
Abstract
Background:
Medical assistance in dying (“MAiD”) became legal across Canada in 2016, and in Québec in 2015. Provincial/territorial regulatory bodies play a critical role in MAiD as they can issue binding requirements on health practitioners. Law and regulatory standards are the “twin pillars” of MAiD regulation, yet the content of MAiD practice standards for physicians is unstudied.
Design:
This article analysed MAiD guidance for physicians from Canadian medical regulators (often called the “College of Physicians and Surgeons”), using a qualitative descriptive approach, informed by regulatory space theory.
Methods:
We identified MAiD-specific regulatory documents (practice standards and related documents) using web-based searches and follow-up inquiries. We analysed the documents using qualitative descriptive analysis and the Framework Method, facilitated by NVivo. The analysis focused on identifying areas where regulators issued guidance beyond the law.
Results:
We identified 15 regulatory documents from 11 of the 13 provinces and territories. We determined that these documents primarily outline the law without detailed guidance on how to apply it. We identified eight areas for which regulators provided guidance that went beyond the MAiD-specific legislation, most relating to core aspects of medical practice, such as competency, documentation, and patient-centred care. The rights and obligations of conscientious objectors were a predominant focus in all documents. The documents largely lacked guidance about the meaning of terms in the legislation. There was also variation in standards between provinces and territories; the documents focused on similar topics but varied in their policy choices. Physicians in each province/territory are therefore subject to differing expectations (to some extent).
Conclusion:
This study highlights a gap in guidance on the meaning of legal terms in the Criminal Code MAiD provisions and highlights interprovincial/territorial variability in MAiD practice standards and guidance for physicians. The study demonstrates the risks of fragmentation inherent in polycentric regulation, which can be challenging for physicians to navigate.
Plain language summary
In Canada, medical assistance in dying (MAiD) became legal in 2016, with Québec legalizing it in 2015. In each province and territory, regulatory bodies like the “College of Physicians and Surgeons,” play a key role in guiding physicians on how to carry out MAiD. However, there has been little research on regulators’ practice standards for physicians. This study examined MAiD-related guidance for physicians from Canadian medical regulators. We found 15 documents from 11 provinces and territories that were specific to MAiD. The goal was to see how these documents went beyond the law and provided additional requirements and advice on how to handle MAiD in practice. The results showed that most documents mainly restate the law, with limited extra guidance. However, there were eight areas where regulators offered advice that went beyond the legal requirements. These areas included medical competencies, proper documentation, and patient-centered care. One key focus in all documents was the rights of physicians who object to MAiD for personal or moral reasons. The study also found that the guidance varied between provinces and territories. While most documents covered similar topics, the specific expectations differed somewhat. This may create some confusion for physicians, as they may face different standards depending on where they practice. Overall, the study points out the lack of clear guidance on the meaning of certain legal terms and highlights the variation in MAiD regulation for physicians across Canada.
Keywords
Introduction
A growing number of jurisdictions, including the Netherlands, Belgium, Switzerland, Canada, Colombia, Spain, Germany, Austria, Portugal, New Zealand, 7 of 8 jurisdictions in Australia, and 11 jurisdictions in the United States, have legalized some form of assisted dying (“AD”). 1 AD involves a physician (or in some jurisdictions, a nurse practitioner) administering or prescribing a lethal substance to a patient who is suffering, at their request, to end their life.
Debates regarding AD are polarized, and jurisdictions around the world have engaged in significant deliberation about whether to permit it and in what circumstances. Beyond the question of whether to legalize AD, jurisdictions must also consider how to regulate it. What constitutes “regulation” is contested, and it is increasingly seen as broader than just law.
2
Regulatory scholar Julia Black defines regulation as: . . .the sustained and focused attempt to alter the behaviour of others according to defined standards or purposes with the intention of producing a broadly identified outcome or outcomes, which may involve mechanisms of standard-setting, information-gathering and behaviour-modification.
2
Modern scholars like Black see regulation as polycentric, involving state and non-state-based actors that interact in complex ways, using a range of mechanisms including law, policy, guidelines, ethical codes, training, and funding.2,3
AD regulation varies internationally both in its content and in the instruments used to steer behaviour. For example, Belgium and the Netherlands have concise legislation supplemented by other instruments, including professional standards and institutional ethics policies.4,5 Additionally, in Belgium, many healthcare institutions mandate patients requesting AD to consult with a specialized palliative care team, even though this requirement is not part of the AD legislation (known as the “palliative filter” norm). 5 The legislation in Australia, which varies by jurisdiction, is much more comprehensive. Each state and the Australian Capital Territory has a lengthy and prescriptive AD statute that governs each step of the AD process. 6 Nevertheless, some key issues, such as institutional objection in the state of Victoria, are left to policy.7,8 In Canada, criminal law is federal, while healthcare implementation (including the practice of AD) is the responsibility of the provinces and territories. 9 Canada’s AD regulatory system involves both law and professional practice standards, 10 which are supplemented by other mechanisms including regional health authority policies, 11 and professional association guidelines. 12
Given their binding nature, we can conceive of law and regulatory standards as the “twin pillars” of Canadian assisted dying regulation. There are two primary legal frameworks for medical assistance in dying (“MAiD”) in Canada (summarized in Table 1). Québec passed the Act Respecting End-of-Life Care (“AREOLC”) in 2014 after a robust civil society process, including the support of the medical regulator. 13 Federally, in 2016, the Canadian government passed Bill C-14 to amend the Criminal Code of Canada in response to the 2015 Supreme Court of Canada decision in Carter v. Canada. 14 After MAiD was legalized, many provincial and territorial health professional regulatory bodies issued MAiD-specific practice standards.15 –17
Overview of medical assistance in dying provisions in Canada’s Criminal Code and Québec’s AREOLC.
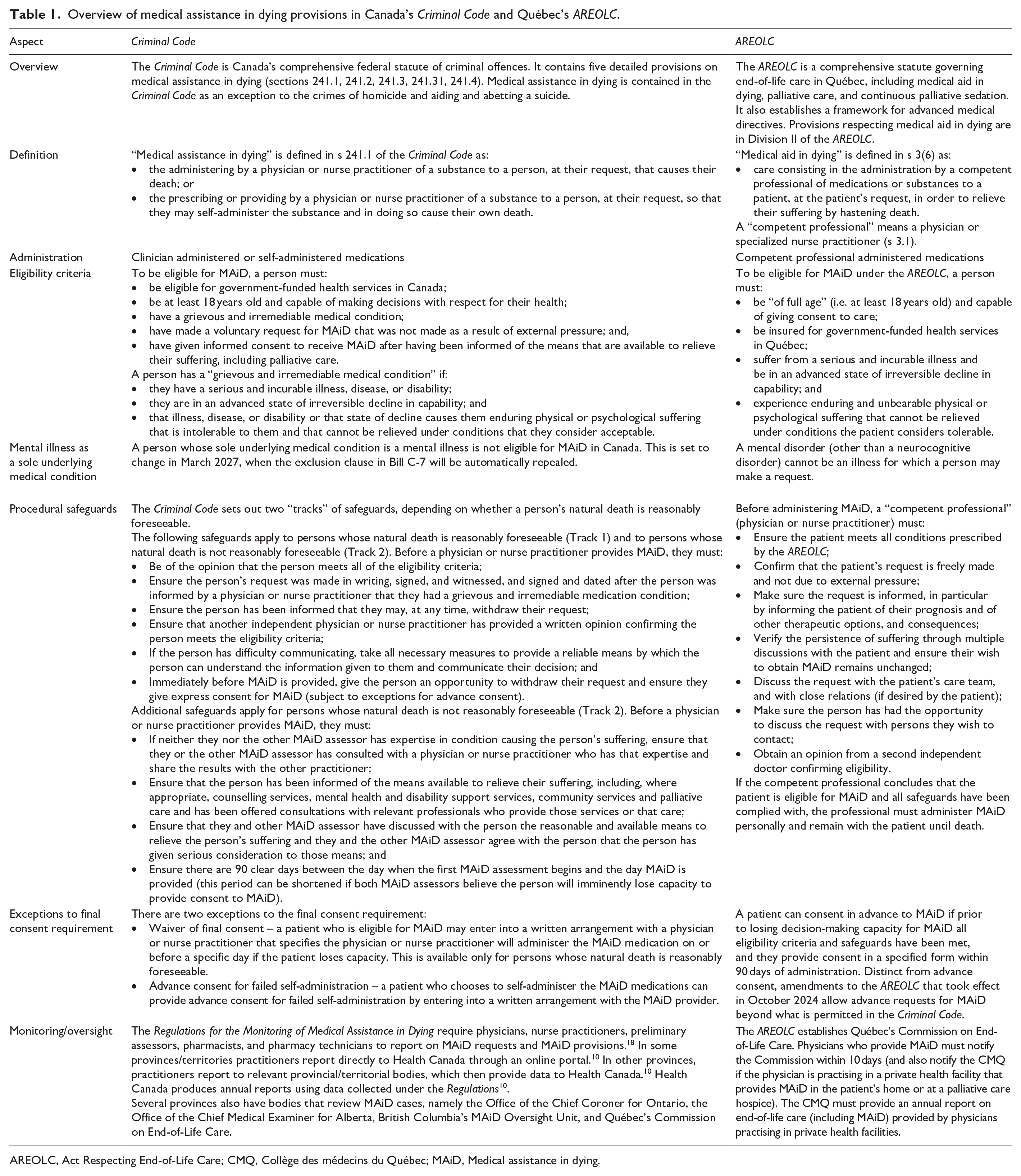
AREOLC, Act Respecting End-of-Life Care; CMQ, Collège des médecins du Québec; MAiD, Medical assistance in dying.
