
Abstract
Background:
Medical Assistance in Dying (MAID) was legalized in Canada without a designated period for implementation. Providers did not have access to customary alternatives for training and mentorship during the first 1–3 years after legalization.
Objective:
To report on how doctors prepared for their first provision of MAID in the early period after legalization in Canada.
Design:
Qualitative research design within an interpretive phenomenological theoretical framework. We asked participants to describe their experiences preparing for first MAID provision. Analysis of transcripts elicited themes regarding training and information desired by early adopters for provision of newly legalized MAID.
Participants:
Twenty-one early adopting physician-providers in five Canadian provinces were interviewed.
Results:
Few formal training opportunities were available. Many early-adopting providers learned about the procedure from novel sources using innovative methods. They employed a variety of strategies to meet their needs, including self-training and organizing provider education groups. They acknowledged and reflected on uncertainty and knowledge gained from unexpected experiences and missteps. Key phrases from participants indicated a desire for early training and mentorship.
Limitations:
This study included only the perspective of physicians who were providers of MAID. It does not address the training needs for all health practitioners who receive requests for assisted death nor report the patient/family experience.
Conclusion:
The Canadian experience demonstrates the importance of establishing accessible guidance and training opportunities for providers at the outset of implementation of newly legalized assisted dying.
Keywords
Introduction
Voluntary euthanasia/assisted dying is a high-stakes and often controversial procedure that has been recently legalized in a growing number of jurisdictions in Europe, South America, the Pacific, and North America.1,2 When a new medical procedure is introduced into practice, there is a learning curve for all involved. Modern providers have not been trained in medical euthanasia and assisted dying and they must develop skills in the different components required by local statute. As legalization of euthanasia/assisted dying expands, other jurisdictions can learn from the Canadian experience to improve processes around implementation of newly legalized MAID.
Language describing voluntary euthanasia and assisted dying remains contentious. This paper will use the term Medical Assistance in Dying (abbreviated in Canada as MAID) to encompass both euthanasia (administration of lethal substance by a provider) and assisted death (self-administration of lethal substance made available by a provider). Throughout, the term MAID refers only to voluntary MAID that has legislated criteria for informed consent. Our dataset includes interviews from both Quebec and the rest of Canada. While legislation in Quebec preceded the rest of Canada 3 there was a similarly rapid implementation and the similarities permit use of the broader term, Canada, to refer to both.
Provider training for MAID is now of international interest as many jurisdictions in Europe, the Americas and the Pacific have legalized or decriminalized the practice and more jurisdictions are on a pathway toward legalization. MAID has been previously described by providers as a ‘complex, dynamic process [that] spans from the initial request to the after-care’. 4 Providers must learn the contents of statutes in their jurisdiction and then decipher and apply the law to clinical situations. Terms, such as unbearable suffering, coercion, terminal illness, and foreseeable death must be interpreted and applied. 5 Providers’ professional roles include ‘consulting/supporting patients and/or other staff members with requests, assessing eligibility, administering/dispensing the lethal drugs, providing aftercare to bereaved relatives, and regulatory oversight’. 6 Each of these steps requires specific skills. Voluntariness and informed consent are at stake in the assessment stage. The patient must be provided enough information, must demonstrate capacity to choose, and must not be subject to coercion. Determinations rely on the provider’s proficiency in communicating relevant and personalized information about MAID and alternatives to the procedure. 6 Beyond the assessment stage, the provider must also choreograph the people involved, supporting the patient, family, and healthcare team. Other roles include making nuanced ethical decisions, negotiating documentation, maintaining professionalism and the public trust, managing emotions or conflicts (including with members of the medical team), maintaining their own resiliency, and delivering the procedure. Some of these competencies are common to clinical skills and may already be part of a providers’ scope of practice, while others require specialized, specific training unique to MAID provision. 6
Canada’s rapid route to legalization was followed immediately by clinical provision. This negatively impacted the capability to plan for provider training. MAID was legalized in Canada in mid-2016 via a judicial route that determined that laws prohibiting MAID infringed human rights, the rights to life, liberty and security. 7 The court mandated that the legislature legalize assistance dying in Canada within 12 months. 8 The Canadian legislature had difficulty meeting the deadline and Bill C-17 received Royal Assent in mid-June 2016 with immediate implementation. 9
