotions and give me spiritual support—having family members’ company [supports my mental strength] and that is important now in my life. [CP05, patient]
The concerns over safety, the distrust towards outsiders and strangers, as well as the desire for understanding and familiarity expressed by both participants provides some insight into how palliative care providers gain community acceptance and trust. The participants suggested that healthcare providers work on gaining community leader endorsements, participation in community events and transparency about motives, funding and plans for sustainability: It’s easier if I know that someone else in the community has gotten good service from them, or if [the local religious leader] says that he has spoken to them and they are here to help. [CC05, caregiver] They can show their sincerity first, if they can do some things for the community, or join us in our event first. We can get to know them and see if they really want to help us here or not. [KP08, patient]
Theme 3: The myriad cares of family
The care provided by family members was often used by patient participants to illustrate the care they would ideally receive throughout their illness. While some of these descriptions of family care were idealized descriptions by patient participants who were not being cared for by family members currently, these descriptions provide insight into the special role of family in caregiving as seen by the participants as well as the elements of care desired by them.
Family care was valued by many patient participants because of the element of companionship, which they felt could not be provided so easily with outsider or professional caregivers. Many patient participants valued the companionship provided by their family members highly as it helped them reduce their feelings of loneliness and isolation. Some patient participants also described the provision of companionship as the main form of care and support provided by their family caregiver.
Family care was also perceived as non-transactional, unlike paid or professional services. As such, patient participants were more comfortable in asking family caregivers for help with private and personal matters such as toileting and hygiene, which they felt was unreasonable to ask of professional helpers: Actually, I would feel very shy [receiving help from outsiders]. If it’s from family, I won’t feel so shy. I would be less embarrassed [to ask for help]. You understand, right? [KP07, patient]
Being cared for by, and in the company of, family caregivers also helped the patient participants maintain their roles and identities within family structures—as parents, spouses, siblings or children. This was crucial for those struggling with loss of professional identity and increasing community isolation. It also allowed them to continue providing care for other family members as well. Many patient participants were, in fact, caregivers to other family members who were similarly ill—a reminder that patients and caregivers often inhabit both roles simultaneously: Ha, since I don’t usually go anywhere outside now, I can still do things like cook for family, I can take care of [my grandchild], I still have things to do for them. I still need to take care of my husband. . . I follow him to his appointment, and he follows me to my appointments. . . . [HD01, patient]
Many caregiver participants also described the positive elements of being able to provide care to their ill family members while fully acknowledging the burdens they faced as caregivers. They viewed care provision as a privilege and opportunity to express love, build closer relationships and find meaning and purpose: I do what I can to take care of her, like with the housework and all. . . because we live under the same roof, I see her being sick which makes me sad, but then again it also lets me be closer to her. So I feel grateful for being here. [HC12, caregiver]
Given this perspective, most caregiver participants preferred services that would alleviate other life burdens—financial challenges and inflexible work schedules—rather than replacing their caregiving duties, allowing them to focus more on providing care to their loved ones: No need for all that, I can take care of [the patient] myself, we can do it ourselves. I already gave up on a work promotion and I shifted back to stay with [the patient] so I can care for them. Now I need. . . part-time jobs where I have more time to take care and stay at home—or if got some financial support, better. [KC08, caregiver]
Theme 4: How to care for us
Both patients and caregivers faced significant challenges impacting their quality of life, health and daily living, revealing unmet needs that community-based services might address.
