
Abstract
Background:
Older people who die from serious chronic disease typically experience long periods (months or years) of illness and complex fluctuations in their physical health and in their social, psychological and existential well-being. Our understanding of these end-of-life trajectories is very limited, focuses predominantly on physical function and clinical predictors and neglects inter-individual differences. A better understanding of end-of-life trajectories, including what is shared among people and what is individually specific, is needed for an optimal provision of palliative care and health services planning.
Objectives:
TRAJECT is a European Research Council-funded interdisciplinary project with a central aim to gain understanding of what is generalisable and what is individually specific in older people’s end-of-life trajectories and in the circumstances that shape them.
Design:
Convergent mixed-methods design including a quantitative longitudinal survey study, a serial narrative study and a mortality follow-back survey.
Methods and analysis:
TRAJECT applies a novel methodological and analytical framework, examining trajectories through two distinct scientific lenses, both suited for uncovering variability as well as general principles: a structured quantitative approach to capture fluctuations in a standardised way, and an experience-focused qualitative approach to study the subjective stories and meanings behind changes in health. The findings of the quantitative and qualitative methods will be integrated through triangulation and by systematically threading key findings from one method across to the other. The research is conducted in Belgium.
Discussion:
This project will lead to a new understanding of the varied ways in which older people’s end-of-life trajectories unfold and which circumstances and experiences shape them. It will also reveal which elements of trajectories are shared across groups of people and which are individually specific. These new insights will provide a much-needed evidence base concerning groups at risk of poor well-being as they near death, which is needed to optimise palliative care practice, needs assessment, as well as health service planning.
Keywords
Introduction
Dying from chronic illnesses in old age
Advances in medicine and public health have considerably extended human life expectancy and have profoundly changed patterns of death.1 –3 Across world regions, a steadily declining number of people die from infectious diseases and a rapidly growing number die in older age and from serious and progressive chronic diseases such as cancer, heart failure, or neurodegenerative diseases. 1 While we are becoming increasingly better at slowing progression of chronic diseases and extending life, the added years of life are not always spent in good health. Older people make up the largest and most rapidly growing proportion of the worldwide population experiencing serious health-related suffering towards the end of life. 4 By 2060, this will affect 22 million people aged 70 or over worldwide, a 183% increase compared to 2016. 4 Deaths from chronic diseases in older age are typically preceded by extended periods of gradual deterioration in health and well-being, with intermittent fluctuations. Risks to well-being in the older population concern physical symptoms such as pain, but also psychological (e.g. anxiety), social (e.g. social isolation) and existential concerns (e.g. feeling of not being at peace). 5 The progression of chronic disease in older people is more complex than in middle-aged or younger people, because chronic diseases in older age are rarely isolated conditions. Many older people experience comorbidity, that is, a simultaneous presence of multiple chronic illnesses, and additional complicating circumstances for which older age is a risk factor, such as mental health problems and social and financial concerns. The combined adverse effects of these circumstances predispose older people to particularly complex and difficult-to-predict fluctuations, or trajectories, of health and well-being over the final months and years of their lives.6 –8
These end-of-life trajectories remain poorly understood and difficult to predict. We know very little about when fluctuations in health and well-being are most likely to occur, in which patient groups, and which personal, clinical, social and wider societal factors shape them. Illness trajectories towards the end of life have been a subject of palliative care research for around two decades. 9 Commonly, three groups of illness trajectories based on the patient’s main diagnosis are distinguished, that is, cancer, organ failure and frailty/dementia. 9 Most recently, a fourth trajectory, the multimorbidity trajectory, has been proposed. 10 The existing work on end-of-life trajectories has been very influential in advocating for timely palliative care for people with chronic conditions other than cancer and for the need to adapt palliative care services to illness trajectories that differ from ‘typical’ cancer trajectories.9,10 However, these ‘conceptual maps of archetypical patient journeys’10, p. 1 are based on very limited empirical data. A study on trajectories of physical decline in the last year of life did not find typical patterns based on the cause of death. 11 Furthermore, recent data from population-based longitudinal surveys of older people’s last years of life 12 counter existing notions of declining social trajectories towards the end of life. 10 This emerging evidence suggests that we still have an insufficient understanding of fluctuations in health and well-being as death approaches and of periods and patient groups that are most at risk of burdensome trajectories.
It is essential that we overcome this scientific gap as it has fundamental consequences for advances on multiple research frontiers as well as clinical developments in end-of-life care that build on knowledge of end-of-life trajectories.6,13,14 Poor understanding of end-of-life trajectories complicates person-centred care by hindering recognition of periods and groups most at risk of adverse trajectories. This hinders anticipatory management of symptoms and concerns, and advance care planning. Understanding the course and causes of change in end-of-life trajectories provides opportunities to influence these trajectories towards reduced suffering, which is what good care, including palliative care, ultimately aims to achieve. Finally, a better knowledge of end-of-life trajectories is also critical for setting priorities and deploying resources in health policy (i.e. when is health and well-being most compromised and in which groups) and for developing prevention and intervention programmes for our ageing societies.