There was little infrastructure to help providers interpret the legislation and to train or support providers willing to provide MAID to the inaugural cohort. 10 The court and legislature used concepts, such as ‘grievous and irremediable’ that are difficult to apply to specific situations thereby forcing interpretation by the clinician within the consultation. 11 Further complicating matters, roll-out was decentralized and each province was individually responsible for establishing procedures, documentation and reimbursement regimes for its region. To fill the gap in both experience and training lag, early adopting providers started an on-line provider community in 2017 to share experience and provide support. 12 The Canadian Association of MAID Assessors and Providers (CAMAP) has since grown and now reaches providers of MAID throughout Canada. It is an important source of information for providers. 10
The experience of newly legalized MAID in other jurisdictions offers insights into the development and establishment of health professional training and education alongside the implementation of MAID. Oregon legalized assisted suicide in 1997 13 and shortly after, a task force of Oregon providers developed a printed guidebook with recommendations for best practice for the novel procedure. 14 The guidebook was updated with clinical experience in 2008. 15 Vermont legalized MAID in 2013 and reports describe implementation as difficult for Vermont providers, ‘providers lamented the lack of formal education, training and institutional support … seeking out information through informal professional networks and advocacy organizations’ (p. 635). 16 When California legalized MAID in 2015, health policy experts had the opportunity to review prior experiences and an implementation primer became available to providers immediately. Despite this progress, California hospitals and health systems still experienced challenges with newly legalized MAID.17–21 Legalization in Victoria (Australia) came into effect in mid-2019. With an 18-month implementation period, academic literature addressing operationalization and training became available synchronously.22,23 Aotearoa/New Zealand legalized MAID in 2020 and has allowed an implementation period to develop training materials and guidance for providers. 24
Methods
A qualitative design with an interpretive phenomenological framework was employed.25–28 Human research ethics approval was obtained prior to recruitment from the collaborating researchers’ institutions which included the University of Otago, New Zealand and Queen’s University, Canada. An interview guide was developed after review of possible interview structures.25,27,29 This guide featured question zones that progressed from factual to open-ended and emotive with gentle prompts for reflection. This progression of dialog encouraged participants to consider and share their experiences. 30 The interview guide contained open-ended questions about participants’ early experience of providing MAID and included questions about the experience of provision in the initial period after legalization, when training or in-person mentorship was often unavailable. This focus on the initial period potentially diminished any timeline differences between providers from Quebec and providers from other provinces in Canada. The study sought English-speaking Canadian physicians who directly participated in the final procedure of face-to-face MAID provision and were willing to be interviewed for 60–90 min. Exclusion criterion were self-reported current mental health issues that could impact participant safety after discussing a potentially sensitive topic. The recruitment strategy was primarily snowballing and specifically sought to include some providers from rural settings. To inhibit selection bias, the snowballing approach began with individuals from a range of medical backgrounds and a variety of opinions about MAID. These people included two academics at universities, two physician professional group leader(s), and several physicians working in family and palliative medicine. The people who acted as the niduses for the snowballs were sent an e-mail introducing the study and asked to send it to physicians whom they thought would be interested in participating in the study or furthering the recruitment network. This e-mail asked potential participants to contact the lead author (J.P.W.) to express their interest. The recruitment procedure required active initiation from the participants to reduce risk of breaches of confidentiality and potential adverse impact on reputation. While this part of the recruitment strategy protected identity and confidentiality, the requirement to actively reach out to the researcher also likely increased selection bias to participants actively interested in sharing their views or experiences. Informed consent was obtained from all participants prior to scheduling the interview and again at the time of the interview. The informed consent document can be found within our study protocol in the University of Otago Archives at http://hdl.handle.net/10523/12201.
After half of the participants were enrolled, we continued recruitment by adding two new ‘snowball nidus’ contacts. One of these people posted the recruitment letter on the professional group (CAMAP) website asking for doctors practicing in rural areas. It is uncertain how many of the subsequently recruited participants learned of the study from CAMAP.
