
Abstract
Background:
To achieve universal care and overcome existing barriers, the most effective strategy is to devise an action plan that incorporates palliative care into primary health care (PHC), as recommended by the World Health Organization’s (WHO) Astana Declaration. In Colombia, a country with an upper-middle-income status, about 128,000 individuals experience severe health-related suffering (SHS) that necessitates palliative care. Although the country’s healthcare system has made steady strides in the integration and development of palliative care, there is still no national plan in place for palliative care.
Objective:
Build up Colombia’s palliative care plan through stakeholder consensus.
Method:
Based on the participatory action research method and the multi-stakeholder platforms model, this study convened 142 stakeholders from different levels of the health system (patient representatives, journalists, health professionals, government entities, insurance companies, universities, and drug regulatory authorities)
Results:
The national plan aims to achieve its objectives through a series of strategic actions. These include integrating and diversifying palliative care services, improving access to opioids, increasing palliative care education, promoting community-based palliative care programs, securing funding, and implementing a regulatory framework for palliative care by public policymakers.
Conclusions:
The national palliative care is an alliance that aims to reduce palliative care inequity in Colombia by 2026 by empowering stakeholders nationwide to collaborate around specific goals and objectives.
Keywords
Highlights
The Astana Declaration suggests creating a plan for integrating palliative care into primary health care.
The Colombian plan for palliative care is suited to provide universal health coverage.
Through participatory research, stakeholders’ interests build the national palliative care plan.
The Colombian plan for palliative care can counterbalance development disparities.
The national plan for palliative care is suited to the challenges of each region.
Introduction
Public health systems are going through a historic and decisive moment. As of the end of 2019, 61 million adults and children in the world died experiencing preventable and treatable suffering. 1 Future projections predict a percentage increase of up to 87% of global suffering, 2 and the COVID-19 pandemic is adding day by day an unknown number of people who die experiencing suffering amenable to palliative care interventions.3,4 In addition, people who live experiencing suffering related to chronic noncommunicable diseases (NCDs) should also be considered because their economic burden results in impoverished countries, especially middle- and low-income countries, 5 increasing global inequity and preventing them from achieving most of the sustainable development goals (SDGs). 6 In 2018, the three leading scientific organizations of palliative care stated that the current situation is an exponentially growing crisis of suffering. 4 International efforts and advances led from a perspective of specialized care delivery have been insufficient and isolated. 7 The main solutions proposed by different think tanks include incorporating palliative care into primary health care (PHC) 8 – 10 and involving health system stakeholders in the processes of identifying barriers to care and decision-making to achieve a greater impact. 11 – 13 These proposals were taken up by the World Health Organization (WHO) in the 2018 Astana Declaration where countries are invited to empower communities and establish PHC as the backbone of their health systems, recognizing palliative care as a primary factor of the initiative. 14 The WHO package of essential noncommunicable (PEN) disease interventions for PHC in low-resource countries, which is a practical approach to the adopted resolutions, included an entire chapter on palliative care. 15
Each country must now draw up an action plan to integrate palliative care into its health system. Some scientific organizations and countries have already undertaken initiatives to start this process. 16 – 20 The multi-stakeholder platforms (MSPs) model has been proposed in international guidelines, and it seeks to empower stakeholders working in a multisectoral manner at different levels of the system. 14 This model makes it possible to address the complex challenge presented by a sustainable transition of the health system in the long term through collaborative and diverse strategic planning that considers the multiplicity of visions and actors involved. 21 This project aims to build, based on MSP, the action plan that integrates palliative care into the Colombian health system by 2026.
Methods
The Colombian action plan for palliative care was built in four phases, following the participatory action research method, which empowers and involves the stakeholders in the decision-making process. Colombia is an upper-middle-income Latin American country according to the World Bank classification (2021), 22 and it has generalized palliative care provision (category 3b) according to the latest global measurement. 23 The Institutional Review Board of the authors institute approved the study.
Phase 1. Getting to know the territories
Information reported by the Colombian Palliative Care Observatory [Observatorio Colombiano de Cuidados Paliativos (OCCP)] was used to establish a baseline of development and integration of palliative care in the country. This is an inter-institutional information system that monitors palliative care activity in seven dimensions: context, palliative care services, essential medicines, education, public policies, vitality, and funding. 24 The baseline results were organized by regional nodes (Amazonia, Orinoquia, Northeast, Bogotá, Pacific, Central, and Caribbean nodes), territorial units of study defined in previous studies 25 to understand the country’s needs and resources from a territorial approach.