The difficulty of understanding end-of-life trajectories
End-of-life trajectories have been conceptualised and operationalised differently with no consistently applied definition. However, they can be seen as falling under the overarching term of ‘health trajectories’. A health trajectory has been defined as ‘a pattern of health over time’ or as ‘the dynamic (changing) course of health and illness’.6, p. S5–S6 The Minnesota Center for Health Trajectory Research describes health over time as resulting ‘from multiple factors operating in nested genetic, biological, behavioural, social, cultural, environmental, political and economic contexts that change as a person develops’.6, p. S5
There are two major reasons why our understanding of the multidimensional end-of-life trajectories of older people is still limited. The first is the very small amount of prospective longitudinal data on changes in health and well-being as people near death. Next to general feasibility challenges in end-of-life research, 15 repeated assessments in the context of illness fluctuations and disability pose risks to recruitment and retention of research participants and to data quality (e.g. missing data).15,16 Longitudinal research is also highly resource-intensive and requires considerable research budgets and longer project runtimes. As a result, most observational studies on the end of life are cross-sectional in nature and include, for example, retrospective mortality follow-back surveys (conducted after death and hence relying on proxies rather than first-person accounts), studies of death certificate data and cross-sectional surveys that cannot capture changes within individuals’ health and well-being over time.14,17 However, despite the methodological and practical difficulties that come with longitudinal research on the end of life, our research field has provided important insights into changes in health and well-being as people near death, for instance of people with renal failure, 18 or physical disability.11,13,19 –25
The second reason for our field’s limited understanding of end-of-life trajectories is that we have predominantly studied average trajectories of specific groups, for instance defined by underlying illness 13 or social connection, 19 and generalised these aggregated temporal patterns across individuals. However, it is becoming increasingly clear that in their search for general, unifying principles concerning end-of-life trajectories, these approaches mask important inter-individual variation and run the risk of drawing inaccurate conclusions about individuals based on aggregated trajectories.18,26 A study of trajectories of symptoms and wider health-related concerns over the last year of life of people with conservatively managed stage 5 chronic kidney disease showed that average patterns of increasing symptoms and concerns masked considerable individual variation, including relatively stable and fluctuant patterns of symptom distress, alongside steadily increasing ones. 18 Not only quantitative, but also qualitative research has followed this generalising principle, aiming primarily to generate common themes among the illness trajectories observed across groups of individuals and to define ‘typical’ trajectories.21,27 That said, letting go of generalisation and seeking purely idiographic information on individual people cannot advance our scientific understanding and clinical developments. A certain level of ‘general validity’ and transferability of findings is needed to constitute an important contribution to science and to inform coordinated efforts to advance patient care. The big hurdle we therefore face is the absence of an integrated understanding of commonalities and individual differences in older people’s end-of-life trajectories and in the circumstances that shape them. We do not know where we can draw generalisable conclusions about end-of-life trajectories without sacrificing or masking crucial variation.
Aims and objectives of the TRAJECT project
The European Research Council (ERC)-funded project ‘Uncovering commonalities and differences: Towards a novel framework for identifying end-of-life trajectories of older people with serious chronic illness’ (acronym: TRAJECT) aims to apply a novel analytical and methodological framework to identify generalisable and individually specific aspects of older people’s end-of-life trajectories and the circumstances that shape them. This overarching aim is addressed through three specific objectives:
Concerning the term ‘end of life’: There is no agreed-on temporal delineation of the ‘end of life’ in the literature. In the TRAJECT project, it is broadly seen as the last year of life, thus extending beyond the terminal phase, but still limited to a period when death is part of a person’s near future. However, predicting when a person will die is very difficult. 28 It is not possible in prospective studies on the end of life to define a uniform period prior to death. 17 Hence, some participants may live shorter or longer after inclusion.
Methods
Study design
TRAJECT studies end-of-life trajectories through a convergent mixed-methods design, combining: (1) a quantitative longitudinal study of health and well-being of older people with serious chronic illness who are nearing the end of life with (2) a serial narrative interview study with a purposively selected sub-sample of these older people and (3) a mortality follow-back survey with proxy respondents (typically a family member or other close person of the deceased older person) concerning the last 3 months of life. The goal of mixed-methods research is to obtain qualitative and quantitative complementary data on the same topic and thus a more complete and complex understanding of a phenomenon. 29 The convergent mixed-methods design indicates that the quantitative and qualitative methods are applied simultaneously (i.e. in the same research phase), receive equal priority and equal ‘weight’, ask different types of questions but are orientated towards a common research aim and are integrated at the analysis and interpretation stage. 30
Methodological approach
To uncover the unifying elements and commonalities in end-of-life trajectories across individuals, this multidisciplinary project draws theoretically and methodologically from different disciplines including psychology, anthropology and health sciences. It aims to integrate positivist and constructivist research paradigms by bringing together quantitative and qualitative research methods. The quantitative methods assess physical, social, psychological and existential well-being using structured and validated measures, while the qualitative, experience-focused methods aim to capture older people’s engagement with the subjective process(es) of meaning-making in the context of changing health.
Quantitative longitudinal research designs, known from epidemiology, are essential for studying changes in health over time (i.e. within individuals) as well as variation between individuals. Structured, standardised measures that have been validated in large samples allow us to obtain data that are comparable across individuals as well as over time within the same person. In this way, changes over time in well-being and the factors that are associated with these changes can be quantified and visualised. Furthermore, quantitative data obtained in larger samples and the statistical methods with which they are analysed allow researchers to determine shared characteristics (i.e. similar trajectories or strong predictors of specific changes in health and well-being) as well as important variation.