Interviews, each lasting 65–90 min, were conducted in late 2019. Face-to-face interviews were conducted for all but four participants, who were interviewed via Zoom. Interviews were held in a private place of the participants’ choice and were recorded, reviewed, and transcribed. ATLAS.ti software was used to assist with analysis 31 using an immersion crystallization technique that is well aligned with a phenomenological approach. This is a substantiated approach used to analyse complex and sensitive data. 32 The initial coding was completed by the first author in consultation with the co-authors. The research team also met to compare and review coding strategies and recoded a random sample. Review of the recoded sample was compared with the initial coding to establish concordance.
Twenty-one participants were interviewed out of 26 who enquired about the study. This was determined by first-come-first-scheduled and then logistical constraints. Data saturation was reached at about 18 interviews, but three more participants already had interviews scheduled and these were completed. The primary author completed the interviews with reviews and feedback from one of the co-authors after every few interviews. Additional information on methods and participants is found in other published results from this study. 33
Results
Participants were drawn from a geographically diverse cohort. The 5 eastern provinces of Canada were highly represented with 11 from Ontario, 4 from Newfoundland, 2 each from Nova Scotia and Quebec, and 1 from New Brunswick. Five participants worked in or near large urban centres, 14 worked in small urban to rural settings with regional hospitals nearby and two worked in remote settings. There were slightly more female participants than male. The mean of their reported years in practice was 21 years (range 2–42 years). As previously reported, participant specialties were varied 33 with the majority of physicians reporting that they completed training in Family Medicine. Two physicians had retired and had restarted part-time work with the provision of MAID as their only clinical practice.
Major findings
Participants in this study had a diverse range of experience preparing for first provision of MAID. We report these findings under five headings: (1) reported preparation for first MAID provision, (2) navigating first-time provision without training or guidance, (3) reported reasons participants organized learning groups or formal training course, (4) hindsight reports on individuals’ conceptualization of the ideal preparation for first provision, and (5) participant desire for support and guidance beyond factual knowledge.
Preparation for first MAID provision
Participating physicians’ preparation for MAID ranged from reading a protocol to organizing an accredited conference (Table 1). Most participants reported that the first experience of MAID provision was undertaken without formal or typical types of preparation for first-time provision of a medical procedure. In general, providers who had hospital-based practices or lived in an urban centre were more likely to meet with other providers for formal or informal training, mentorship or support. Rural providers were more likely to rely on on-line resources, including on-line advice and descriptions from others (often via the organization CAMAP). Providers associated with urban or regional centres sometimes formed cooperative groups for self-education or invited expert guest speakers.