Using the OCCP dimensions, an online semi-structured interview was designed to explore the development of palliative care and the stakeholders’ perception of needs and resources in the regional nodes. The stakeholders were selected through snowball sampling, and they included patient representatives, health professionals, government entities, health insurance companies, and journalists. The qualitative data were analyzed using a content analysis method, and the findings are reported in a previous publication that maps stakeholders’ viewpoints on barriers for each dimension and regional node under study. 26 The interviews were recorded and transcribed in MS Word. Data saturation for each node was reached when the stakeholders did not provide new information that would contribute to identifying more perception of needs and resources in the regional nodes. Interviews were coded and synthesized using NVivo software.
Phase 2. General framework of actions for palliative care
With the information obtained in phase 1, a technical document entitled ‘General Framework of Actions’ (GFA) was written. A panel of experts, specialists in palliative care, public health, PHC, and family practice, synthesized the information. The GFA was structured around strategic objectives, activities, barriers, strengths, and stakeholders, and it was used as a starting point for the multi-stakeholders’ analysis of the proposed actions.
Phase 3. Multi-stakeholders’ assessment of actions
The multi-stakeholders’ analysis was organized through a national public open call, in which different audiences were invited to participate in seven regional online workshops (one by territorial node). Each regional workshop had four participant profiles: (a) health care providers, including palliative care specialists, PHC professionals, pediatric palliative care providers, nurses, and psychosocial professionals; (b) patient representatives; (c) palliative care educators in undergraduate and graduate programs; and (d) representatives of the opioid regulatory authorities. In the regional workshops, holding an open discussion led by a moderator from the region, the participants provided feedback about the feasibility of the proposed actions and the relevance of the activities for each explored dimension. They also agreed on further actions to improve palliative care in their regions. Each workshop session was video recorded, and two independent rapporteurs wrote up minutes of the sessions. With the information obtained, the actions proposed by the participants were adjusted and included in the GFA.
Phase 4. Colombian palliative care plan for 2026
The GFA adjusted in phase 3 was taken up again in a national workshop that brought together leaders from scientific organizations of palliative care, home-based care, and psychosocial and spiritual support; associations of faculties of medicine, nursing, and psychology; officials from the areas of chronic diseases and health human resources of the Colombian Ministry of Health; and officials representing the national opioid regulatory authority, the National Cancer Institute, and the health insurance companies. The GFA was reviewed and articulated in a document with specific goals and defined time frames to achieve them. This document was then shared online with and commented on by the participants and the institutions identified as key stakeholders during the design of the plan. With the comments received, the final document of the Colombian action plan for the integration of palliative care by 2026 was written.
Results
The study was conducted between September 2019 and July 2021. A total of 142 stakeholders with diverse backgrounds and origins participated throughout the project. Supplementary Table S1 shows the profile and number of participants for each phase and regional node. The results reported below are presented according to the four phases previously described.
Phase 1. Getting to know the territories
Supplementary Table S2 shows the current level of development of palliative care in Colombia. The OCCP data consolidated by dimensions and nodes showed four asymmetric levels of development. An extremely low level of palliative care was observed in the Amazonia and Orinoquia nodes with less than 0.5 services per 100,000 inhabitants, morphine consumption of less than 2 mg per capita, no academic education in palliative care, and a lack of health professionals and research projects. A low level of palliative care was found in the Pacific node and the Northeast node with 0.5 to 1 service per 100,000 inhabitants, morphine consumption of less than 2 mg per capita, low academic education in palliative care, low presence of health professionals, and lack of research projects. An intermediate level of palliative care was observed in the Central and the Caribbean nodes with 1 to 1.5 services per 100,000 inhabitants, morphine consumption of less than 5 mg per capita, little academic education in palliative care, low presence of health professionals, and absence of research projects. A high level of palliative care was identified in the Bogotá node with 1 to 1.5 services per 100,000 inhabitants, morphine consumption of 24.8 mg per capita, availability of academic education in palliative care, and presence of health professionals and research projects. The public policy and financing dimensions in the seven nodes are equivalent due to the country’s centralized system, so it is not possible to make territorial comparisons with these dimensions. These identified development differences contrast with each node’s need for palliative care evidenced in the context dimension. The percentage of SHS in children is similar across the seven nodes, and it is in the range 7–8.7%. On the contrary, the percentage of SHS in adults are in the range 47.4–56%.