Research has tended to focus on MAiD law and its implementation,19 –25 with comparatively less attention paid to standards. Existing regulatory studies have examined guidance for nurses, 16 pharmacists, 17 health authority policies, 11 practices surrounding death certificates, 26 and rural considerations in regulatory documents. 27 These studies have found that, like other healthcare practices, there is considerable variation in how each province and territory regulates MAiD, a function of Canada’s federated structure.11,15,16,28 Some argue that variation in regulation by province and territory is problematic; it wastes resources, and may confuse health professionals and the public.29 –31 On the other hand, regulatory variation may reflect and be responsive to the specificity of jurisdictional needs and priorities.
To our knowledge, there is no research to date on MAiD regulatory documents for physicians in Canada. This is an important gap to fill. Physicians and nurse practitioners are the only two professions authorized to assess and provide MAiD, with physicians providing the majority of MAiD procedures (90.6% in 2022). 10 Non-compliance with practice standards is serious; it can subject physicians to investigation and discipline, up to and including the loss of their licence to practice. 13 Additionally, as illustrated by a 2018 legal case challenging the Ontario College of Physicians and Surgeon’s “effective referral” requirement for objecting physicians, the framing of practice standards can directly impact patient access to MAiD. 32 Canada’s regulatory approach of law scaffolded by practice standards may also provide insights for other countries considering or implementing AD, particularly those that have some separation of regulatory authority, such as Australia.
This article examines practice standards and related documents (i.e. “regulatory documents”) issued by each Canadian province and territory’s medical regulator. As a threshold point, we note that while there is a diversity of opinions on whether MAiD should be permitted, and in what circumstances, this article steps beyond these discussions and recognizes that MAiD is now legal in Canada. The aim of this article is to investigate how medical regulators have responded to the law and what guidance they have provided to physicians. The study investigated three key research questions:
(1) What MAiD-specific regulatory documents have been released by provincial/territorial medical regulators?
(2) For which topics do these documents aim to regulate behaviour beyond legal obligations?
(3) Does this content vary across provinces and territories, and if so, how?
Regulation of the medical profession in Canada
In Canada, the medical profession is self-regulating. With some exceptions, each province and territory has delegated the authority to regulate physicians to “Colleges,” 33 non-profit corporations empowered by legislation to act as the governing professional organization (in the Yukon, the regulator is called the Yukon Medical Council rather than a “College”; Table 2). The Northwest Territories and Nunavut do not have Colleges; the government is the regulatory authority. This article refers to these bodies as “regulators.”
Canadian medical regulators by jurisdiction.
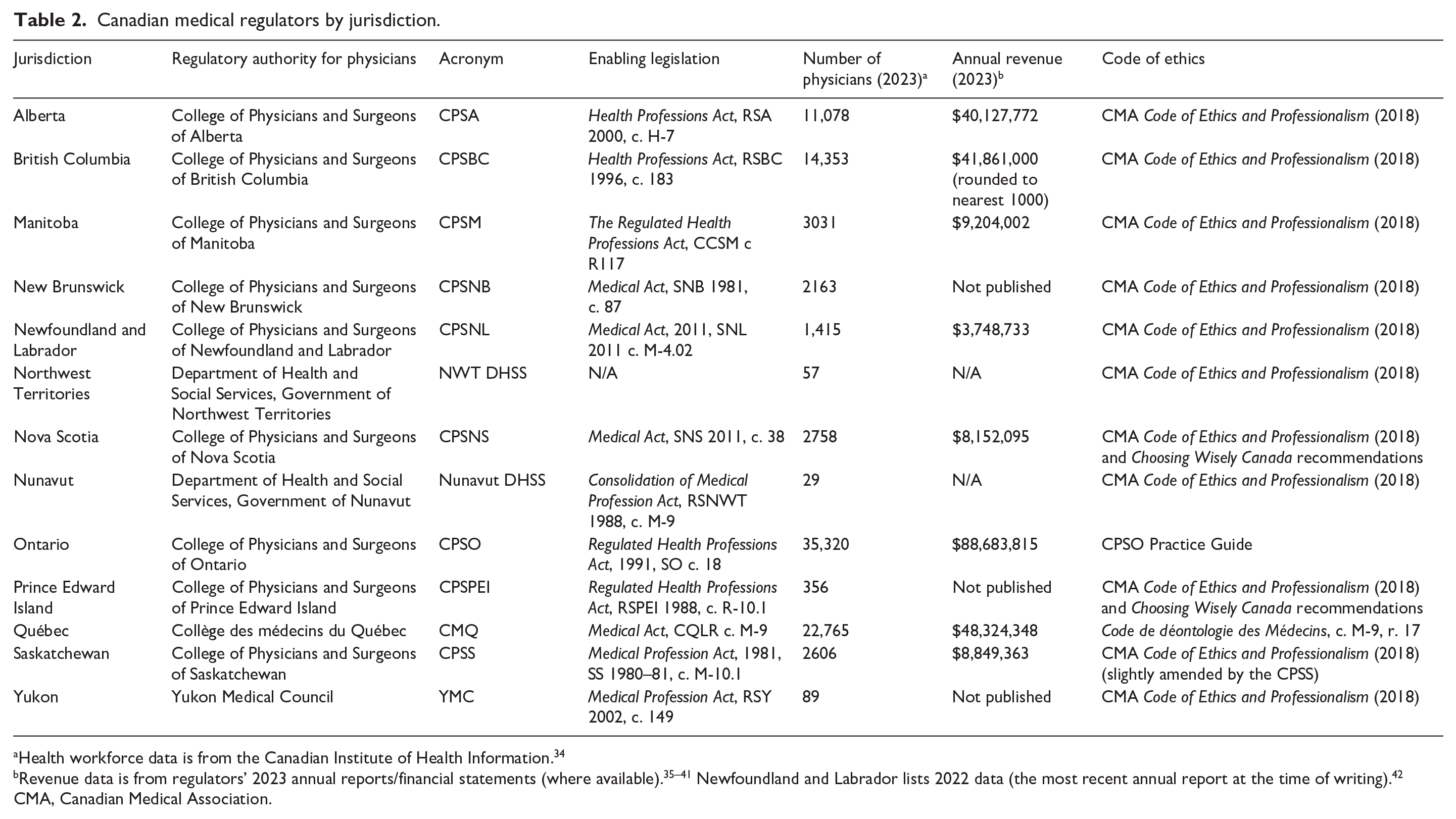
Health workforce data is from the Canadian Institute of Health Information. 34
Revenue data is from regulators’ 2023 annual reports/financial statements (where available).35 –41 Newfoundland and Labrador lists 2022 data (the most recent annual report at the time of writing). 42
CMA, Canadian Medical Association.