Reported preparation for first MAID provision.
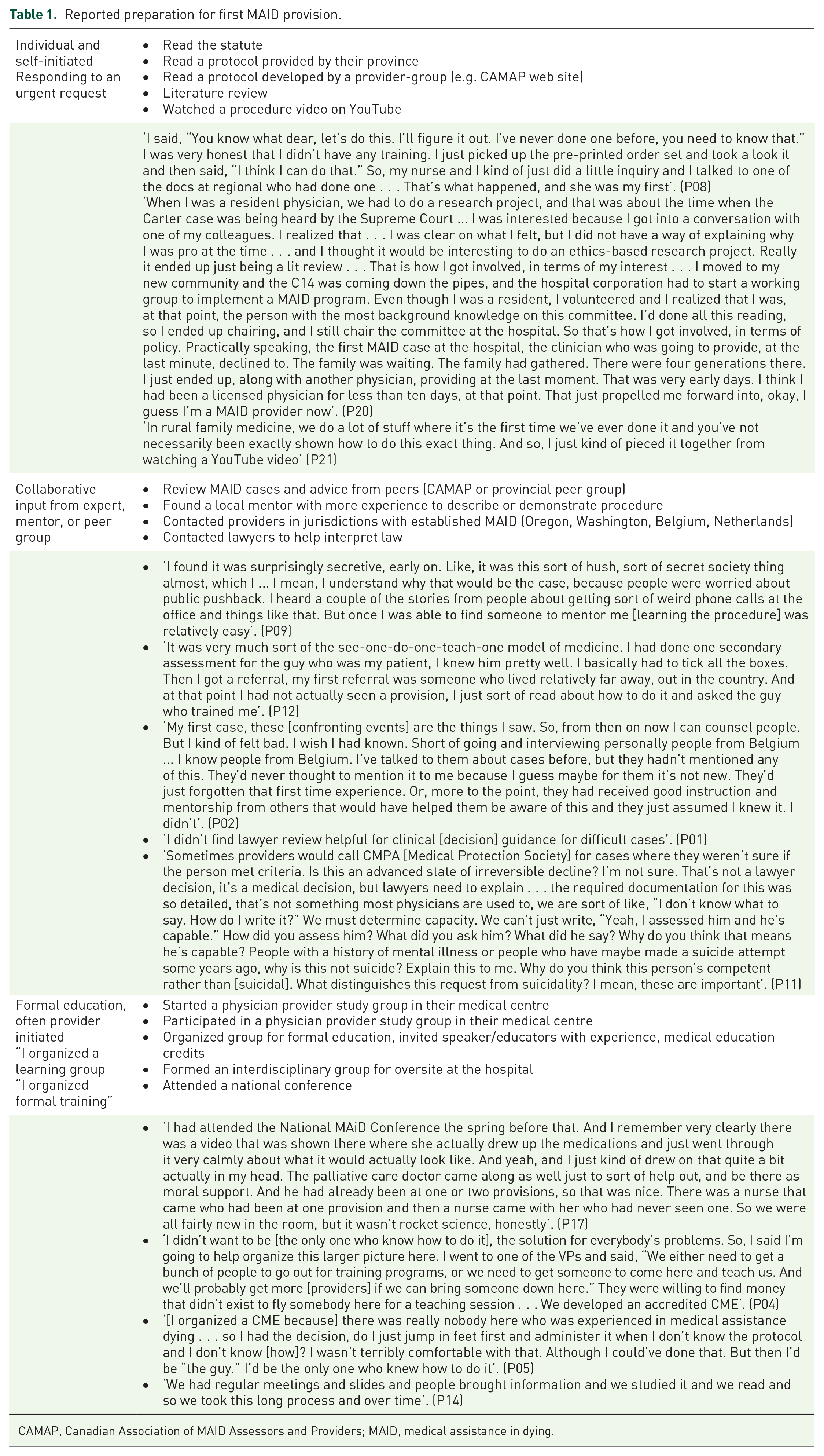
CAMAP, Canadian Association of MAID Assessors and Providers; MAID, medical assistance in dying.
Navigating first-time provision without training or guidance
Several participants described self-directed learning when responding to a request. In these circumstances, there was a perceived urgency to provide MAID prior to training because of a heartfelt request from an individual patient, some of which occurred within days after legalization of MAID. Providers responding to urgent requests made statements such as ‘I figured it out’, and ‘You just do it’. Full versions of these quotes are found in Table 2 alongside other first-hand accounts describing how providers navigated making MAID available to patients prior to formal training. Self-directed preparatory learning and learning from on-the-job experience were both articulated. Participants described gathering information from available resources and figuring out how to merge their own established medical and communication competencies with new specific information about MAID and apply these to their first MAID consultation. Providers described the importance of previously acquired competencies, such as providing informed consent, conveying empathy, and managing patient and family emotions. They also described learning from their own experience for subsequent provisions of MAID. Providers attributed some of the initial non-optimal or ‘negative learning experiences’ to lack of expertise, training, or guidance. We found that rural physicians frequently described individual learning strategies but varied greatly in their expressions of confidence in using existing clinical competencies to inform their adaptations to providing MAID.
Navigating first-time provision without training or guidance.

MAID, medical assistance in dying.
Reasons participants organized learning groups or formal training courses
A small minority of the 21 participants were able to access a formal (accredited) learning programme before first provision of MAID. Two attended a national conference. The learning programmes several others attended were organized by two other participants who were influential in developing formal (accredited) in-person training opportunities. Two additional providers organized informal (unaccredited) face-to-face training sessions utilizing the models of peer groups and journal clubs. Due to the snowballing recruitment strategy, three of the study participants had attended the same regional training.
Participants involved in organizing education described several drivers for investing their energy in organizing group training. They considered this learning style as conducive to multiple goals including gaining clinical competencies, learning from others’ experiences, having peer support and generating fellowship. For some providers, organizing training programmes also extended advocacy and activism by improving accessibility of services. One frequently repeated rationale was that participants did not want to be the only person in their region providing MAID. Sharing knowledge and experiences assisted in increasing the pool of providers, increasing comfort for the procedure, and legitimizing local pathways. Table 1 includes sample quotes describing why providers organized training for themselves and their peers.