However, when used in isolation, the quantitative methods of assessment fail to capture the complexities inherent in understanding end-of-life trajectories in their entirety.31,32 In conjunction with the quantitative methods, qualitative methods can help researchers additionally study layers of personal and collective meanings that otherwise go undiscovered.17,33 Yet, this perspective is crucial for a full understanding of commonalities and diversity in end-of-life trajectories. Understanding scientifically the personal meanings and individual processes (e.g. perceptions, emotions, thoughts and behaviours) through which people navigate changes in health34 –37 can help us uncover complex interplays of medical, social, psychological and societal influences on health and well-being that quantitative epidemiological research alone does not reveal.32,38 –41
The qualitative research method used in TRAJECT is the narrative method. Trajectories of health and well-being are first and foremost individual experiences or stories that hold similarities and differences among people. When people are asked to describe disruptive life events, such as the course of a chronic illness, many respond with stories or narratives. 42 Stories or narratives, which are influenced by an understanding of self and affect the ‘self’ in turn, 43 are powerful in the ways they bring forth the embedded polycontextuality in the understanding of trajectories. They can reveal how the construction of one’s subjective reality is affected over time by their illness(es) and how the illness experience shapes people’s experiences of self and identity. 44 Rather than a chronological ordering of facts, or a medical history, personal narratives of illness trajectories are reconstructions of how people experience, understand and interpret their past, present and even future health. 38
The quantitative and qualitative methods will be combined in a convergent mixed-methods design that follows a ‘pragmatic’ approach, signifying the complementarity of the methods based on different ontologies and epistemologies to produce shared meaning of the phenomenon.45,46 The methods are thus interdependent while retaining their paradigmatic modalities and perspectives, balancing the perspective of the researcher and the researched.31,32 Each of the two methods will serve to identify commonalities and differences in trajectories, each through its unique scientific perspective.
Relationship between objectives, work packages and methods
The research will be conducted in four work packages (WPs1–4). Each method, quantitative and qualitative, will first be analysed separately within its methodological parameters to address Objectives 1 (WPs1 and 3) and 2 (WP2), respectively. WP4 will then integrate the mixed-methods data of WPs1–3 in a synergistic way to address Objective 3. The interconnections between the study objectives, methods and work packages over the course of the project are visualised in Figure 1.
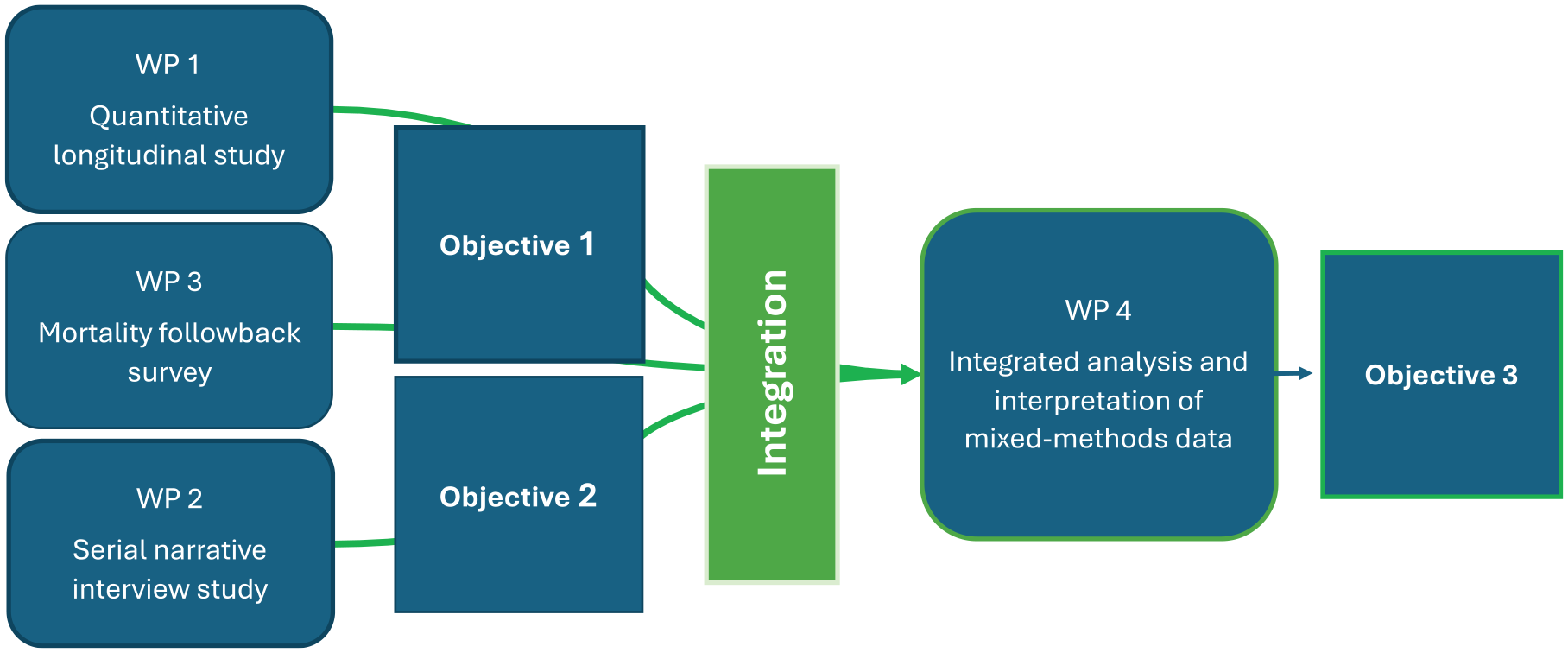
Relationships between objectives, methods and work packages over the project course.