Most regulators have a similar governance structure determined by legislation, with a board (or council) as the primary governing and standard-setting body, and committees that have powers and duties exercised on behalf of the board. The size and budget of each regulator varies widely (Table 2). The regulator is responsible for: licensing postgraduate medical trainees and physicians; setting policies, guidelines, and standards for safe and ethical practice; and responding to complaints from the profession and the public, including conducting investigations and hearings, and disciplining members who fail to meet the regulator’s standards and expectations. 13
The central mandate of the regulators, like other professional regulatory bodies, is to promote and protect the public interest. For example, Alberta’s Health Professions Act, RSA 2000, c. H-7 states a College “must carry out its activities and govern its regulated members in a manner that protects and serves the public interest”.43, 44 This public interest mandate distinguishes the regulators from medical associations, which are focused on representing member interests, and professional societies, which are focused on supporting learned activities. 13 To practice medicine in a province or territory, a physician must be licensed by the regulator. The effect of this is that regulators are powerful agents in shaping practice behaviour: recognized by law, they set standards that all practising physicians must comply with and possess the power to sanction non-compliance, including preventing a physician from practising medicine.
Most Colleges limit their role to the regulatory functions of licensing, quality assurance, and discipline, and leave advocacy, position-taking, and collective bargaining with the government to provincial/territorial medical associations. 13 Notably, the Collège des médecins du Québec (CMQ) has a more active role than its counterparts in other provinces and territories. 13 It takes positions in the media and has its own Code de déontologie as a disciplinary standard.
The regulators guide medical practice using a range of instruments, including codes of ethics45,46 and standards (called “standards of practice” or “policies”), which set out the minimum requirements and recommendations across a range of practices. For example, the College of Physicians and Surgeons of Alberta has over 40 standards of practice on issues ranging from prescribing to maintaining patient records to relationships with industry and patients. 47 The requirement to develop standards is set out in legislation (e.g., Ontario’s Regulated Health Professions Act, 1991, SO 1991, c. 18 states that the objects of the College include: developing, establishing, and maintaining standards of professional ethics and standards of practice 48 ). The purpose of standards is to “assure the quality of the practice of the profession,” 47 and to “reduce incompetent, impaired or unethical practice amongst registrants.” 49 Regulators also develop companion documents, under a variety of labels including “guidelines,” “guidance,” or “advice to the profession,” which do not require board approval. While physicians must comply with standards of practice or risk discipline, companion documents do not carry this same weight. Although they are endorsed by the regulator and are recommended practices that physicians should adopt, physicians may choose whether/how to take them into account.
Method
Analytical framework
This study is a qualitative content analysis of MAiD regulatory documents for physicians. It is part of a broader project that aims to develop an optimal holistic model for AD regulation, 50 premised on Black’s broad definition of “regulation” 2 and “regulatory space” theory, which suggests actors and their regulatory tools interact to shape behaviour.3,51
We defined “regulatory documents” as documents that set standards and offer physicians MAiD-specific guidance. We included supplementary documents like “advice to the profession” statements, as they inform the interpretation of practice standards and can be considered a component of standard-setting. We excluded general medical practice standards from our analysis (e.g. those pertaining to informed consent), as the focus was on MAiD-specific standards. It is important to emphasize, however, that MAiD-specific standards are situated in a network of relevant general medical practice standards, to which all MAiD assessors/providers are expected to adhere. This is reinforced by the Criminal Code, which states in s 241.2(7): “Medical assistance in dying must be provided with reasonable knowledge, care and skill and in accordance with any applicable provincial laws, rules or standards.”
Search strategy
The authorial team was comprised of three legal academics and a psychiatrist, all with MAiD-related regulatory expertise. Regulators were identified through legislative review (Table 2). We employed a two-stage search strategy: (1) searches of each regulator’s website and grey literature; and (2) email inquiries (where required). The lead author (EC) searched each regulator’s website for current MAiD regulatory documents using drop-down menus and a variety of search terms individually and in combination, including: medical assistance in dying, MAiD, standards of practice, guidance, policy, advice, advice to the profession, and FAQs. Repeated searches were conducted from April 2022 and were finalized on 1 September 2023. EC also identified and examined relevant literature to triangulate searches on medical regulator websites.
EC located publicly available regulatory documents on medical regulator websites in each province and territory, except Québec, New Brunswick, and Nunavut. In these provinces, EC followed up with email inquiries. In Québec, the CMQ provided its MAiD policy. On 12 October 2022, EC again emailed the relevant regulators in New Brunswick and Nunavut to request any MAiD regulatory documents but received no response (these jurisdictions do not have a MAiD standard).
Analysis
For context, the research team reviewed the mandate of each regulator as set out in the relevant legislation (Table 2) and as stated on their websites, noting the contrast between the CMQ and counterparts in other provinces and territories. The research team also drew on their expertise with Criminal Code provisions to identify aspects of the documents that reflected the law versus aspects that went beyond the law.
All documents were uploaded into NVivo qualitative data analysis software (release 1.6, QSR International). We employed Sandelowski’s qualitative descriptive analysis, 52 which has been used in previous studies of nursing and health authority regulatory documents.11,16 This approach produces “thematic surveys,” with the analysis and interpretation of the findings remaining descriptive and “data-near.” 52 To manage the data, we used the Framework Method of qualitative content analysis, a method increasingly used in policy studies to code and systematically chart data into a matrix to facilitate comparison and analysis.53,54
EC conducted the initial analysis. EC read all documents in full and then coded each one, focusing on elements that were not merely a restatement of the law, but rather new obligations or guidance from the regulator. Based on discussions with all authors and reference to EC’s reflexive journal created while coding, EC grouped codes into themes. EC then charted the data into a matrix to aid in comparison and analysis. The authors iteratively discussed the matrix and refined the final themes. The manuscript was written in accordance with the SRQR reporting guidelines (Supplemental Material). 55
Results
Sample of regulatory documents and their characteristics
We identified 15 regulatory documents on MAiD from 11 regulators (Table 3). The regulatory documents were labelled:
standards of practice (seven documents);
policy (four documents; which effectively function as standards);
guidelines (one document); and
advice to the profession (three documents).
The documents ranged from 4 to 102 pages (median = 12 pages) and had reasonably consistent style. Most documents were between 4 and 17 pages and focused on legal requirements and professional expectations for physicians. In contrast, documents from Québec and the Northwest Territories were considerably longer, at 102 pages and 35 pages, respectively.56,57 The Northwest Territories document was addressed to multidisciplinary teams, not just physicians. 57 The Québec document contained much more clinical guidance than the other jurisdictions and referenced a medication protocol developed by the Institut national d’excellence en sante et en service sociaux (“INESSS”), at the CMQ’s request (this document is in a “restricted access” section of the INESSS website, which one of the authors (M.G.) had access to by virtue of being a physician licensed in Québec). 58 The documents cross-referenced other sources including College standards and ethical codes.
Overview of provincial/territorial medical regulatory documents on medical assistance in dying.