One such unmet need was transportation and mobility support. Living with a chronic illness often required frequent travel for treatment, specialist visits and laboratory tests, often over long distances and at high cost. Patient participants struggling to drive due to illness-related fatigue and impairments faced significant challenges, sometimes forgoing medical appointments when transportation was unavailable: Can [drive] a bit, a bit. No choice. . . who is going to send me. . . everyone is busy, so good luck to those who can’t drive. There is no car or van to take us to the dialysis centre, so I have to drive. But the other day, when it flooded, I dare not drive—my eyesight is blurry—so I couldn’t go for a week. When I called them, they told me to wait for the flood to end. [KP08, patient]
Financial assistance was another reported unmet need. Many participants struggled with increased healthcare costs, medication expenses and medical supplies. Some of them admitted forgoing treatment due to financial constraints, worsening their health. The participants also described needing both direct financial support as well as help navigating the application process for financial aid as many of their applications had previously failed due to overly complex instructions. Financial difficulties, unsurprisingly, affected the participants’ quality of life as they had to frequently make difficult decisions regarding medical expenses, daily necessities, as well as the financial needs of other family members: Yeah, for sure, sometimes we don’t have enough for everything like daily expenses and other things. We have no choice—like it or not, you have to pay for water, power, food. If you don’t, or if you stop, then your life just get’s much harder. So, if we know it’s coming to that time of the month [to pay the bills], we will just stop spending on other things. If it’s an emergency, sometimes, I’ll ask [community members] for help. But that’s how it is. . . . [HD01, patient]
Limited income sources due to job loss among both patient and caregiver participants further compounded their financial difficulties. Most patient participants were unemployed due to age or illness, while many caregiver participants struggled to find flexible employment that could accommodate their caregiving duties. Financial support schemes for caregivers were particularly scarce: Maybe if the government could help support caregivers, that would be great. Caregivers like us spend a lot of our time, but we’re not given any payment. So, if there were some financial support from the government, God bless them, it would be good. I would love it, I would accept it. [HC01, caregiver]
The patient participants also commonly described how their illness and the disabilities resulting from it left them isolated from their friends, neighbours and the wider community, giving rise to an unmet need for social connection and companionship. They described being excluded from social activities and community events (at times, of their own choosing), leading to loneliness and the gradual decline of their mental health. This was particularly significant for patient participants who lacked regular companionship from family and friends: I am just afraid. . . if anything were to happen, who will realize, who will know to look for me, people don’t know I am alone here. [HD04, patient]
Discussion
This study reveals insights into the complex dynamics underlying community acceptance of palliative care services, challenging fundamental assumptions about healthcare service implementation in community settings. Our findings demonstrate that the patients with advanced NCDs and their caregivers exhibit significant scepticism towards new healthcare services, not because they lack the need for support, but because their lived experiences have shaped distinct preferences for how care should be delivered and by whom.
Challenging the “build it and they will come” paradigm
Our study challenges the prevailing assumption that establishing clinically sound, evidence-based services will naturally lead to community uptake. The scepticism and indifference expressed by participants towards a proposed CBPC service—despite their clear unmet needs—reveals the limitations of supply-side approaches to healthcare implementation, aligning with implementation science literature demonstrating that the mere service availability does not guarantee adoption.25,42
The participants’ resistance was not rooted in a rejection of support per se, but rather in their accumulated experiences with healthcare systems that had repeatedly failed to address their lived realities. Their scepticism represents a rational response to previous encounters with services that were designed without meaningful community input and delivered in ways that prioritized provider convenience over patient needs. This finding resonates with NPT’s emphasis on how individuals engage in sense-making work when encountering new interventions. 26 For our participants, their sense-making process was profoundly influenced by past disappointments, creating cognitive barriers to accepting new services. Efforts to deliver new healthcare services must therefore address historical experiences and trust deficits, not simply present evidence about intervention effectiveness, while providing opportunities for positive experiences that can reshape future coherence work.
The preference for “supportive relationships over supportive services” represents more than simple preference—it reflects a fundamentally different conceptualization of what constitutes effective care. While healthcare systems organize around service delivery models, our participants’ prioritized relational continuity, trust and understanding, suggesting that successful implementation requires moving beyond transactional service provision towards relationship-centred care models.
The centrality of trust and relationship-building
Perhaps our most significant finding is the participants’ emphasis on trust-building as a prerequisite for service acceptance. This finding extends beyond typical discussions of patient–provider relationships to encompass community-level trust and the social processes through which healthcare providers establish legitimacy within local contexts. Participants clearly articulated that healthcare providers must “earn the trust of their communities”—a process requiring sustained engagement rather than professional credentials alone—before attempting to offer services.
This emphasis on community-level trust reflects what anthropological literature has long recognized: that healthcare interventions are fundamentally social processes that must navigate existing social structures, relationships and power dynamics.43,44 Our participants’ preference for care from people they had relationships with suggests that effective palliative care implementation must account for the social embeddedness of care relationships. This finding challenges healthcare systems that prioritize professional expertise over relational continuity and suggests that community health worker models or peer support approaches may be more acceptable than specialist-led services.
The participants’ suggestions for trust-building—including gaining endorsement from community leaders, participating in community events and demonstrating transparency about motives and funding—provide concrete guidance for implementation approaches. These strategies reflect principles of community organizing and participatory development that emphasize the importance of establishing social capital before attempting to introduce innovations. 45 The fact that participants spontaneously identified these approaches suggests an intuitive understanding of what constitutes legitimate community engagement.