The study designs used in the four WPs are:
Setting: The Belgian context
The TRAJECT project will include participants from two university hospitals in Brussels and Flanders, two regions in Belgium. Although relatively small in surface, Belgium is the third most densely populated country in Europe. 47 It is one of many countries worldwide with steep projected increases in life expectancy over the coming decades. 3 Belgium has a very prevalent system of healthcare and healthcare financing in Europe, but also outside Europe. It has universal health coverage, with compulsory health insurance financed through social security and taxation, that covers the full continuum of essential health services. Healthcare is delivered by a mixed public and private system of independent medical practitioners and public, university and semi-private hospitals. Belgium scores relatively highly in international comparisons of the development of palliative care systems, 48 and palliative and end-of-life care are represented in the Flemish policy agenda concerning healthcare for older people. 49 It is also one of several countries or states worldwide where assisted dying under specific conditions has been legalised. Belgium is a federal constitutional monarchy with a parliamentary system and is divided into three autonomous regions: Brussels-Capital Region, Flanders and Wallonia. It has two major linguistic communities, the Flemish community (around 60% of the population) and the French-speaking community (around 40%). This project will be conducted in both linguistic communities.
Population
The population studied by the TRAJECT project are older people (i.e. aged 70 or over) who are diagnosed with a serious chronic illness and who are judged by their physician as being in deteriorating health, based on pre-specified criteria (see section on eligibility criteria below). While the OECD definition for ‘older persons’ is 65 and over, linked to retirement age, 50 this project takes a higher threshold age as it aims to study those at risk of comorbidity and complex health fluctuations. 51 We have decided against a prognostic criterion (e.g. expected survival) for identifying older people who are nearing the end of life because such estimates have low predictive validity, with a tendency towards overestimating survival time.28,52 Instead, to include older people nearing the end of life, we apply disease-specific criteria to identify older people who are in deteriorating health linked to the chronic illness with which they have been diagnosed.
Eligibility criteria and identification of participants
This project applies general inclusion criteria, applicable to all participants as well as disease-specific inclusion criteria to identify those patients who are in deteriorating health.
The general inclusion criteria are:
- patient is 70 years old or over,
- diagnosed with a serious chronic condition (this also includes frailty or the co-existence of multiple pathologies which might not be considered serious chronic conditions each on their own but, in combination, may cause death),
- able to participate in data collection in Dutch or French.
The disease-specific inclusion criteria for deteriorating health (Table 1) are applied according to the medical specialty (hospital department) that identifies the patient and are judged by the patient’s treating hospital physician.
Inclusion criteria indicating deteriorating health. a

The inclusion criteria presented in this table are currently under development and subject to refinement through ongoing consultations with clinicians and a pilot study, prior to the main study. Criteria for additional chronic conditions may be added. They are based on empirical studies of prognostic indicators combined with outcomes of consultations with physicians during the preparation of the TRAJECT project.
The general exclusion criteria are:
- patient is not able to give informed consent or participate in data collection due to cognitive impairment, based on physician judgement or researcher’s assessment during informed consent procedure,
- patient is in the terminal phase of their trajectory, defined as last days of life, based on physician judgement.
No criteria are formulated for neurodegenerative diseases where neurocognitive impairment is the main feature (e.g. Alzheimer’s disease) according to ICD-11 criteria, because people who are nearing the end of life as a result of one of these diseases would not be cognitively able to participate in this study. We acknowledge that the criterion of cognitive capacity, which effectively excludes people who are dying from dementia, presents a limitation. However, they may be included in the study if they fulfil the inclusion criterion of deterioration in another chronic condition (e.g. a patient with advanced cancer and comorbid, but not advanced, dementia).
Potential participants will be identified from two university hospitals in Brussels and Flanders from the following departments, where older people with serious chronic illnesses are cared for: geriatrics, oncology, pneumology, cardiology, gastro-enterology (hepatology), nephrology, neurology and haematology. The geriatric departments also coordinate geriatric liaison teams, who provide and coordinate care for older people across different hospital departments. Recruitment is not stratified per specialty, but we will aim to include patients across these recruitment sites with a view to obtaining a diverse sample regarding pathology, age, gender and other sociodemographic characteristics.
To include people in deteriorating health into research, close collaboration with local clinical settings is crucial. Most older people with a serious chronic illness in Belgium who are in unstable or deteriorating health undergo hospitalisation at some point in the last phase of life, which makes hospitals an appropriate setting to identify this group in the Belgian healthcare context. 24 Depending on the progress of recruitment and characteristics of recruited patients, we may include additional hospitals and departments at a later point. We considered recruitment through general practice, but this approach would have been unfeasible because Belgian GP practices are rather small, with on average four patients per practice who die per year, 54 and many practices would have had to be included to achieve the required sample size for this study (see work package descriptions for information on sample sizes).
Work Packages
WP1: Quantitative longitudinal study
To address Objective 1, we will conduct a quantitative longitudinal observational study with measurements at baseline, and every 2 months over a period of 12 months or until death if the participant dies before. Participants who live longer than 12 months after inclusion will be retained in all analyses as the data they provided still concern a period of deteriorating health that can be, broadly, considered as the ‘end of life’, even if death itself does not fall within the study period. We will include 280 participants, accounting for attrition due to participants dying but also for reasons other than death.
The focus of this WP is to measure well-being specific to the four domains of palliative care, that is, the physical, social, psychological and existential domains. The research team has selected different constructs to represent these domains based on two main sources: first, the constructs covered by the most important validated instruments assessing quality of life/well-being among people nearing the end of life/receiving palliative care,55,56 and secondly qualitative research specifically among older people in deteriorating health about their palliative care needs and what is important to them as they near the end of life.57,58 After conferring with the research team, the following constructs were assigned to the four palliative care domains:
- physical: pain and other symptoms, functional status;
- psychological: depression, anxiety/worries, sadness; self-reported cognitive functioning
- social: social connectedness, loneliness, family support, trust in carers;
- spiritual/existential: having meaning and purpose, autonomy/sense of control, feeling good about oneself, religiosity.