The College of Physicians and Surgeons of Ontario (CPSO) issues “policies,” “statements,” and “positions.” It indicates policies: “set out expectations for the professional conduct of physicians practising in Ontario.” 58 Advice to the profession documents “are intended to provide physicians with additional information and general advice in order to support their understanding and implementation of the expectations set out in policies.” 59 In Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393, the Ontario Court of Appeal noted at paras (15)–(16) that the CPSO’s MAiD policy and another related policy: “are not ‘regulations’, nor are they a ‘code, standard or guideline relating to standards of practice of the profession’ adopted pursuant to s. 95(1.1) of the Health Professions Procedural Code, Schedule 2 of the RHPA [the Regulated Health Professions Act, 1991, SO 1991, c. 18]. Accordingly, non-compliance with the Policies is not an act of professional misconduct under the College’s professional misconduct regulation: Professional Misconduct, O. Reg. 856/93. However, the Policies establish expectations of physicians’ behaviour and are ‘intended to have normative force’. As such, they may be used as evidence of professional standards in support of an allegation of professional misconduct.” 32
The CPSPEI issues “policies” and “guidelines.” It indicates policies: “reflect the minimum professional and ethical behaviour, conduct or practice expected by the College of Physicians and Surgeons of PEI. Physicians licensed with the College are required to be familiar with and comply with the College policies.” 60
The CMQ’s regulatory document was on a secure website and was only available to the public on request. At the time of the analysis, there were two versions of the CMQ’s document, one in French (updated November 2019) and one in English (updated April 2018).55,61 The foreword to the document in French indicates that the November 2019 updates concerned revisions to discrete areas: obtaining medicines and dealing with the pharmacist; the medical prescription; clarifications regarding administration of the MAiD substance; and updates to forms. 61 In May 2022, the pharmacological guidelines of the November 2019 update were replaced by a new national medical protocol developed by INESSS at the CMQ’s request. 57 On 24 January 2023, the CMQ confirmed via email correspondence that the English version of the CMQ regulatory document contains the same content the document in French, but for the updates listed in the foreword. Given the lead author of the study is English-speaking, and the updates were only to these discrete areas, the analysis was conducted using the English version of the CMQ document. The lead author also reviewed a DeepL English translation of the French version to check for any unique content relevant to this analysis.
The CPSS uses policy to set out expectations of the College for physicians practising in Saskatchewan.62,63
CMQ, Collège des médecins du Québec; CPSA, College of Physicians and Surgeons of Alberta; CPSBC, College of Physicians and Surgeons of British Columbia; CPSM, College of Physicians and Surgeons of Manitoba; CPSNL, College of Physicians and Surgeons of Newfoundland and Labrador; CPSNS, College of Physicians and Surgeons of Nova Scotia; CPSO, College of Physicians and Surgeons of Ontario; CPSPEI, College of Physicians and Surgeons of Prince Edward Island; CPSS, College of Physicians and Surgeons of Saskatchewan; MAiD, medical assistance in dying; NWT DHSS, Department of Health and Social Services, Government of Northwest Territories; YMC, Yukon Medical Council.
Our analysis focused on obligations beyond the law, but we note that all documents included information about the law. The legal content was descriptive; the documents generally avoided interpreting or defining legal terms, instead referring physicians to seek legal advice if unsure (although a few documents did define key legal terms, discussed further in Theme 4). Uniquely, the CMQ’s document was designed to help clinicians reconcile the federal law in the Criminal Code and the AREOLC (both apply in Québec).56,62 As of 1 September 2023, most documents (13/15) had incorporated the 2021 amendments by Bill C-7 amendments to the Criminal Code.
Consistent with the regulators’ mandate, the documents stated their purposes were to:
provide information on legal and procedural requirements for MAiD (for physicians and the public); and
set out the law and guidance about physicians’ professional responsibilities.
We identified eight themes involving guidance and additional standards beyond the law (Table 4). Key aspects where the documents aligned and varied are set out in Table 4.
Topics that Canadian medical regulators have issued guidance on regarding medical assistance in dying.

MAiD, medical assistance in dying.
Theme 1: Balancing patient access with physicians’ objections to MAiD
All documents addressed conscientious objection, a refusal to participate because of personal, moral, or religious convictions. Nova Scotia referenced “non-participation,” encompassing conscientious objection and “various practical reasons such as lack of availability or lack of expertise.” 65
The Criminal Code indicates in s. 241.2(9): “. . . nothing . . . compels an individual to provide or assist in providing medical assistance in dying.” 66 Section 50 of the AREOLC requires objecting physicians to “ensure continuity of care for the patient. . ..” 67 The regulators had additional expectations of physicians who conscientiously object or are unable or unwilling to participate (Table 5). All documents emphasized that physicians’ conscience must be balanced against patients’ interests.
a. Fostering patient access to MAiD: Regulators varied in their expectations of objecting physicians (Table 5). There were three broad approaches. First, some only required physicians to provide patients with information.61,63,64,68 Second, some required physicians to connect the patient with a care coordination service (not all provinces/territories have care coordination services).57,69 Third, some required physicians to provide “timely access to a resource”70,71 or make an “effective transfer of care” or “effective referral.”56,59,60,65,72,73
Expectations varied somewhat in the third category, despite similar language. For example, the Manitoba document instructed physicians to provide: “timely access to a resource [such as other registrants, healthcare providers, and publicly available resources] that will provide accurate information about MAiD.” This aligns with provincial legislation which confirms that professional regulatory bodies in Manitoba cannot require participation: “a professional regulatory body must not make a regulation, by-law, rule or standard that requires a member of the regulated profession to provide or aid in the provision of medical assistance in dying”71, 74 British Columbia and Nova Scotia required an “effective transfer of care”: . . .advising patients that other practitioners may be available to see them, suggesting the patient visit an alternate physician or service, and if authorized by the patient, transferring the medical records as required.
72
In Nova Scotia, “effective transfer of care” also requires the practitioner to transfer the patient to a person who is willing to accept the transfer and provide MAiD (so long as eligibility criteria are met).
65
Similarly, Ontario indicated physicians must make an “effective referral” (the only regulator to use the word “referral”): . . .positive action to ensure the patient is connected in a timely manner to a non-objecting, available, and accessible physicians, other health-care professional, or agency that provides the service or connects the patient directly with a health-care professional who does.59,60
Six medical regulators explicitly required the physician to transfer the patient’s records (Table 5).
b. Communication by conscientious objectors and other non-participants: The documents commonly required: disclosing the objection; not promoting one’s own values or beliefs; and communicating sensitively and with respect (Table 5). A few documents indicated physicians must not provide false, misleading, coercive, or incomplete information.59,61,63,64,68 Several instructed physicians to communicate their objection promptly, to ensure the patient’s access to MAiD is not impeded.63,64,69,71 Nova Scotia uniquely required non-participating physicians to provide patients with a copy of its standard of practice. 65
c. Continuity of care other than MAiD: Many of the documents emphasized the physician’s duty of care to the patient. A common edict was that a patient must not be abandoned, must not be discriminated against, and must be treated with respect (e.g. Saskatchewan) (Table 5).63,64 Some documents were more specific and required physicians to continue to provide care unrelated to MAiD, provided the patient consents, unless alternative arrangements are in place (e.g. Québec, Prince Edward Island, Nova Scotia, Manitoba).56,61,65,71 In Newfoundland and Labrador this was recommended, not mandatory. 68
d. Limits on conscientious objection: Québec indicated that physicians who are consulted by a MAiD assessor regarding a patient’s capacity or degree of suffering are not permitted to claim a conscientious objection as this would be discriminatory. 56 Québec also stated that a physician with a conscientious objection to MAiD administration should not provide a MAiD assessment. 56
Overview of obligations to patients requesting MAiD for physicians who have a CO.