Thirty-three palliative care stakeholders participated in the interviews. Twenty-seven barriers to palliative care were identified in the regional nodes in the different dimensions (see Table 1).
Barriers in palliative care dimensions per node.
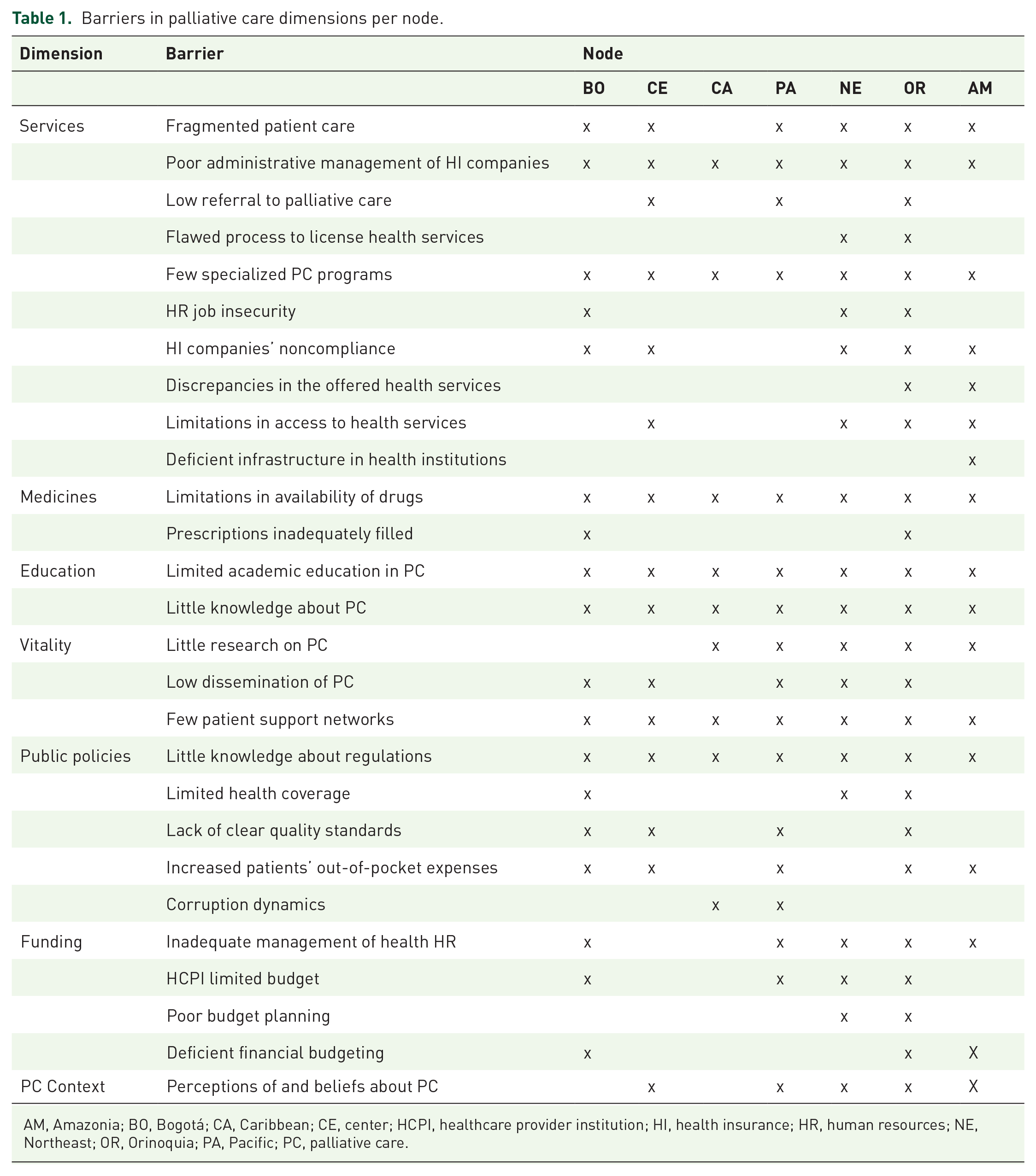
AM, Amazonia; BO, Bogotá; CA, Caribbean; CE, center; HCPI, healthcare provider institution; HI, health insurance; HR, human resources; NE, Northeast; OR, Orinoquia; PA, Pacific; PC, palliative care.