Additionally, prompted by qualitative research evidence, we will include, as independent variables, constructs related to individuals’ perceptions of their care as well as practical, informational and environmental needs. Further independent variables cover sociodemographic and clinical characteristics and living situation/social environment. Data collection will be done with structured questionnaires. Next to strong psychometric criteria (reliability, validity in older populations), the measures were selected based on availability of short forms (to reduce burden) and suitability for use in structured interview formats. The questionnaires will be administered in face-to-face structured interviews as many older people who are nearing the end of life find it difficult to complete self-report questionnaires on their own, judging from this team’s previous research involving older people in poor health. 59
Regarding data analysis, spaghetti plots will help visualise the trajectories of the outcome variables over time. Distinct groups of trajectories will then be identified by conducting latent class growth models (LCGMs). We will assess associations between participants’ characteristics (personal, clinical and social) and the different groups of trajectories. The individual trajectories that cannot be classified into a specific group and the characteristics of these respective participants will be described. Next to LCGM, linear mixed models will be used to compare trajectories between predefined groups (based on the independent variables assessed). Both types of longitudinal analyses will be conducted twice with different measures of time as independent variable: either age or time before death (the latter will only include participants who died during the study period).
WP2: Serial narrative interview study
To address Objective 2, we will conduct a serial narrative interview study in parallel with the quantitative longitudinal study in WP1. The narrative study will include 36 older people, a sub-sample of the 280 WP1 participants, again accounting for attrition due to death or other reasons. Overlap of participants among WP1 and WP2 will allow individual-level triangulation of the mixed-methods data in WP4, next to triangulation on an aggregated level of analysis. Interviewing is a very common method in narrative research. Narrative interviews will be conducted at baseline (corresponding to the baseline of the quantitative longitudinal study) and every 2 months over 12 months or until death, if the participant dies before. Serial narrative interviews were feasible in a sample of older people who were living and dying with frailty. 60 The narrative interview method is exceptionally well suited to get a patient’s illness perspective with a focus on the subjective construal of bodily occurrences. 61
The narrative interviews will be guided by a semi-structured conversation guide. Inspired by an example given by Anderson and Kirkpatrick, 62 the first interview with each participant will commence with the following question: ‘Could you tell me about when you first got sick, and what has happened since?’. This broad, open-ended question is meant to encourage the participants to tell a story, allowing them to shape it based on their own exploration of their illness experience and its impact on their life. The answer to this question will form the main narrative part of the interview, during which the researcher interrupts the participant as little as possible and only provides non-verbal encouragement. In subsequent narrative interviews with the same participant, the first question will be a similar open-ended question probing for storytelling. Other than the initial question, the conversation guide consists of a list of open-ended questions serving as examples for the interviewer. While narrative interviews are by definition quite unstructured, 63 the conversation guide serves to create a guideline and to remind the researcher of potentially relevant topics to cover. Except for the first question, all questions in the guide are suggestions, and the researcher is encouraged to let the interview unfold based on the narrative that the participant creates. Most important in the conduction of narrative interviews is the capacity of the researcher to relinquish control over the conversation and let the participant lead the conversation to potentially unexpected topics.42,62
Seen through a scientific lens, narratives, like all stories, consist of content, structure and performance. Narrative analysis seeks to determine these aspects of narratives, and it does so by preserving longer stretches of the story, set in the context in which it was generated and told. 39 This distinguishes it from thematic analysis, where individual accounts are fragmented into discrete categories for coding. We will apply Riessman’s combined approach to analysing content, structure and performance aspects of narratives. 42 It involves determining content (what was said, i.e. themes or topics of the narrative and setting of the story), structure (how was the story told and organised, e.g. identifying introduction, problem, climax, resolution, characters as well as gaps and inconsistencies, or sequences of events) and the performance aspect (to whom was the story told, including the relationship between narrator and listener and differences in their social positions). After each narrative has been analysed separately, the longitudinal series of narratives of each participant will be analysed to identify any changing or recurring content and structures over time, and any underlying narrative threads. As the final step, we will identify commonalities and diversity among participants’ narratives over time.
WP3: Mortality follow-back proxy survey
If a participant dies, either during the 12-month follow-up period or if the research team is informed of their death after they have completed the 12-month study period, we will invite a proxy respondent (i.e. family carer or another close person) to complete an after-death (mortality follow-back) survey covering the deceased’s last 3 months of life. The proxy will be identified based on the contact person indicated by the older person upon their inclusion in the study.
Retrospective surveys with family carers or healthcare providers of deceased people are a widely used method to study people’s last phase of life, as they allow the identification of a uniform period at the end of life across participants (e.g. last 3 months of life), which is not possible in prospective studies.24,64 It is common practice in these studies to invite bereaved family carers to participate at least 3 months after their bereavement, and this was found to be acceptable by participants.65 –67
The main purpose of the mortality follow-back survey is to obtain information on the terminal phase of older person’s life and circumstances of their dying and death, and to enable us to examine how trajectories of the last year of life relate to experiences in the terminal phase. The proxy survey is a structured quantitative measure, largely using items from existing mortality follow-back surveys with family caregivers. It will be conducted in a structured interview format at a location of the respondent’s preference or via telephone. Additionally, the survey will include a narrative prompt with the aim to elicit a short narrative from the proxy respondent about the older person’s last phase of life. This open question is meant to be broad enough to initiate a story, but not so broad that it goes beyond the scope of the after-death interview, that is, the end-of-life trajectory of the older person with chronic illness. Proxy respondents will be included if they were identified by the WP1 and/or WP2 participant as their contact person, if they are able to consent to participation, and if they are able to participate in data collection in Dutch or French. There are no exclusion criteria.