Hindsight reports on providers’ conceptualization of the ideal preparation for first provision
Optimal strategies for preparing for first MAID provision were articulated spontaneously by providers, and providers were specifically asked what they would advise for a new provider. A representative quote is from participant 09 (P09) regarding the desire for preparation and support: Have mandatory training for all providers … Make sure that everybody who does MAID or assesses for MAID, has completed a course on how you assess for capacity. Many of us haven’t had that extensive training. You could learn it, but why not just treat it like everything else we do in medicine, teach people how to do it and then they can do it. And have one set of standards, because there’s subtly different tests for capacity. There’s no blood test. But just being able to record your rationale for something, just so that you can defend it, so if anybody comes along saying, ‘I don’t think my dad was capable when he said this’. Okay, well, who’s right? Only one of you can be right, so what’s the deal? Then you just have to be able to answer that for the purpose of the public retaining trust in the system … Have an advisory group [to help providers with] tough cases.
Major subthemes extracted include desiring (1) information, (2) peer guidance, and (3) specific supports including moral permission. The desire for these was most emphatically expressed when providers disclosed errors or non-optimal experiences. Participants’ statements about preparing for first MAID often began with the phrase ‘I wanted’ and went on to describe the themes presented in Table 3.
Conceptualizing the ideal preparation before first provision of MAID.

ICU, intensive care unit; MAID, medical assistance in dying.
Participant desire for support and guidance beyond factual knowledge
A final theme extracted from the data about preparation and training opportunities was that participants desired guidance beyond technical and factual knowledge when approaching first MAID provision. Many reported little continuing difficulty in acquiring knowledge to perform the technical aspect of administration of the lethal agent. Individuals utilized and honed previously acquired communication skills to reassure and counsel patients. The most desired and difficult-to-obtain support was accessing wisdom to ‘hold’ the responses of self and others, and approach navigating the ambiguous legal-ethical decision-making paradigm. Many participants expressed an emotional–interpersonal requirement characterized by the statements ‘I was not ready for that’, ‘I wasn’t expecting that’, ‘I had to give myself consent’, ‘I was scared’, and ‘I wanted a mentor’. Further quotes that articulate and explain their desire for support and guidance beyond factual knowledge are found under support and experiential guidance in Table 3.
Discussion
The vivid accounts and analysis of themes in this research add insight into what it was like to be a provider of MAID during a time when there were few resources for training. The participants’ own words depict what guidance and training was available, accessed and useful. Descriptions of how it felt to be an inexperienced provider can add further insights into what preparation will be most useful to inexperienced providers in the future. While we cannot make claims as to the representativeness of our sample across Canadian providers or transferability of our findings across jurisdictions, we note that our study had strong internal validity within the participant cohort, and external validity is demonstrated by a strong degree of ‘fittingness’ with previous studies.
Published reports document challenges experienced by Canadian providers with newly legalized MAID, such as ambiguous statute requiring interpretation by the clinicians. 34 Recurring problems included lack of protocols or clear guidelines, role ambiguity for team members, and deficiencies in interprofessional collaboration.6,35 Early adopting physicians from British Columbia described a steep learning curve because ‘there were few regulations and no protocols that were immediately in place after MAID was legalized’ (p. e397). 10 Preparation for first MAID provisions on Vancouver Island, BC, included provincial credentialing based on training physicians received outside BC.10,36
The results of our study align with a cross-jurisdiction meta-synthesis of qualitative studies about legal requests for hastened death that reports that policies governing MAID consistently are unclear and require situational interpretation. ‘The legalization of medical assistance in dying in numerous countries over the last 20 years represents a significant shift in practice and scope for many clinicians who have had little-to-no training to prepare them to sensitively respond to patients request for hastened death’. 34 Canadian medical trainees also expressed ‘need for additional training in MAID, specifically around medical-legal issues, communication skills and technical aspects of the MAID process’.37,38 These findings together suggest that early structural preparedness for newly legalized MAID provision is crucial.