Importantly, the trust-building process our participants described is fundamentally different from typical healthcare provider–patient relationship development. It requires healthcare providers to engage with communities as communities, not simply as collections of individual patients. This community-level engagement demands skills and approaches that may not be emphasized in traditional healthcare professional training, suggesting the need for new competencies in community engagement and relationship-building.
The primacy of social and relational dimensions of care
Our study reveals that participants’ care preferences were fundamentally social and relational rather than primarily medical. Social isolation was also identified as a significant concern. The participants conceptualized ideal care as encompassing companionship, maintenance of identity and roles and non-transactional support. This finding challenges healthcare systems that organize primarily around clinical interventions and suggests that effective CBPC must address the social dimensions of illness, including loneliness and isolation, through social prescribing, peer support and community engagement strategies.
The participants’ preference for family caregivers was not simply about familiarity or convenience—it reflected deep-seated values about reciprocity, dignity and the maintenance of social relationships in the face of serious illness. Family caregivers were valued because they could provide companionship, maintain the patient’s roles and identity within family structures and offer support without creating feelings of indebtedness. These preferences align with research on the social determinants of health, which recognizes that health outcomes are profoundly influenced by social relationships and community connections. 46
Importantly, our findings suggest that family caregivers did not want to be replaced by professional services but rather supported in their caregiving roles. This finding has significant implications for palliative care service design, suggesting that effective community-based approaches should focus on caregiver support and empowerment rather than caregiver replacement. Such approaches might include caregiver education and training, respite care, financial support and assistance with non-caregiving burdens that interfere with caregiving capacity.
It is important to note that our findings regarding family caregiving reflect a specific context where multigenerational households and extended family networks facilitate family-based care. In societies where family structures differ—such as contexts with predominantly nuclear families, geographically dispersed relatives, or competing employment demands—the specific caregiving arrangements described by our participants may not be feasible. However, the underlying principles participants articulated—preferences for relational rather than transactional care, care provided by trusted individuals and support that maintains patient identity and dignity—may have broader applicability across diverse caregiving contexts. Moreover, the barriers to family caregiving identified by participants (inflexible work, financial constraints, transportation challenges) may be even more pronounced in contexts where family members face geographic distance and employment demands, suggesting that addressing these structural barriers through community-based support services may be particularly important. Critically, this observation reinforces our argument that effective CBPC must be co-developed with communities to ensure services align with local family structures, caregiving arrangements and social realities rather than assuming a universal caregiving model.
Addressing structural determinants of health and illness
Our study identified significant unmet needs related to transportation, financial support and access to social services—needs that extend beyond traditional healthcare service boundaries but profoundly impact health outcomes and quality of life. These findings align with growing recognition that health is socially determined and that effective healthcare interventions must address the structural conditions that shape health experiences. 47
The transportation challenges identified by participants illustrate how healthcare systems’ organization around fixed locations and scheduled appointments can create barriers for individuals with mobility limitations and limited resources, supporting the argument for mobile or remote service delivery models and community-based transportation support. Additionally, the financial burdens described by participants—including medication costs, healthcare expenses and lost income—reflect broader issues of healthcare affordability and social protection. Participants’ reports of forgoing medications and treatments due to cost illustrate how financial barriers can undermine clinical care effectiveness. Finally, the social isolation described by the participants reflects broader issues of community integration and social support that healthcare systems typically do not address but may be as important as addressing clinical symptoms for maintaining quality of life in serious illness.
These findings about transportation, financial and social barriers underscore a broader issue: the failure of healthcare systems to operationalize genuinely person-centred care. The participants’ frustrations with receiving generic, impractical advice that ignored their financial constraints, transportation challenges and social circumstances reflect what occurs when person-centred care remains an aspirational principle rather than a practice reality. Person-centred care—defined as care that is respectful of and responsive to individual patient preferences, needs and values—requires healthcare providers to understand and address the social, economic and cultural contexts shaping patients’ lives, not simply their clinical presentations. The participants’ negative experiences suggest that healthcare providers often delivered standardized advice without taking time to understand each individual’s unique circumstances, resources and constraints.
Our findings suggest that achieving person-centred care in CBPC requires more than individualized clinical consultations; it demands sustained relationships that allow providers to develop deep understanding of individuals’ circumstances, co-develop care plans that are realistic and achievable within their constraints and actively work to address the structural barriers—financial, social and logistical—that shape health experiences. The emphasis participants placed on relationships, trust-building and co-development can thus be understood as articulating the essential preconditions for genuine person-centred care, suggesting that current approaches in palliative services may need fundamental reconceptualization to move from rhetoric to reality.