Analysis of the quantitative WP3 data will involve frequencies, and linear and logistic regression model analyses to examine associations between variables while controlling for covariates. Regression analyses will also be applied for joint analyses across the quantitative data of WP1 and WP3 (e.g. where data reported by the older person in WP1 are used to predict end-of-life outcomes reported by the proxy). The analysis of the qualitative narrative will follow the same principle as the narrative analysis in WP2, including the possibility of a cross-cutting analysis of narratives of WP2 and WP3.
WP4: Integrated analysis and interpretation of mixed-methods data
This WP will synthesise the findings of WPs 1 through 3 through a convergent design, involving analysis and interpretation that cut across the different methods. In doing so, this WP will generate insights that go beyond the separate findings of the methods applied in WPs 1 through 3. It is important to note that the quantitative and qualitative methods to be integrated do not serve to ‘validate’ one another. No method reveals an absolute ‘truth’, but they shed light on the same social reality through different scientific lenses. The integrated analysis will follow rigorous methods, according to established guidance for mixed-methods research.30,68,69 It contains two components:
(1) Triangulation of quantitative data on trajectories of health and well-being (WP1 and WP3) with narratives (WP2 and narrative prompt in WP3): For those individuals that provided quantitative and narrative data, the team will create a mixed-methods matrix on the level of the individual, displaying related findings from the different methods side-by-side to identify patterns within and across cases. Next, we will develop a triangulation protocol to integrate findings based on the whole of both datasets, that is, looking at overall findings obtained in WPs 1 and 3 on the one hand and WP2 on the other hand, rather than data of individual cases. It will involve displaying and appraising findings of the quantitative and qualitative methods side-by-side, organising them visually as well as through tables and considering the relationships between the findings. This process will identify inter-method agreement, partial agreement, complementarity, discrepancy or silence (i.e. theme arises in one method but not another). For instance, we will analyse what is shared and what are differences in the narratives of people with similar and different quantitative trajectories. We will also study in-depth the illness narratives of people whose quantitative trajectories could not be grouped with others in WP1. We will look for reasons that can explain inconsistencies in both datasets. The research team will then create a narrative synthesis based on these analyses.
(2) Following-a-thread method69,70: Starting from the initial analysis of each separate method, we will identify key findings that require further exploration. We will then follow each of these findings from one method across to the other component (following a thread). This will create a multi-faceted picture of the phenomenon. This is a focused iterative approach that interweaves the findings that emerge from each dataset. It will help gain a deeper understanding, for instance, of the multiple factors and circumstances that interact with and/or shape end-of-life trajectories. This integration method preserves the nature of the open, exploratory qualitative inquiry while combining it with the focus and specificity of the quantitative data.
Ethics
The TRAJECT project has received ethics approval from the Commission for Medical Ethics of UZ Brussel (Brussels University Hospital, 1432024000122, approved on 03.07.2024) and the Commission for Medical Ethics of UZ Gent (Ghent University Hospital, B6702024000297, approved on 02.09. 2024). The project will be conducted in accordance with all applicable legislation and regulations, including the Declaration of Helsinki, International Guidelines for Ethical Review of Epidemiological Studies (1991), International Ethical Guidelines for Biomedical Research Involving Human Subjects (2002) and EU General Data Protection Regulation 2016/679 (GDPR).
In our research, we are committed to minimising patient burden by closely monitoring participants’ physical and emotional distress, and offering the option to stop, reschedule, or shorten the interview. For participants involved in both work packages, the structured survey and the narrative interview will be conducted on different days to limit burden.
Prior to the main study, we will conduct a pilot study, involving 10 patients over a 2-month period, that will play a critical role in evaluating the feasibility and acceptability of the proposed data collection strategies, including the scheduled follow-up intervals. Data collectors will closely monitor and document patient experiences throughout the study, paying particular attention to the ease of participation, the effectiveness of follow-up frequency, and any challenges encountered during data collection. Based on these insights, adjustments will be made to improve the overall process and ensure a more efficient approach that minimises burden to participants.
In case any participant experiences psychological distress from discussing their health or illness, the researchers will follow a previously established distress protocol. This includes reminding participants of their right to skip questions or withdraw from the study at any time without consequences and can also involve directing participants to appropriate professional help, if needed. The research protocol includes several measures to minimise distress, such as providing clear information about the study beforehand, allowing participants to control the depth of the conversation and offering a post-interview debriefing for additional support.
Managing a large-scale, interdisciplinary mixed-methods research project
The TRAJECT project, being interdisciplinary in nature and involving multiple methodologies and methods and researchers with different scientific backgrounds, relies on productive collaboration and a well-attuned plan for its successful completion. We outline here the principles based on which the project is being conducted and managed with the aim to achieve the project aims in the foreseen time. The core project team consists of the principal investigator (L.P.), two senior researchers with complementary scientific expertise (K.T., L.V.dB) and two doctoral researchers (E.G., C.V.dB). They collaborate with clinicians from diverse medical and nursing specialties and with research assistants who help with data collection. The TRAJECT project is also followed by an external Advisory Board (members are named in the Acknowledgement section), who meet the project team twice a year to discuss key aspects of the research methods and findings and the project’s progress.
