
Abstract
Background:
End-of-life care for patients with advanced cancer can impose a significant financial burden. However, data on the economic impact of end-of-life care in low- and middle-income countries are limited.
Objective:
This study aims to compare the costs associated with palliative care units (PCUs) and non-PCU settings for cancer patients in Iran.
Design:
We designed a retrospective study at the largest hospital in the country.
Methods:
We conducted a comprehensive evaluation of hospitalization costs and care service delivery for 150 patients in the final 5 days of life, who were admitted to the largest hospital complex in Iran. All costs were adjusted based on the 2018 USD exchange rate.
Results:
Among the 150 patients included in the study, 56 (37%) were admitted to the PCU. The average total treatment cost during the final 5 days of life was three times higher in general wards compared to PCUs. In non-PCU settings, the total cost of care during this period amounted to $2873, while in PCU settings, it was $909.63.
Conclusion:
The establishment of PCUs within tertiary hospitals and the provision of palliative consultation services to patients with advanced cancer can yield significant benefits, even when resources are limited.
Plain language summary
An economic study about the cost of last five days of cancer patients in two different hospital ward, to show the importance of establishing palliative care in cancer hospitals in Iran, a low- and middle-income country in point of view of health economic. Why was the study done? There was only one hospital with palliative care setting in the country. Unfortunately in 2020 because of COVID-19 pandemic and the policy of hospital to use beds for COVID patients the PCU ward was closed and we tried to show the role of PCU and the importance of opening the ward again. What did the researchers do? The research team studied the cost of services that patients received during their last days of their life in PCU and non-PCU. What did the researchers find? Among the 150 patients included in the study, 56 (37%) were admitted to the PCU. The average total treatment cost during the final five days of life was three times higher in general wards compared to PCUs. In non-PCU settings, the total cost of care during this period amounted to $2873, while in PCU settings, it was $909.63. What do the findings mean? This study showed that having PCU in hospitals could save money and reduce the futile services.
Background
Cancer is one of the costliest diseases around the world, accounting for a great share of the economic burden in any country. According to the GLOBOCAN 2020 estimates, the incidence and mortality rates of all cancers were 19,292,789 and 9,958,133 worldwide, respectively. 1 Approximately 13% of personal healthcare costs are attributed to the last year of life in cancer patients due to hospitalization and the need for intensive care unit (ICU) admission. 2 In a study conducted by Li et.al., in China, data from 894 cancer patients revealed that the costs of treatment were US$ 18,234, US$ 13,043, US$ 6349, and US$ 2085 in the last 6 months, 3 months, and 1 month, and 1 week of life, respectively. In this study, the authors reported that the cost of healthcare increased dramatically as the patient’s death approached. 2
In Iran, the corresponding numbers of incidence and mortality were 131,191 and 79,136 cancer patients, respectively. The total cost of some cancers has been estimated in Iran, including colorectal cancer ($298,148,718), oral cancer ($64,245,173), breast cancer ($947,374,468), and gynecological cancers ($51,000,000).3 –6
In 2016, Cagle et al. studied the financial burden of end-of-life care among cancer patients’ families in the United States. They concluded that overall, cancer costs affect all family members and consume nearly all family savings, even when the patient is insured. 7
Palliative care is best started after cancer is diagnosed, but usually, it is suggested when physicians declare that there are no curative options for patients with advanced cancer, and palliative care can be used to minimize both the patient’s pain and the cost of treatment. 8 It has been shown that palliative care improves the quality of life of patients with serious end-stage diseases at the end of life. Palliative care services reduce patients’ symptoms and eliminate the need for medical interventions and non-beneficial imaging, which can increase the quality of life of patients, their families, and physicians compared to non-palliative care unit (PCU) services.8,9 People with advanced cancer need to reduce symptoms such as pain, nausea, vomiting, and shortness of breath. The palliative care could manage these symptoms. 10
The PCUs can reduce the healthcare costs of patients at the end of life by avoiding inappropriate or futile treatments.11 –14 Therefore, increasing the number of PCUs can lead to greater cost avoidance for the patients and the healthcare system, alongside improving the quality of life for patients approaching the end of life. 15 The total cost of care delivery in the last 3 days of life was estimated at $1340.60 in the PCU setting versus $9467.78 in a tertiary hospital setting in Australia. 16 Overall, PCUs lead to cost savings by reducing the length of hospital stay (LOS) and the intensity of treatment. 17 However, most of these examinations and cost-estimation studies have been conducted in high-income countries, and a lack of evidence to support the cost-effectiveness of PCUs in low- and middle-income countries is a potential barrier to their accessibility. 18
The economic evaluation studies conducted on cancer costs in Iran have not estimated the cost of palliative care due to the limited number of PCUs in the country.3 –6
In 2020, during the COVID-19 pandemic, based on the limitation to the use of beds for COVID-19 patients, the PCU ward was closed and we tried to show the role of PCU and the importance of it to open the ward again. We aimed to determine whether implementing PCUs in tertiary hospitals can reduce the cost and burden of cancer care and to evaluate and compare the cost of care in the last 5 days of life for cancer patients in general wards.