CMQ, Collège des médecins du Québec; CO, conscientious objection; CPSA, College of Physicians and Surgeons of Alberta; CPSBC, College of Physicians and Surgeons of British Columbia; CPSM, College of Physicians and Surgeons of Manitoba; CPSNL, College of Physicians and Surgeons of Newfoundland and Labrador; CPSNS, College of Physicians and Surgeons of Nova Scotia; CPSO, College of Physicians and Surgeons of Ontario; CPSPEI, College of Physicians and Surgeons of Prince Edward Island; CPSS, College of Physicians and Surgeons of Saskatchewan; MAiD, medical assistance in dying; NWT DHSS, Department of Health and Social Services, Government of Northwest Territories; YMC, Yukon Medical Council.
Theme 2: Ensuring requisite care, knowledge, and skill
The Criminal Code indicates in s. 241.2(7) that MAiD “must be provided with reasonable knowledge, care and skill and in accordance with any applicable provincial laws, rules or standards” (there is no equivalent provision in the AREOLC). 66 Regulators focused on: (a) defining core competencies; (b) knowledge building; and (c) limits on who can practice MAiD. Overall, as in other areas of medical practice, the regulators gave physicians discretion in how they fulfil knowledge and competency requirements.
a. Defining core competencies: Core competencies for MAiD assessors/providers included assessment (e.g. of capacity, and of whether the person has a grievous and irremediable medical condition), and technical aspects (i.e. medication prescription and administration). Québec uniquely noted the physician must also have “soft skills.” 56 Guidance regarding assessments was framed broadly; MAiD assessors must take all relevant information into account and use a “reasonable method of assessment.” 71 Physicians must exercise “professional judgement,” “common sense,” and “good faith” when conducting an assessment (e.g. Newfoundland and Labrador, Ontario, Québec56,59,68), which aligns with their legal duty of care to the patient, as well as protections in the Criminal Code for those who provide MAiD in good faith.
b. Knowledge building and skill development: A few documents recommended training and education on MAiD from government agencies, 72 or “reputable sources” such as the Canadian Medical Association (“CMA”). 68 Other documents were silent regarding training but encouraged physicians to seek out best practice guidelines from professional organizations, such as those from the Canadian Association of MAID Assessors and Providers (“CAMAP”). 60 The Northwest Territories guidelines uniquely “strongly encouraged” all practitioners involved in MAiD to join CAMAP. 57
c. Limits on who can practice MAiD: Some documents restricted who can practice MAiD. Saskatchewan’s documents required authorization from the Saskatchewan Health Authority or the College.63,64 Others documents explicitly excluded residents or trainees (e.g. Québec 56 ), or permitted them in “an assisting or learning capacity only” (Newfoundland and Labrador) 68 or within their registration limits (Ontario 59 ). Several documents required at least one assessor to be licensed in the province/territory in which MAiD was provided (e.g. British Columbia). 72
Theme 3: Facilitating patient-centred decision-making and care
Guidance on facilitating patient-centred decision-making and care related to five distinct aspects. These centred on who to involve and the practical aspects of MAiD provision.
a. Framing roles and responsibilities: The Criminal Code requires two independent physicians and/or nurse practitioners to assess MAiD eligibility and confirm compliance with procedural safeguards. The documents emphasized physicians’ duty to deliver patient-centred MAiD within a broader team or family context (a particular focus for Québec). This was framed as acting as a “navigator” 65 or central point of communication between the patient, the patient’s family, and care coordination services. 68
b. Understanding the patient’s circumstances and perspective: Physicians who receive MAiD requests were instructed to explore the patient’s “circumstances, perspective and reason for contemplating MAID” (e.g. Alberta, Newfoundland and Labrador, Québec56,68,69). However, only Manitoba, Saskatchewan, and the Northwest Territories specifically referred to the patient’s cultural and religious beliefs.57,63,64,71
c. Reducing unnecessary delay: The documents required avoiding delays, which would prolong the patient’s suffering. For example, physicians must assess the patient “expeditiously,”65,68 and notify the pharmacist of the MAiD prescription as soon as possible.56,59,61 Those with a conscientious objection must notify the patient in a “timely”59,60,68,70,71 way or “immediately.” 56
d. Involving family and other caregivers: The AREOLC (s. 29(1)(e)) indicates physicians must discuss the MAiD request with the person’s close relatives or any other person (if the patient wishes; the Criminal Code is silent on this). 67 This was discussed in the Québec document. 56 Several other documents encouraged involving family members, friends, or spiritual advisors, with the patient’s consent. The family can provide information to inform assessments (e.g. in relation to suffering). 72 Additionally, Ontario noted it is preferable to inform the family of any final consent waiver “to avoid potential conflicts” when MAiD is provided. 60
e. Involving care coordination and multidisciplinary teams: In some provinces and territories, contact with the provincial/territorial care coordination service was mandatory56,67,68; in Manitoba this was “strongly encouraged” (not all jurisdictions have care coordination structures). 70 Multidisciplinary teams and interdisciplinary support groups (which have a special status in Québec) were strongly emphasized in the Québec document, which recommended health and social services professionals seek consensus about the patient’s eligibility as much as possible (although the decision about MAiD eligibility is ultimately the assessing practitioner’s). 55
f. Developing a plan for MAiD provision/death: Some regulators required physicians to collaborate with patients to develop a plan for MAiD provision and death (e.g. Alberta, Québec56,69). Prince Edward Island’s document used less patient-centred language: the MAiD provider must “decide on the appropriate venue.” 61 Some regulators also addressed self-administration (which is very rare in Canada, and not permitted under the AREOLC 10 ). For example, the Ontario and the Northwest Territories documents required the physician to help the patient and family assess feasibility of self-administration.57,60 Alberta’s documents uniquely mandated physicians to complete an Alberta Health Services Goals of Care Designation order for persons seeking MAiD (a form of advance care planning).69,75 This would ensure that patients who are pursuing MAiD are not resuscitated or offered other life-sustaining treatments against their wishes, supporting a coherent end-of-life plan.
Theme 4: Assisting physicians to satisfy legislative criteria and safeguards
The Criminal Code and AREOLC establish eligibility criteria and procedural safeguards for MAiD (Table 1).66,67 The documents provided guidance on seven distinct areas related to the legislative criteria and safeguards.
a. Interpreting legal terms: A few documents provided limited guidance on legal terms like “reasonably foreseeable natural death.” For example, Nova Scotia and Ontario referenced the leading case, AB v. Canada, 2017 ONSC 3759: “. . .natural death need not be imminent and that what is a reasonably foreseeable death is a person-specific medical question to be made without necessarily making, but not necessarily precluding, a prognosis of the remaining lifespan.”60,65 Regulators also provided limited guidance on “expertise.” If a patient’s natural death is not reasonably foreseeable, at least one of the MAiD assessors must have expertise in the condition that is causing the person’s suffering, or they must consult someone who does. Some regulators clarified this “expertise” can be gained through experience, training, or education (e.g. Alberta, British Columbia73,75). The documents did not address “serious and incurable” or “advanced state of irreversible decline in capability” (elements of “grievous and irremediable condition”; Table 1).