The main principles for managing and progressing the project include:
Regular and frequent exchange among core project team members to effectively manage the project and track its progress, achieve coordination and integration in research activities, enable collaborative problem solving that leads to innovative solutions, and share knowledge and foster a deeper understanding of the project’s broader implications across scientific disciplines
Collective decision-making on key scientific, procedural and management issues
Fostering trust among the project team and a sense of responsibility for the project’s success among all team members
Ensuring input of clinical expertise from medical and nursing specialties relevant to the population under study
Ensuring input from the external Advisory Board which helps the project team take a bird’s eye view of the different aspects of the project and recognise the need for re-engagement, modification or further development
Paying attention to researchers’ well-being as they conduct research with a vulnerable population and on a sensitive research topic
Effective mentoring of PhD students, skill development and progress monitoring in the context of their PhD trajectories
Discussion
Conceptual and theoretical contributions
The key contribution of the TRAJECT project will be a new understanding of how older people’s end-of-life trajectories unfold. The project will bring forth the diversity in trajectories stemming from wide-ranging circumstances and experiences that shape them. This work will also reveal which aspects of end-of-life trajectories are shared and where we need to pay particular attention to inter-individual differences.
End-of-life trajectories do not just ‘happen’ to people. Humans also play a pivotal role in (re)shaping their changing health and hence the trajectories of their well-being as they near death. This project contributes a fundamentally new approach to the scholarship on end-of-life trajectories, which have so far mostly been explored as being shaped by one’s diagnosis or cause of death. 13 We look at a wider range of circumstances that can shape trajectories, as well as their interactions, including not only the observable ones, such as clinical or sociodemographic characteristics or social support, but also the meanings that people attribute to their changes in health and the processes through which they navigate them. In doing so, TRAJECT aims to enhance the understanding of what is common or generalisable in end-of-life trajectories and where the limits of generalisation lie. It looks beyond the generalising principle to include also the individually specific, thus encouraging us to re-think how we examine, understand and categorise end-of-life trajectories.
Currently available evidence suggests that there are no universal end-of-life trajectories. 11 Generalisation based on defined patient or clinical characteristics is an effective way to draw attention to the fact that there are different courses of illness towards the end of life and that health and social care need to be able to respond to different needs. However, an exclusive focus on aggregated trajectories risks that we draw inaccurate conclusions about individual people. In isolation, aggregated trajectories are not suited to guide reflection about current and future fluctuations in older people’s health, the circumstances and periods that put them at risk of deterioration in well-being and possible interventions to support them. To gather a more complete understanding of end-of-life trajectories, there is a need to create a safe separation from the ‘general’ in trajectories to bring forth the ‘atypical’, that is, the inter-individual differences and specificities in how these trajectories are shaped by diverse circumstances in a person’s life. This necessitates looking beyond the clinical factors and towards those that encapsulate the ‘human’ and their experiences with their illness(es). At the same time, a scientific examination of end-of-life trajectories that can inform palliative care practice and other clinical developments also needs to be able to draw generalisable and transferable conclusions across individuals. This project seeks to unite these two aims, finding unifying elements in older people’s end-of-life trajectories while also showing where the limits of generalisation lie.
To achieve this, our research will generate ‘researcher-constructed’ (quantitative, structured) trajectories of well-being alongside participant-constructed narratives of their health and illness, through different methodologies that both allow the examination of the shared and the individually specific. These methodologies, a structured quantitative approach to measuring well-being and its predictors longitudinally and a constructivist approach to studying serial narratives of health and illness, are located on what are usually considered opposing ends of ‘axes of inquiry, from which research operates’71, p. 43 (i.e. inductive-to-deductive, subjective-to-objective, idiographic-to-nomothetic, high to low reflexivity). Our project will show that the integration of such diverse epistemologies is not only feasible, but that it leads to scientific breakthroughs that each of the approaches could not achieve in isolation.
A final conceptual and theoretical contribution of the TRAJECT project is inquiry into and a new framing of what end-of-life trajectories, and, by extension, health trajectories are. The scholarship on ‘trajectories’ is varied, and end-of-life research literature has mentions of multiple trajectories pertaining to the end-of-life aspects, for example, dying trajectories, care trajectories, cost trajectories and trajectories of symptoms at the end of life.72 –75 An illness trajectory deconstructs the experience of illness as ‘longitudinal with recognisable phases’.73, p. 2 Weiner and Dodd (1993) differentiated between the course of illness and illness trajectories. 76 Illness trajectories along with the physical aspects of the disease also include ‘the total organisation of work done over the course of disease’76, p. 20 affecting all those involved, the patients, health professionals as well as the family. Trajectories abide by and derive their meanings through the notion of time. The different ways in which end-of-life trajectories have been understood and interpreted are a testament to their convoluted yet comprehensive nature. They are convoluted, as there is no single universal trajectory defining the end of life, and comprehensive because anything in temporal continuity could be made sense of as a trajectory. Rather than attempt to simplify or find one specific definition of the concept of end-of-life trajectory, our project will bring forth and highlight their inherent complexities and nuances by applying the notion of time as both objective and subjective; through an exploration of changes in health and well-being over time as understood by both researchers and research participants.