The Caribbean node reported 9 barriers, the Central node reported 15, the Amazonia and Pacific nodes reported 17, the Bogotá node reported 18, the Northeast node reported 19, and the Orinoquia node reported 25. The dimensions with the highest number of barriers were service (10 barriers), followed by public policies (5 barriers), and funding (4 barriers). The dimensions with the lowest number of barriers were medicines (two barriers), education (two barriers), and context (one barrier). The following seven barriers were common to all nodes: Poor administrative management of health insurance companies (service dimension), few specialized palliative care programs (service dimension), limitations in availability of drugs (medicines dimension), limited academic education in palliative care (education dimension), little knowledge about palliative care (education dimension), few support networks for patients (vitality dimension), and little knowledge about regulations (public policies dimension). The other barriers were common in at least two regional nodes. The barrier of deficient infrastructure in health institutions (dimension of services) was only identified in the Amazonia node.
Phase 2. General framework of actions for palliative care
The territorial diagnosis revealed the need to establish common objectives with individualized strategic actions in the GFA, as summarized in Table 2.
General framework with objectives and strategic actions of the palliative care action plan.
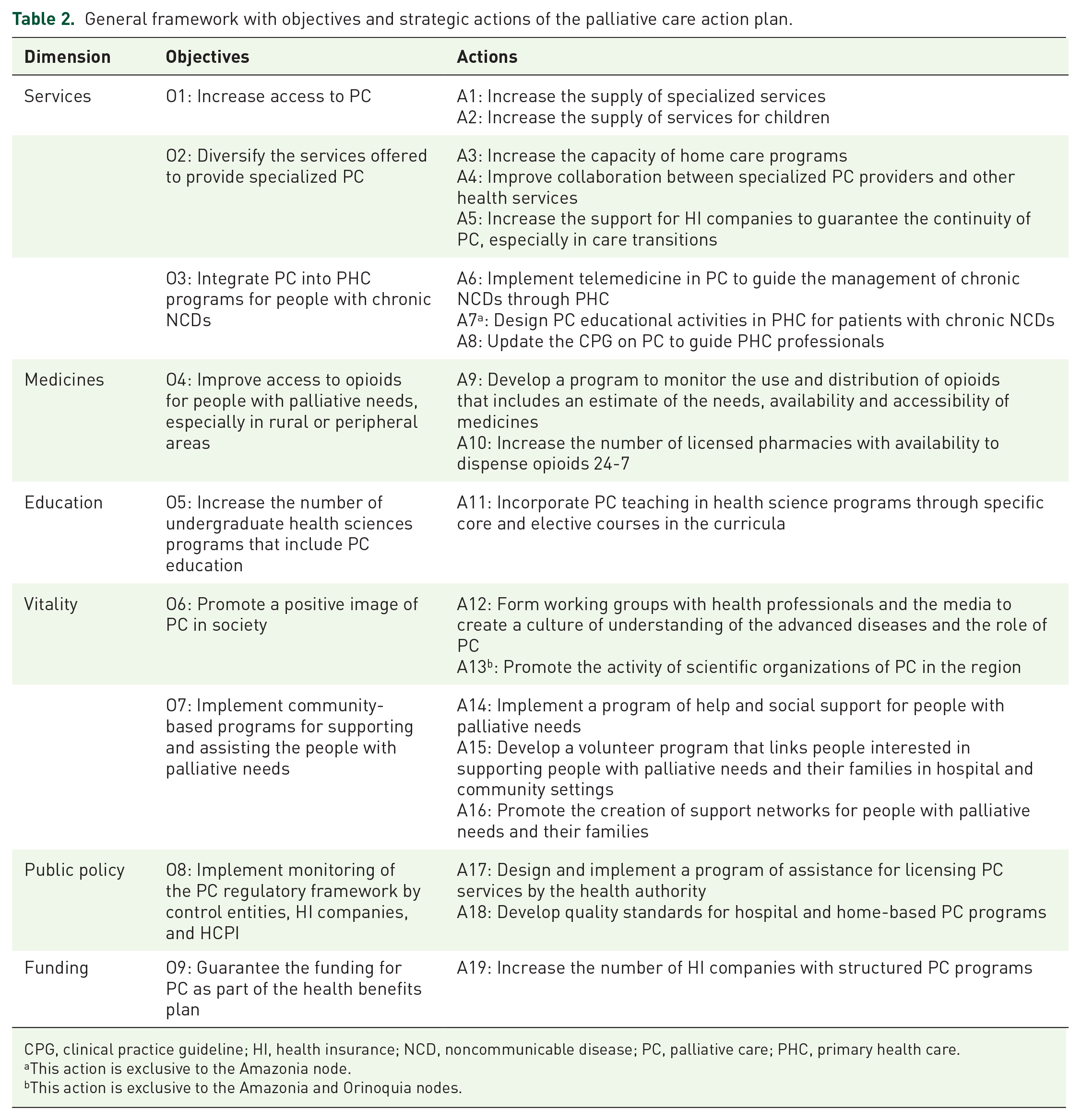
CPG, clinical practice guideline; HI, health insurance; NCD, noncommunicable disease; PC, palliative care; PHC, primary health care.