b. Assessing capacity: Québec provided the most detail regarding capacity assessment for MAiD. Other regulators were more general, instructing physicians “to rely on existing practices. . .,” 59 and existing standards on capacity and consent. Some regulators required a psychiatric referral if the physician is uncertain about capacity (e.g. British Columbia, Mantioba, Prince Edward Island).61,71,72 Québec indicated this is “often required” if a patient has a psychiatric disorder or dementia. 56
c. Discussing options and alternatives as part of informed consent: Physicians have legal obligations to offer appropriate resources as part of informed consent. Regulators left the choice of services largely to physicians’ discretion. For example, physicians must provide information and referral to “any other service that may be of benefit” 68 and/or “appropriate counselling resources.”61,71 The Ontario Advice to the Profession also notes Health Canada advises MAiD providers to “take great care” if a person is proceeding with MAiD due to delays in accessing desired services/treatments. 60
d. Assessing suffering: The Québec document was the only one to provide guidance for assessing (and responding to) suffering. It noted that although suffering is subjective, the physician may use symptom assessment scales and collaborate with the interdisciplinary team using an “intersubjective approach.” 56
e. Ensuring voluntariness: Some regulators required a physician to meet with the patient at least once alone (e.g. Manitoba, Northwest Territories, Saskatchewan57,63,64,71). Québec indicated that physicians should use caution if a person is not near the end of life, and “verify that MAID is not being requested for relational, social or economic reasons.” 56 The documents provided little to no guidance about raising MAiD as an option. A few indicated (in the context of conscientious objection and more generally) that the regulators expect physicians to provide patients with sufficient information to make informed choices (e.g. British Columbia 72 ) and must be read in conjunction with other standards on informed consent (e.g. Nova Scotia 65 ). While this arguably requires physicians to bring up MAiD as an option, the documents did not explicitly discuss raising MAiD. The Northwest Territories interim guidelines cautioned physicians that when providing lawful information about MAiD, they “must exercise extreme caution to ensure they do not recommend, incite, or encourage” MAiD as this would constitute a criminal offence. 57
f. Referrals to other practitioners to inform assessments: As noted, several regulators required referral for a capacity assessment (e.g. from a psychiatrist) if the physician is unsure (or had “reasonable doubt” 71 ) whether the person had the requisite decision-making capacity (e.g. Ontario, Prince Edward Island, Saskatchewan59,61,63,64). Newfoundland and Labrador mandated referral for all patients if neither the assessor nor provider has expertise in the condition causing the person’s suffering (this is required by the law only for patients whose natural death is not reasonably foreseeable) 68 . In a somewhat less directive vein, Alberta indicated a psychiatric or psychological referral was “strongly advised” if a patient requesting MAiD had an underlying mental health condition. 69
f. Virtual consultations: MAiD assessments using telehealth are not addressed in the law but were mentioned in certain documents. British Columbia permitted both physicians’ assessments to occur virtually using quality video provided another regulated health professional is physically present. 72 Ontario required that physicians must contemplate the suitability of virtual tools on a situational basis and recommended consulting guidelines from organizations like CAMAP. 60
Theme 5: Safe and effective MAiD provision
The Criminal Code (s. 241.2(8)) requires the MAiD provider to notify the pharmacist that the medication is intended for MAiD (to enable them to refuse to be involved and to enable arrangements to be made to ensure timely access to the medications). While the Criminal Code and the AREOLC define MAiD, they do not regulate the medication protocol or other steps related to provision. The regulatory documents focused on medication prescribing and MAiD provision. This was a pronounced focus in Québec, which incorporated the detailed INESSS protocol.56,58
a. Medication prescribing and management: The documents discussed prescribing, dispensing, and return of the MAiD medications. Some jurisdictions required physicians to follow medication protocols set by their province or territory,56,69 while others gave physicians discretion regarding the protocol (e.g. Northwest Territories, Yukon57,70). Some regulators instructed physicians to collaborate with the pharmacist on the appropriate protocol (e.g. Yukon). 70
b. MAiD provision: Guidance regarding MAiD provision varied. Nova Scotia instructed physicians to review all documentation before providing MAiD. 65 Regulators also required physicians to remain present until death is declared (i.e. a legal requirement in Québec under the AREOLC but is not mandated by the Criminal Code). Several jurisdictions required physicians to be present for self-administration57,63,64,68,72; in others it was “strongly encouraged.” 75 The Northwest Territories required physicians to inform a patient who is contemplating self-administration that they are required to provide advance consent for failed self-administration. 57
Theme 6: Documentation and accountability
Regulators emphasized thorough documentation and compliance with accountability mechanisms to protect the patient, the physician, and the public.
a. Thorough documentation: While there are no specific documentation duties in the Criminal Code, the AREOLC (s. 32) requires all information and documents associated with a MAiD request, regardless of whether MAiD is provided, to be “recorded or filed” in the medical record. 67 All regulators required physicians to carefully and meticulously document the MAiD process. Newfoundland and Labrador’s document indicated failure to comply with record-keeping “will be treated as a serious matter.” 68 Documentation was seen to help physicians “demonstrate compliance with the Criminal Code.” 60 Some documents instructed physicians to document that they have met all steps in the College standards (e.g. Alberta, Nova Scotia).65,69
b. Reinforcing accountability mechanisms: The Criminal Code regulations require physicians to report MAiD data to the federal government (directly or through a “designated recipient,” typically the provincial/territorial health department). 18 In some provinces, such as Ontario and Québec, the designate is also an oversight body for those requests resulting in MAiD deaths. The documents reiterated these legal obligations and some added timeframes for reporting. For example, the Alberta documents required physicians to report within 7 days of a MAiD request to the Alberta Health Services Care Coordination Service to advise if the person will be involved in the MAiD assessment/provision or will be referring the patient on. 75 Some regulators mandated (e.g. Northwest Territories, Saskatchewan57,63,64), or encouraged (Yukon 70 ) the use of provincial/territorial forms for reporting.
c. Guidance for the completion of medical certificates of death: The Criminal Code (s. 241.31(3.1)) requires the federal Minister of Health to issue voluntary (non-binding) guidelines for the completion of death certificates. 66 They are non-binding because medical certificates of death fall within the jurisdiction of provinces/territories. The federal guidelines were issued 26 April 2017. 76 Medical certificates of death are regulated by provincial/territorial legislation and there is variation between provinces/territories with respect to reporting manner, underlying, and antecedent causes of death (including MAiD).25,77 Despite this variation, all MAiD deaths are, as noted previously, reported to Health Canada.10,78 The regulatory documents varied in the extent of guidance regarding death certificates. Some did not mention completing the death certificate, 57 some required physicians to follow the federal guidelines, 65 and others explicitly mentioned their distinct provincial/territorial requirements. For example, Ontario noted that physicians must follow joint guidance from the Ministry of Health, Ministry of Government and Consumer Services, and Office of the Chief Coroner which requires physicians to list the disease, illness, or disability leading to the request for MAiD as the cause of death, and must not refer to MAiD or the drugs administered on the death certificate. 59 In contrast, physicians in British Columbia were instructed to include MAiD on the death certificate and provided instructions for how to do this in accordance with provincial legislation. 72
Theme 7: Professional ethics
The Criminal Code does not address professional ethics. In contrast, the AREOLC has guiding principles for end-of-life care including respect for patients, compassion and fairness, and open and transparent communication. Ethical principles are also reflected in the law in other ways. Canada’s Charter of Rights and Freedoms provides constitutional protection for human rights, including life, liberty, and security of the person, freedom of expression, freedom of religion and conscience, and equality. Human rights legislation also exists at the federal and provincial/territorial level and prohibits discrimination on certain protected grounds. In addition to conscientious objection (discussed separately in Theme 1, given its significance), regulators gave additional guidance focused on dealings with patients, conflicts of interest, and interactions with other health professionals.
a. Interacting with patients and family caregivers: When encountering patients seeking MAiD and their caregivers, physicians must demonstrate clear and respectful communication, sensitivity, and support for the patient’s autonomy and dignity. Regulators referenced codes of ethics, for example, “always treat the patient with dignity and respect, according to the Canadian Medical Association Code of Ethics and Professionalism.” 72 Connected to Theme 1, physicians were instructed not to impose their own views or values on the patient.