Strengths and limitations
This study has several important strengths. The focus on patient and caregiver perspectives addresses a significant gap in implementation research, which has predominantly examined organizational and provider factors. Our longitudinal approach with multiple interviews per participant provided rich, in-depth insights into lived experiences and preferences, while also allowing us to verify interpretations over time. The inclusion of both patients and caregivers offered comprehensive understanding of care dynamics, while the focus on non-malignant conditions addresses an underserved population in palliative care research. The use of established implementation science frameworks (CFIR and NPT) as sensitizing frameworks helped situate our findings within broader theoretical contexts while maintaining an inductive approach grounded in participants’ experiences.
However, several methodological limitations should be acknowledged. First, the relatively low participation rate (25 of 98 eligible patients; 9 of 25 nominated caregivers) raises questions about potential selection bias, as those who agreed to participate may have had different perspectives or experiences than those who declined. We did not systematically collect data on reasons for non-participation, which limits our understanding of whether certain perspectives are underrepresented in our findings. Second, while we maintained reflexivity logs throughout the research process, we did not return transcripts to participants for verification or conduct formal member checking sessions beyond the iterative exploration of themes in subsequent interviews. This may have limited opportunities for participants to correct misinterpretations or elaborate on their perspectives. Third, the focus on a single geographical region with specific demographic, cultural and healthcare system characteristics may limit transferability to other contexts, though identified themes align with broader literature on community engagement and healthcare implementation.43,44 Fourth, our study examined perceptions of hypothetical services rather than experiences with actual implementations. Participants’ views about proposed services may differ from their actual experiences once such services are established, which may limit the practical applicability of findings. Fifth, the emphasis on participants’ perspectives, while valuable for addressing our research questions, should be complemented by research examining healthcare provider, system administrator and policymaker perspectives on community engagement approaches to provide a more complete understanding of implementation dynamics. Finally, while our sample achieved diversity across conditions, age groups and geographic sub-districts, the predominantly female caregiver sample (89%) reflects gendered caregiving patterns but may underrepresent male caregiver perspectives.
Conclusion
This study provides critical insights into the complex social processes underlying community acceptance of palliative care services. Our findings demonstrate that successful implementation requires moving beyond traditional service delivery models towards relationship-centred, community-engaged approaches that prioritize trust-building, co-development and genuine partnership. The scepticism expressed by participants towards new healthcare services reflects rational responses to historical experiences and should inform implementation strategies that address trust deficits and power imbalances.
Most importantly, our findings suggest that effective CBPC must be truly community-based—not simply located in communities but designed, developed and delivered in partnership with communities. This approach requires fundamental shifts in how healthcare systems conceptualize service development and delivery, moving from expert-driven models towards participatory approaches that recognize communities as partners rather than simply recipients of care. Such approaches may be more complex and resource-intensive than traditional service delivery models, but our findings suggest they may be essential for achieving the goals of accessible, acceptable and effective palliative care for all who need it.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251409212 – Supplemental material for “Supportive relationships over support services”—A qualitative study of patient and caregiver perspectives on the implementation of community-based palliative care for people living with advanced noncommunicable diseases
Supplemental material, sj-docx-1-pcr-10.1177_26323524251409212 for “Supportive relationships over support services”—A qualitative study of patient and caregiver perspectives on the implementation of community-based palliative care for people living with advanced noncommunicable diseases by Mark Wing Loong Cheong, Nurul Aqilah, Shaun Wen Huey Lee, Sylvia McCarthy, Daniel D. Reidpath, Narelle Warren and Tin Tin Su in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank Dr Devi Mohan, the staff of the South East Asia Community Observatory, as well as the Segamat community members for their support of this study.
Ethical considerations
This study received ethical approval from the Monash University Human Research Ethics Committee (Project ID: 27097) on 22 April 2021. This research was conducted ethically in accordance with the Declaration of Helsinki.
Consent to participate
All participants provided written informed consent prior to enrolment in the study.
Consent for publication
All participants provided written informed consent for publication.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Fundamental Research Grant Scheme (FRGS), Ministry of Higher Education, Malaysia (Project code: FRGS/1/2020/SKK04/MUSM/03/1).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analysed during the current study are not publicly available due to the inclusion of personal information or details that may potentially identify individual participants, but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.