This action is exclusive to the Amazonia node.
This action is exclusive to the Amazonia and Orinoquia nodes.
The GFA, written by four authors, proposes nine objectives and 19 strategic actions for palliative care development, 2 of these strategic actions are exclusive to the nodes with the lowest levels of development: strategic actions 7 and 13. The GFA aims to increase specialized palliative care services for adults and children; diversify the services offered through collaboration and support from the health insurance companies, other medical services, and home palliative care; and integrate palliative care services into PHC through telemedicine and clinical practice guidelines (CPG) for primary care. In addition, it also seeks to improve access to opioid medications by increasing the number of pharmacies that dispense them and monitoring their use and distribution. The GFA also aims to increase palliative care education in health sciences curricula, establish monitoring of regulation by regulatory entities and ensure universal funding for care. Finally, the GFA aims to implement community-based programs and promote a positive image of palliative care.
Phase 3. Multi-stakeholder’s assessment of actions
Eighty-four stakeholders participated in the regional workshops and proposed 23 additional strategic actions. No additional objectives were proposed for inclusion in the GFA. Table 3 shows all the additions.
Strategic actions proposed in regional workshops.

HI: health insurance; PC: palliative care.
The education dimension received the highest number of additional strategic actions: nine proposals. Most of them include optimizing training for health care personnel and the general population, using technology for distance learning, and involving non-palliative care professionals through different methods. The service dimension has the second-highest number of additional strategic actions: eight proposals. The suggested actions stressed the importance of increasing palliative care services for pediatric and indigenous populations and establishing continuous communication with health insurance companies to design new palliative care services and promote palliative care advantages. The dimension of medicines received four additional strategic actions: three involved drug regulatory authorities to advance accessibility, traceability, and good use of opioids, and one advocated for the availability of opioids in dosage forms and concentrations appropriate for pediatric use. The public policy dimension received the lowest number of new strategic actions: one aimed to make the regulations in force known and the other to influence public policy by having better communication with the entities in charge. The context and funding dimensions did not receive additional strategic actions or modifications.
Phase 4. Colombian palliative care plan for 2026
The modified GFA was taken up for discussion at the national workshop, where 25 stakeholders proposed 17 development goals of palliative care linked to the objectives stated. Table 4 shows the goals by each objective and the established time frame to achieve them.
Goals of the national action plan in palliative care.