b. Conflicts of interest: The Criminal Code (s 241.2(5), (5.1), (6)) and the AREOLC (s 26, 29) address conflicts of interest by restricting who can witness a MAiD request and by requiring the MAiD assessors to be independent.66,67 A couple of the documents also addressed other conflicts of interest. The CMQ indicated the Québec Code de déontologie requires physicians to avoid conflicts of interest. 56 The Newfoundland and Labrador document indicated that physicians cannot act as assessors for a family member or any patient which would put the physician in a real or perceived conflict of interest. 68
c. Interacting with other healthcare professionals: The documents discussed mandatory and suggested ethical principles for dealing with other health professionals, such as being “sensitive to the needs and concerns of other members of a patient’s care team.” 75 The documents also discussed the relationship with the pharmacist, related to the Criminal Code requirement that the practitioner who prescribes or obtains a substance for MAiD must inform the pharmacist of that fact before the pharmacist dispenses the substance. 66 Some jurisdictions mandated prompt notification to pharmacists, which reduces delay for the patient and provides the pharmacist with more time to fill the prescription (e.g. Nova Scotia, Prince Edward Island, Yukon).61,65,70
Theme 8: Support for physicians involved in MAiD
Regulators “encouraged,”65,70 or “strongly encouraged”68,75 professional support including support for the emotional challenges of being involved in MAiD.
a. Managing risk: Professional support, particularly legal advice from the Canadian Medical Protective Association (“CMPA”; insurer), or other legal counsel, was encouraged given the evolving nature of MAiD law (e.g. Newfoundland and Labrador 68 ). Other professional supports that the regulators mentioned that could be seen to be related to managing risk included training, education, and professional guidelines, including those from CAMAP, Health Canada, and provincial MAiD teams.57,65,71,73
b. Promoting physician well-being: Acknowledgment of the potential impact on physician well-being varied among documents (some regulators did not mention this). Where this was addressed, it was usually brief. For example, the Newfoundland and Labrador document notes: “Clinicians should be cognizant of their own emotional, physical, and mental well-being. . . . Clinicians may . . . find themselves affected by this process.” 68 In contrast, Québec provided more depth, noting that both the physicians who cared for the person accessing MAiD and the interdisciplinary team may experience grief and need support. 56
The documents suggested resources to support well-being, including those from the CMA, provincial/territorial medical associations, and employee assistance programs. Québec provided additional suggestions, including turning to colleagues, support groups in an institution, team meetings, and an individual consultation with a psychologist or social worker. 56
Discussion
This article provides important insight into the obligations of physicians who encounter patients seeking MAiD. It also showed how different regulators have approached the same federal law (the MAiD framework in the Criminal Code), and how the CMQ in Québec attempted to reconcile the federal law with the AREOLC. As a relatively new framework, legally in force federally since 2016, and a medical practice specifically regulated by the Criminal Code, it is perhaps unsurprising that most medical regulators (like their nursing counterparts) 16 had issued MAiD-specific standards.
MAiD regulation, like other aspects of healthcare, involves a broad range of bodies and actors that steer the system. 2 Provincial and territorial medical regulators are a powerful player in Canada’s MAiD “regulatory space.”51,79 They can investigate and sanction physicians and are an important mediator between the public and the profession. As a result, they can be seen as the “next level down” from the law. They have the potential to provide needed guidance on MAiD to physicians and to bridge some of the federal-provincial/territorial divide. However, this study suggests that the regulators do not occupy this middle space in some key respects. We found that regulatory documents focus primarily on describing (but not defining or offering interpretations of) the MAiD law, largely reflect existing medical practice, and defer to guidance from other regulatory actors such as provincial health departments, Health Canada, and CAMAP.
Professional standards are centred on the MAiD law
A key part of developing MAiD competency is learning to apply the legal framework to clinical practice.16,21 Canada’s MAiD provisions in the Criminal Code are especially difficult for clinicians to grapple with,19,22,80 because they use phrases that are unclear, which generated significant debate from the outset. 81 MAiD assessors and providers must interpret open-ended, ambiguous, and/or unfamiliar terms like, “reasonably foreseeable natural death,” “grievous and irremediable condition,” “advanced state of irreversible decline in capability,” “serious and incurable,” and “mental illness.”19,81 Interpretation and application of the law is an area where clinicians seek clear and consistent guidance,19,22 and is a known challenge in Canada, 19 and in other jurisdictions with AD laws. 21 The regulatory documents provided little guidance on the meaning of these legal terms. As a matter of law, only the courts can provide authoritative interpretations of language used but not defined in legislation, and the regulators’ silence regarding the interpretations of terms found in the Criminal Code must be considered in this context. However, this provides little comfort for physicians as this impasse means it is left to them to navigate the uncertainties of existing law and seek further assistance.19,20,81 Indeed, the documents instructed physicians to consult legal counsel, the CMPA, or guidelines from reputable sources such as CAMAP when facing challenging cases. However, a gap in guidance remains as physicians have reported in other research that they do not find consulting legal counsel or the CMPA to be that helpful for MAiD cases.19,80
Professional standards reflect existing medical practice
The regulators provided some guidance where the law (particularly the Criminal Code) was open-ended or silent. Most of the themes identified involved core aspects of medical practice that are not unique to MAiD: conscientious objection (Theme 1); requisite care, knowledge, and skill (Theme 2); patient-centred care (Theme 3); appropriate documentation (Theme 6); and professional ethics (Theme 7). The lack of many additional rules implies that regulators’ role in the regulatory space is to reinforce these core aspects of existing medical practice and provide an overarching scaffolding for safe practice. Like other areas of medicine, regulators rely on physicians to draw upon their training, experience, and continuing professional development to ensure their practice occurs within the constraints of this scaffolding. The content of the standards demonstrates that regulators have refrained from providing more detailed, practice-near guidance; this has been left to other regulatory actors to provide. Additionally, some regulators may have refrained from issuing standards that add to the content of law out of fear of potential litigation, as occurred when several doctors challenged the College of Physicians and Surgeons of Ontario’s requirement that objecting physicians must provide a patient seeking MAiD with an “effective referral.” 32 While these rationales are understandable, this stance has the potential to create gaps in guidance for physicians when direction from other regulatory actors is unavailable.
Professional standards connect with and defer to other “regulatory actors”
This study supports the view that MAiD regulation in Canada, while centred on twin pillars of the law and professional standards, also reflects “networked governance,” through an interconnected set of actors across organizations. 3 The documents reinforced guidance from Health Canada, provincial/territorial governments, and other professional organizations, including CAMAP. Alignment in guidance from various regulatory actors helps physicians to know what to do, because they receive consistent normative guidance and so do not have to reconcile competing positions. However, when it comes to facing challenging and complex cases, silence from medical regulators leaves physicians to look to other regulatory actors for guidance, such as their provincial/territorial government, local authority, healthcare institution, and professional societies.
Causes of variation in standards
The documents focused on broadly similar topics, yet regulators made distinct policy choices on a range of issues (Table 4). Several factors may account for this variability. As a threshold point, variation in provincial/territorial standards is not unique to MAiD, given Canada’s approach to health professional regulation (which some see as outdated).33,82 Each medical regulator operates independently, 33 with its own local context, policies, and interactions with other key actors in the regulatory space, such as health authorities, and regulators of other health professions. Budget differences may also influence resources that various regulators have available for the development of MAiD-specific standards and guidelines. For example, Ontario, a large province, has nearly 20 times the revenue of the regulator in Newfoundland and Labrador (Table 2). Another factor is regulators’ obligation to consult when changing practice standards, a model that has been criticized as less responsive and flexible than in other countries. 82 Variability may also be a product of the regulators playing distinct roles in MAiD reform and implementation. Québec’s CMQ was deeply involved, actively initiating reflective inquiry into MAiD and taking a lead role in civil society engagement. 13 The AREOLC, being provincial legislation, is not limited to MAiD and covers aspects of end-of-life healthcare that are outside the remit of the Criminal Code. 67 In the rest of Canada, regulators did not catalyse discussions of law reform, and the provinces have not passed comprehensive legislation specifically directed at MAiD or end-of-life care. After Bill C-14 was passed, some provinces’/territories’ regulators took the lead in implementing MAiD, but in others it was the government that initially took on this role. 15 This means that policy choices evolved somewhat differently over time as various regulatory stakeholders in each province/territory implemented MAiD.