Early workforce preparation
There are potential policy implications for the findings, as our results confirm prior reports that implementation before health care staff training resulted in uncertainty and challenges in first provision of MAID.10,35 Urgent demand for MAID was seen immediately after legalization and other jurisdictions should expect some providers to prioritize fulfilling patients’ persuasive requests before fully preparing for first provision. Instigating a training period before implementation is supported by this and previous research. The content, methods, and context of the training will be influenced by specific needs within the jurisdiction. One example of content is described for implementation in the context of New Zealand in 2021. 39 Preparation for providing MAID begins with assisting providers to identify and self-evaluate their ‘scope of practice’ and their individual underlying talents and competencies with the suite of services associated with MAID. Individual competencies identified in the New Zealand context included: counselling and informed consent, interpreting prognostication data, assessing for coercion, determining competency, negotiating contrasting stakeholder views, recognizing ethical dilemmas, supporting families and colleagues, resolving ‘tricky situations’, and self-care (p. 150–151). 39
Clinical education for MAID provision
Participants used a variety of strategies to prepare for first provision and many had only a brief time window. These providers usually engaged in self-education which included reading the law, reading protocols and utilizing resources found on the Internet, particularly those provided by CAMAP. Providers from isolated practice communities were more likely to use self-education methods. One of the key competencies in physician training is to become an accomplished self-directed and lifelong learner. 40 Participants clearly drew on these skills to provide this novel procedure. We postulate that practice setting, previous experience, prior education and personality types all influence comfort with self-education prior to first MAID provision. We confirmed that MAID providers perceived web-based peer knowledge exchange and support to be very helpful. In contrast, providers stated that legal advice from professional organization lawyers were of limited clinical utility. 41
Participants accessing continuing group education expressed that the fellowship of the group process was useful for professionalism and validation. We note that participants who had utilized these groups did not express some of the concerns frequently reported by self-trained physicians. This difference was especially notable around ‘giving themselves permission’ to proceed. Structure and content of the early provider learning groups are likely to be a useful guide to determine content and style of future efforts to prepare providers. The summative list compiled from providers’ statements about what they needed in preparation for first provision is supported by the veterinary literature about the roles of training, continuing education and support for veterinary providers of euthanasia. 42 Participants acknowledged shortcomings and difficulties in first MAID provision and identified what they learned from missteps and experience. Together, these insights provide a roadmap for designing training regimens that will meet the needs of service providers.
Limitations and further study
The usual limitations of qualitative research apply, including selection bias, recall bias and confirmation bias.43–45 Recollections of poignant or potentially controversial past events change with mood and time 46 and are uniquely interpreted and conveyed to the interviewer shaded by coping mechanisms 47 and world-view. This study did not address the training needs for medical staff who are not providers but receive requests to hasten death. We recommend studying needs for both training and support for all health care providers who receive MAID requests. We suggest further research to support or refute the suggestion that widespread palliative care education could improve communication about the role of MAID in end-of-life preferences. 48 Mentorship was frequently desired by participants as a training modality that could assist with aspects of preparing for MAID that are beyond factual knowledge and we are reanalysing our data to elucidate this finding. 49 We suggest researching the role of apprenticeship–mentorship learning, in contrast to self-study or lecture presentations. Finally, further study of preparing for MAID provision should address goals that surpass the provider perspective and encompass the patient experience (by proxy), family engagement, and societal interests.
Conclusion
Optimal clinical care for patients and families is dependent on provider communication, knowledge, decision-making, and problem solving. While MAID is a new paradigm for all stakeholders, including families, medical teams, and society, the inherent uncertainties are amplified for the early-adopting providers. 34 Early-adopting MAID providers in Canada stated preferences for information, guidance, and mentorship. When legalizing medical assistance in dying, jurisdictions should optimize the care experience for patients and families by ensuring time and resources for training, support, and guidance for health care professionals prior to first provision.
Footnotes
Author contribution(s)
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Research ethics approval
(1) University of Otago Human Ethics Committee, Dunedin, New Zealand Reference number: H19/011. Ethics approval to proceed: 11 February 2019. (2) Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board. IRB#: 00001173 Kingston, Ontario, Canada. TRAQ # 6026915 Department Code: FMED-6693-19. Ethics clearance 24 June 2019.