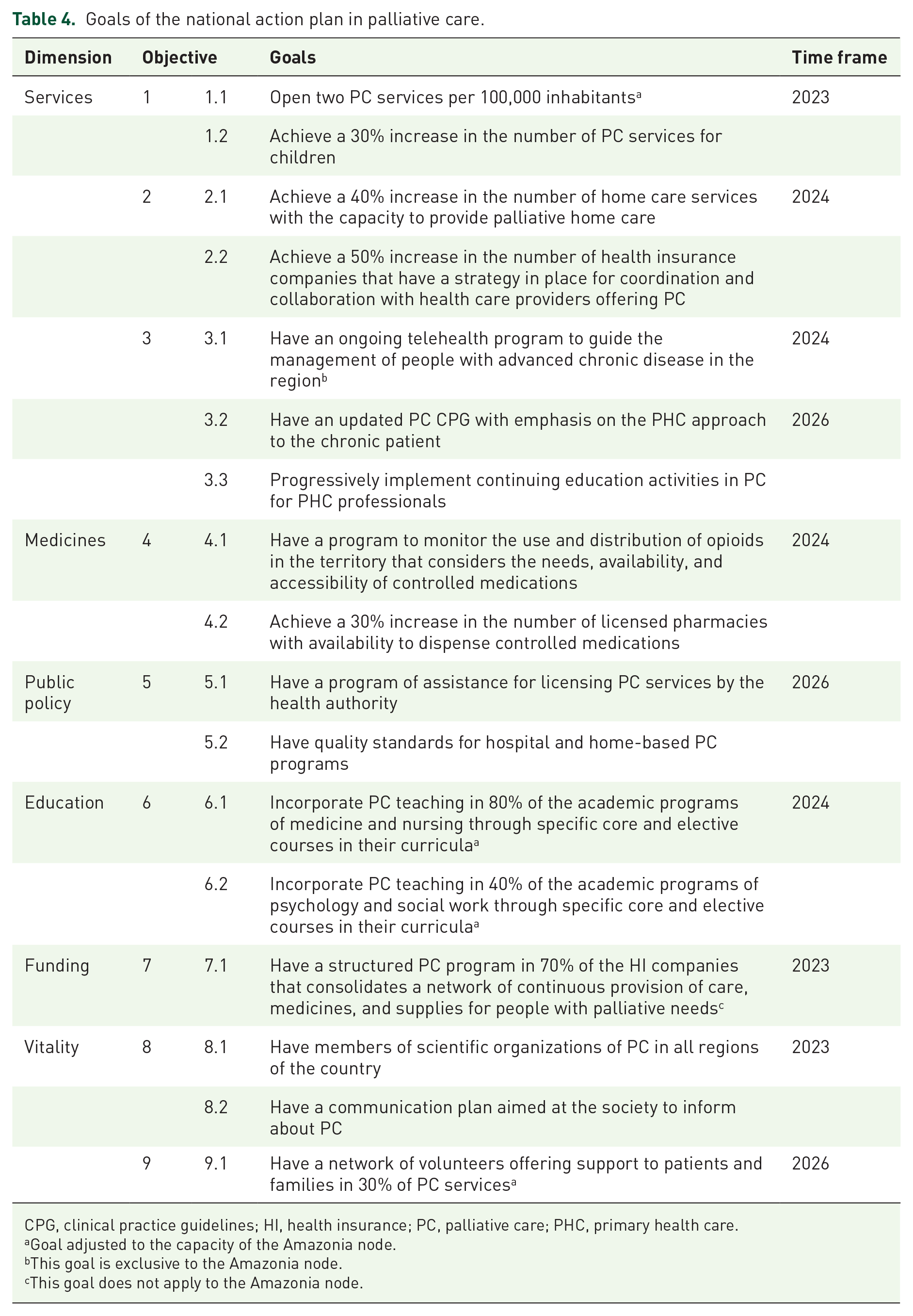
CPG, clinical practice guidelines; HI, health insurance; PC, palliative care; PHC, primary health care.
Goal adjusted to the capacity of the Amazonia node.
This goal is exclusive to the Amazonia node.
This goal does not apply to the Amazonia node.
Five short-term goals were established: to increase the number of services, achieve a 30% increase in the number of palliative care services for children, establish a palliative care network with health insurance companies, have members of scientific organizations in the seven regional nodes, and create a communication plan on palliative care for society (deadline 2023). Seven medium-term goals were established: to increase home care services, have pharmacies with opioid availability, have health insurance companies offering palliative care, have a telehealth program for palliative care, have a monitoring program of opioids, incorporate palliative care into medical and other health science academic programs (deadline 2024). Finally, five long-term goals were established: to have a CPG for palliative care in PHC, design palliative care educational activities for PHC professionals, have assistance from the health authority to license palliative care services with quality standards, and create a network of volunteers offering support to patients and families (deadline 2026).
The goals were commonly and individually set according to the regional possibilities explored in phases 1 and 3. Therefore, goals 1.1, 6.1, 6.2, and 6.3 were adapted for the Amazonia node. Finally, other goals could not be adapted or were specifically created to strengthen regional nodes with low levels of development; this is the case with goals 3.1, 7.1, and 7.2. These goals and exceptions that take a territorial approach seek to account for the country’s needs without ignoring each node’s progressive and objective growth.