Implications of findings for policy and practice
This study highlighted a gap in guidance about the meaning of legal terms in the Criminal Code. It also highlighted interprovincial/territorial variability in MAiD regulatory guidance for physicians.
A key implication of this study is that polycentric regulation can lead to fragmentation. Other studies have demonstrated that this creates uncertainty and is challenging for physicians to navigate.22,31,80,83 Gaps in guidance and variability (whether from the constitutional division of powers or polycentric regulation) leave physicians to try their best to determine who they should be following among a range of regulatory actors, including the federal and provincial/territorial governments, local health authorities, professional organizations, and healthcare institutions. Coupled with the prospect of Criminal Code sanction for failure to comply with the regulatory framework, other research suggests fragmented guidance adds to the stress experienced by physicians and may deter physicians’ participation in MAiD, whether or not they are conscientious objectors.16,22,31
Whose role then is it to provide practitioners with guidance on the meaning of the MAiD law, and what form should it take? The federal government could have done so through defining the key terms in the legislation. It did not do so. The courts could provide an authoritative interpretation, but other than in the AB v. Canada (Attorney General) case (which considered the meaning of “natural death has become reasonably foreseeable” 84 ) they have not been asked to do so and cannot do so on their own initiative. Colleges could provide interpretations in their professional standards. They have, unsurprisingly, declined to do so (they have neither the responsibility nor authority to provide authoritative interpretations).
In 2023, a Model Practice Standard was released by Health Canada, designed to help regulators align their practice and “ensure the protection of the public in . . . complex cases.” 10 Yet, at the time of writing this article the regulators had not adopted this standard wholesale or agreed to harmonize their MAiD standards. Is variation in regulatory documents problematic? On one hand, some argue that inconsistency can be confusing to physicians and the public,11,30 and represents duplicative resource investment. 29 Aspects of the documents may also impact patient access. There are regional differences in MAiD prevalence in Canada, 78 and internationally,85,86 and reasons for these differences are still emerging (Québec is actively exploring the question of why its rates of MAiD are higher than some other provinces/territories. 87 ) Existing research suggests that cultural factors, and factors that facilitate or hinder a patient’s ability to connect to the MAiD system, including regulatory and institutional policies, may play a part in these differences.86,88 For instance, Canadian jurisdictions requiring effective referral connect patients to MAiD services, whereas those with an “information-only” approach risk less access by placing the burden on patients to take positive steps (even when they do not have the information or power to do so). On the other hand, variability in regulatory documents may not necessarily be problematic as it may reflect a jurisdiction’s unique cultural context. Variation is inevitable in healthcare more generally, 91 and other areas of medicine also lack uniform national standards. Variation between jurisdictions can also lead to systems improvements provided regulators are having “regulatory conversations” 89 and are open to observing and learning from each other. 3 This reflects the idea of provinces/territories as “laboratories of democracy,” testing and refining policies (an approach that is also seen in other international jurisdictions, such as Australia) 90 .
Numerous studies have described challenges with implementing MAiD, and how resources for practice have developed over time.19,21,22 In Australia, for example, where both criminal law and health care are regulated at the state level, each state’s voluntary-assisted dying (“VAD”) statute requires VAD assessors and providers to complete mandatory training on the law. 92 Law reform bodies deemed this training necessary because VAD was new and without an established body of practice. 92 Recent education initiatives have been aimed at addressing the gaps in Canada that we identified in this study, but their non-binding nature means that gaps in the regulatory space remain. In 2024, CAMAP launched a comprehensive accredited training program for MAiD assessors and providers, funded by Health Canada. 93 This can help promote shared approaches to practice and help practitioners to feel more confident in their knowledge of the law and its application. However, in constrast to Australia, the training is not mandatory.
Implications for other jurisdictions
Canada’s model of MAiD regulation with its “twin pillars” (law and professional standards) has strengths and weaknesses. The federal law provides national consistency in MAiD eligibility criteria and procedural safeguards. In the provinces and territories, the regulators are potentially a powerful source of additional MAiD regulation. They have a more direct understanding of clinical care than legislators and can shape issues relevant to their local contexts. However, this model gives significant discretion to the regulators in choosing whether to issue a standard and what policy choices to make on discrete issues. Practice-near guidance is left to other actors. This has the potential to result in regulatory fragmentation and practice variability, both of which pose challenges for MAiD practitioners.
The study’s findings can support regulators and policy makers in other countries that are considering legalizing AD or are in the process of implementing it to identify issues to regulate. They may wish to consider what regulatory tools to use to give effect to the topics discussed in this paper, and the implications of these choices. We found that in Canada, there is potential for certain issues relevant to the practice of MAiD – such as the definition of key terms in the law – to fall between cracks in the regulatory space, with no one body being responsible for giving clinicians the guidance they seek. Countries may wish to ensure greater clarity in the terms used in their laws or may wish to identify those regulatory actors responsible for providing guidance on the meaning and interpretation of law. This study surfaces the need to consult with clinicians to ensure that legislative terms and associated guidance is meaningful and understandable to clinicians.
Limitations
This study examined regulatory documents as of 1 September 2023. Some documents may have been revised since. Additionally, this study did not examine practice standards from medical regulators that were not specific to MAiD but might nonetheless influence practice. The study is a document analysis and does not capture the impact, or perceived impact, of these documents in practice, or the context of the policy development. Three of the authors (EC, JD, BW) are currently undertaking a qualitative study exploring key stakeholders’ perceptions of MAiD regulation in practice, which will investigate these issues further.
Conclusion
This study analysed regulatory documents on MAiD for physicians from Canadian regulators. The documents were focused on similar topics, but there was variation in medical regulators’ policy choices. Physicians in each province and territory are therefore subject to differing obligations (in some respects) depending on where they practice, despite the unifying framework of the federal Criminal Code. Ensuring that physicians know and follow the law and practice standards is paramount. While there are some efforts towards harmonization in MAiD standards, such as the Model Practice Standard, the choice to harmonize ultimately remains in the hands of the individual regulators. A better understanding of how this variation in regulatory instruments affects patient access and physician experiences is needed.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251338859 – Supplemental material for Medical assistance in dying in Canada: A review of regulatory practice standards and guidance documents for physicians
Supplemental material, sj-docx-1-pcr-10.1177_26323524251338859 for Medical assistance in dying in Canada: A review of regulatory practice standards and guidance documents for physicians by Eliana Close, Mona Gupta, Jocelyn Downie and Ben P. White in Palliative Care and Social Practice
Footnotes
Acknowledgements
We gratefully acknowledge research assistance from Katie Cain.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Australian Research Council Future Fellowship (project number FT190100410: Enhancing End-of-Life Decision-Making: Optimal Regulation of Voluntary Assisted Dying) funded by the Australian government. The funder only provided funding and did not participate or influence this research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.G. and J.D. were on Working Groups that developed modules for the federal MAiD National Curriculum (funded by Health Canada and developed by the Canadian Association of MAiD Assessors and Providers). M.G. chaired the Canadian Task Group that developed the Model Practice Standard, and J.D. was a member (mandated by Health Canada to develop a model practice standard for the regulation of MAiD by provincial/territorial health professional regulatory bodies). J.D. is on the Advisory Board for the Completed Life Initiative, a national MAiD advocacy and education initiative in the United States. B.P.W. was contracted by the Victorian, Western Australian, and Queensland governments to provide the legislatively mandated training for health practitioners involved in voluntary assisted dying in those states. E.C. was employed on these projects. All views expressed in this article are those of the authors and not the organizations they are affiliated with.
Data availability statement
The regulatory documents used in this study have been cited in the manuscript. Those which are no longer publicly available on regulators’ websites can be obtained from the lead author, on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.