Methodological contributions
There is a dearth of large-scale prospective research in populations nearing the end of life, and much of research on the end of life (e.g. last 3 months of life) is retrospective, meaning that proxies are invited to report about a deceased person’s experiences in their last days, weeks or months of life. 17 The advantage of retrospective studies is that one can capture a delineated period at the end of life (e.g. last 3 months of life) across the sample because the moment of death is known, and that sampling frames for retrospective studies (e.g. death registries) allow researchers to obtain representative population-based samples. However, major disadvantages of using retrospective research in isolation include a lack of first-person reports on well-being and specifically on less observable experiences in the areas of psychosocial and existential well-being, where proxy reports have uncertain validity, 77 as well as the inability to study changes over time. This project incorporates the longitudinal prospective and retrospective methods and thus collects both first-person and proxy reports on experiences at the end of life. Combining the two methods helps in overcoming the limitations of the retrospective studies, especially with respect to recognising the unique patient experiences that often go unexplored.
A further important methodological contribution of this project will be data on the appropriateness of disease-specific inclusion criteria for deteriorating health to identify people who are in the last months of life. One key obstacle in prospective research on the end of life is identifying those who will die within a given period. For several chronic diseases, we needed to develop new criteria for deteriorating health in the absence of previous examples. This project will provide survival data for the various criteria and hence important methodological guidance for the design of future prospective research on the end of life. Our longitudinal study will also provide much-needed information on the circumstances under which repeated assessments in relatively short intervals (i.e. 2 months) over 1 year can be done in a feasible and acceptable way in a population of older people who are in poor health. Prior to the main study, we will pilot all work packages (except for WP3, as we do not expect deaths to occur over a piloting period of 2 months) to test and, if needed, modify research procedures and materials.
Finally, this longitudinal study uncovers commonalities and differences through a convergent mixed-methods design that is highly innovative in its approach to integration. It was found that mixed-methods research in palliative and end-of-life care often reports insufficiently on the specific methods and procedures used to integrate the quantitative and qualitative data. 78 The same analysis also showed that one-quarter of mixed-methods studies failed to report any evidence of integration. Most of these were convergent mixed-methods studies, where qualitative and quantitative findings were reported separately without a holistic integration of the two. The TRAJECT project dedicates a work package to mixed-methods integration through two specific methods, triangulation and the following-a-thread method. Particularly the latter has not been applied frequently 70 yet holds much promise for gaining novel insights that are ‘more than the sum’ of the contributions of each individual method. As the project progresses, we will also publish a methodological paper on the use of the following-a-thread method to inform other researchers on its use and strengthen the robustness of mixed-methods research in our field.
A further strong point of the interdisciplinary mixed-methods approach of this project is that it gives equal ‘weight’ to the qualitative and quantitative components. Oftentimes in mixed-methods research, the quantitative component is used to determine what is generalisable, while the qualitative component is meant to elucidate what is specific and subjective.29,71,79 Our approach will show that both methods can achieve both, each through their unique lens. It will also show that qualitative and quantitative methods can each study objective and subjective phenomena (e.g. objective presence of a disease; subjective reports of symptoms and well-being)
Clinical and public health impact
By reconciling the general and the specific in the end-of-life trajectories, the research project primarily aims at shifting the focus from the clinical factors that have been understood to shape and label the end-of-life trajectories to the psycho-socio-clinical factors, dynamic in nature that actively reconfigure these trajectories. Through the convergent mixed-methods design, it weaves together measurement and meaning and thus offers a more holistic understanding of end of life by embedding trajectories in people’s social and material world. The TRAJECT project has the potential to change how we think about end-of-life trajectories and will likely have an important impact on future research projects. For instance, our findings will have the potential to guide new means of identifying target groups for palliative care interventions based on combinations of characteristics and experiences that are more indicative of shared trajectories than underlying disease alone.
Next to impact on research, the project’s findings will set the stage for innovations in health service planning and individual patient care. A better knowledge of end-of-life trajectories will be critical for setting priorities for deploying healthcare resources. It will aid in developing large-scale prevention and intervention programmes relevant to the end of life, including but not limited to palliative care and advance care planning. One of the key clinical impacts of this research will be to uncover the medical, social, psychological and contextual determinants of well-being at the end of life. Understanding these determinants and their effect on end-of-life trajectories could help healthcare providers to better anticipate the needs of the different patient groups at different periods, thus enhancing their well-being. This could furthermore contribute to identifying risk groups for burdensome trajectories and developing specialised and targeted interventions, including needs-based and patient-centred criteria for specialist palliative care referral. The clinical and health service impact will concern diverse patient populations. It will be particularly pronounced for those included in our project that have been relatively under-researched in palliative care, such as older people who are nearing the end of life due to heart failure or advanced chronic liver disease.
Conclusion
This ERC-funded project will lead to a new understanding of the varied ways in which older people’s end-of-life trajectories unfold based on the circumstances and experiences that shape them, paying equal attention to what is shared and what is individually specific. It challenges the over-simplification of diverse end-of-life aspects and over-reliance on clinical perspectives. The project focuses on the multiple factors that could variously affect the end of life, including people’s social world as well as the meanings and processes through which they navigate health and illness, alongside clinical determinants. These new insights will provide a pressingly required evidence base concerning groups at risk of poor well-being as they near death. This will significantly inform the palliative care practice, needs assessment and health service planning aiming to address the needs of older people in diverse societies.
Footnotes
Acknowledgements
We would like to thank ERC for funding the TRAJECT project. We are also grateful to the clinicians who participate in this project for facilitating patient identification and recruitment and for their valuable advice concerning study methods and inclusion criteria. Thank you to the Advisory Board members of this project – Caroline Nicholson, Annemarie Samuels and Sigrid Sterckx – for their valuable input concerning project aims and methodology.