Discussion
The objective of this study was to build an action plan for the development and integration of palliative care into the Colombian health system. The method used for this purpose was participatory action research involving different stakeholders. This research method has been previously employed by Schneider et al. 27 who interviewed 442 stakeholders from different levels of the German health system to gain insight into their perspectives on the barriers to palliative care. May et al. 28 also used the participatory action research method to analyze Ireland’s palliative care action plan and the level of development of palliative care. Recently, Centeno et al. 29 published a consensus known as the PAL-LIFE White Paper that proposes involving stakeholders in decision-making as an advocacy strategy for the development of palliative care. Our work retrieved these initiatives and implemented them sequentially for the stakeholders to learn about, analyze, and propose an action plan for palliative care for 2026. Other methodologies use international literature, international experts, government processes, universal barriers, or comparative analysis between national strategies to build palliative care plans. 30 However, it has not yet been determined which of these methodologies yields the best results.
The results of our work agree with previous studies’ findings and shed light on the inequity of palliative care provision. 31 – 33 The most relevant finding was the comparison between the level of palliative care development and territorial palliative needs. This result shows Colombia’s considerable and shared need for palliative care, despite the scarce availability and unfair distribution of palliative care among the regional nodes. Another important finding was the commonality that seven barriers were identified in all the regional nodes, and many of them coincide with the barriers recently indicated in the second edition of the Atlas of Palliative Care in Latin America. 34 Especially in the dimension of palliative care education, formal educational programs are scarce in relation to palliative care needs; for this reason, a greater number of additional proposals were received to be included in the strategic actions for this dimension. A comparative analysis of health personnel education in Latin America corroborates this need, reporting one specialist per 1.5 million inhabitants. 35 Qureshi et al. 36 demonstrated that palliative care education is a determining factor for integrating palliative care into the Canadian health system. Other research groups’ analyses of the Colombian health system have also shown that the lack of education has been one of the leading causes of the stagnation of palliative care development. 37 These and other common deficiencies represent a challenge and an opportunity for the countries of the region to make a joint effort to overcome these barriers.
The action plan presented responds to the current situation and empowers stakeholders to prioritize their needs and become involved in decision-making to ensure a path of equity. 38 Nonetheless, our study has three limitations. Despite our best efforts to include as many stakeholders as possible through continuous and follow-up email messages, only a moderate number of stakeholders participated, which could potentially impact the implementation process of the national plan. Several participants highlighted the presence of significant variations in the development of palliative care within the nodes, which are not adequately captured by the division used in this study. Further research is warranted to explore a more refined territorial classification of Colombia. An alternate division may enable more precise and accurate results regarding the territorial differences in palliative care. Although government and scientific representatives were involved in the phases, neither a budget nor a delegate responsible for coordinating the implementation of the action plan was assigned, a shortcoming pointed out in previous national strategies. 20 These limitations and difficulties are intended to be overcome through the ongoing future work led by the OCCP, which seeks to report and monitor the action plan that Colombia has drawn up to integrate palliative care into the health system.
Conclusion
Public health is facing an exponentially growing crisis of suffering. The WHO and international palliative care organizations have called on countries to lead efforts to develop action plans aimed at achieving universal palliative care through PHC and community empowerment. Using participatory action research, the capacities and barriers of the Colombian territory were identified. The data were synthesized into actions and objectives that were evaluated publicly and locally by stakeholders from all over the country. Finally, development goals in palliative care were agreed upon. This construction process carried out by stakeholders resulted in the Colombian National Palliative Care Plan for 2026. The following research method directly involves those responsible for the compliance of the plan and guarantees stakeholders’ involvement in the achievement of the project, which, in short, aims to solve the territorial inequity in palliative care that currently exists in this country.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231189520 – Supplemental material for Building an action plan to tackle palliative care inequality through multi-stakeholder platforms
Supplemental material, sj-docx-1-pcr-10.1177_26323524231189520 for Building an action plan to tackle palliative care inequality through multi-stakeholder platforms by Miguel Antonio Sánchez-Cárdenas, Marta Ximena León-Delgado, Luisa Fernanda Rodŕguez-Campos, Juan Esteban Correa-Morales, Laura Vannesa Gonźlez-Salazar, Ángela María Cañón Piñeros, Genny Paola Fuentes-Bermúdez and Lina María Vargas-Escobar in Palliative Care and Social Practice
Footnotes
Acknowledgements
We are grateful to all regional palliative care stakeholders who participated in building the Colombian national palliative care plan.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.