Methods
Study design, setting, and patient selection
This was a retrospective study. The perspective of the study was based on payers.
We conducted a retrospective study at Imam Khomeini Hospital Complex (IKHC), the largest hospital in Iran between 2015 and 2018. Iran Cancer Institute (CI) is a multidisciplinary specialized hospital for cancer patients located in IKHC. It is the first hospital with a PCU in the country, established in 2015 with six beds. Patients with cancer were either treated or diagnosed in the CI or IKHC. Factors those patients referred to CI or IKHC were based on patient entries to the hospital and the physician’s decision. If the entry of the patient was a general hospital, the patient was admitted to a non-PCU, if the patient’s entry was CI, based on CI’s protocol it may refer to PCU. The cost data of patients admitted to the PCU of CI were abstracted and compared with the data of cancer patients admitted to IKHC in any unit. We only selected cancer patients who died in the PCU of CI or the non-PCU setting of IKHC, and we calculated the cost of care and interventions in the last 5 days of life. Most patients admitted to the palliative ward of CI were in the last days of their lives. Patients who died within less than 5 days of admission were excluded from the study. Based on the inclusion criteria, we included a total of 56 patients in the PCU setting and 94 patients in the non-PCU setting between 2015 and 2018.
To ensure that our method section is complete, we have followed the CHEERS 2022 checklist based on the EQUATOR guideline (https://www.equator-network.org/). The completed checklist is attached in the Supplemental File.
Data extraction
We calculated the cost and number of services the patients received in the last 5 days of life. The study variables included sex, age, cancer type, cancer morphology, file number, type of insurance, date of admission, date of death, hospitalization date, days of ICU stay, cost of hospitalization, frequency of hospitalization, consultation, imaging, laboratory tests, interventions, and prescribed medications.
Data analysis
We used Stata (Ver. 16; Stata Corp, College Station, TX, USA) for all statistical analyses. Data were not normally distributed, and we performed nonparametric tests to determine statistically significant differences between the groups concerning the variables under study. A p value of 0.05 was considered statistically significant. We examined the differences in costs using the Wilcoxon signed-rank test. Moreover, we performed a correlation analysis using Spearman’s rank correlation test to assess the relationship between care cost and type of ward. We conducted a Mann–Whitney test to examine the association between the sociodemographic variables and the type of wards. The median values are presented as interquartile range (IQR) between Q1 and Q3. Since healthcare inflation was highly unstable between 2015 and 2018, we converted all costs based on the exchange rate from the US Dollar (USD) to the Iranian Rial in 2018 (one USD equaled 43,888 Rials in 2018).
Results
A total of 150 patients were included, 63 of whom (42%) were female. The total number of patients in the PCU was 56. The mean age of female and male patients was 53.42 and 54.67 years, respectively. The variables of sex and age had no significant relationships with the type of ward. Table 1 presents the demographic status of the patients.
The demographic characteristics of the participants stratified by the hospital unit.

IQR, interquartile range; PCU, palliative care unit.
The average number of visits by physicians was 3.78 in the PCU setting and 2.18 in the non-PCU setting. The average number of laboratory tests in the non-PCU setting was 2.15 times higher than that of the PCU setting. The number of consultation visits, medications, and imaging procedures was lower in the PCU compared to the non-PCU setting. These results were statistically significant according to the type of hospital ward (Table 2).
The mean value and IQR of variables stratified by the hospital unit.

We have to use the median for LOS in ICU instead of the mean value, because of a wide range of LOS (30–188 days).
ICU, intensive care unit; IQR, interquartile range; LOS, length of hospital stay; PCU, palliative care unit.
According to Table 3 and Figure 1, the average total cost of treatment in the last 5 days of life was $2872.69 for each patient in the non-PCU setting and $909.63 in the PCU setting (almost three times lower). The cost of medications was nine times higher in the non-PCU setting compared to the PCU. We found that six patients admitted to non-PCU received one course of chemotherapy in the last 5 days of their life.
The mean values of cancer cost (USD) and IQR in the last 5 days of life stratified by the hospital ward.
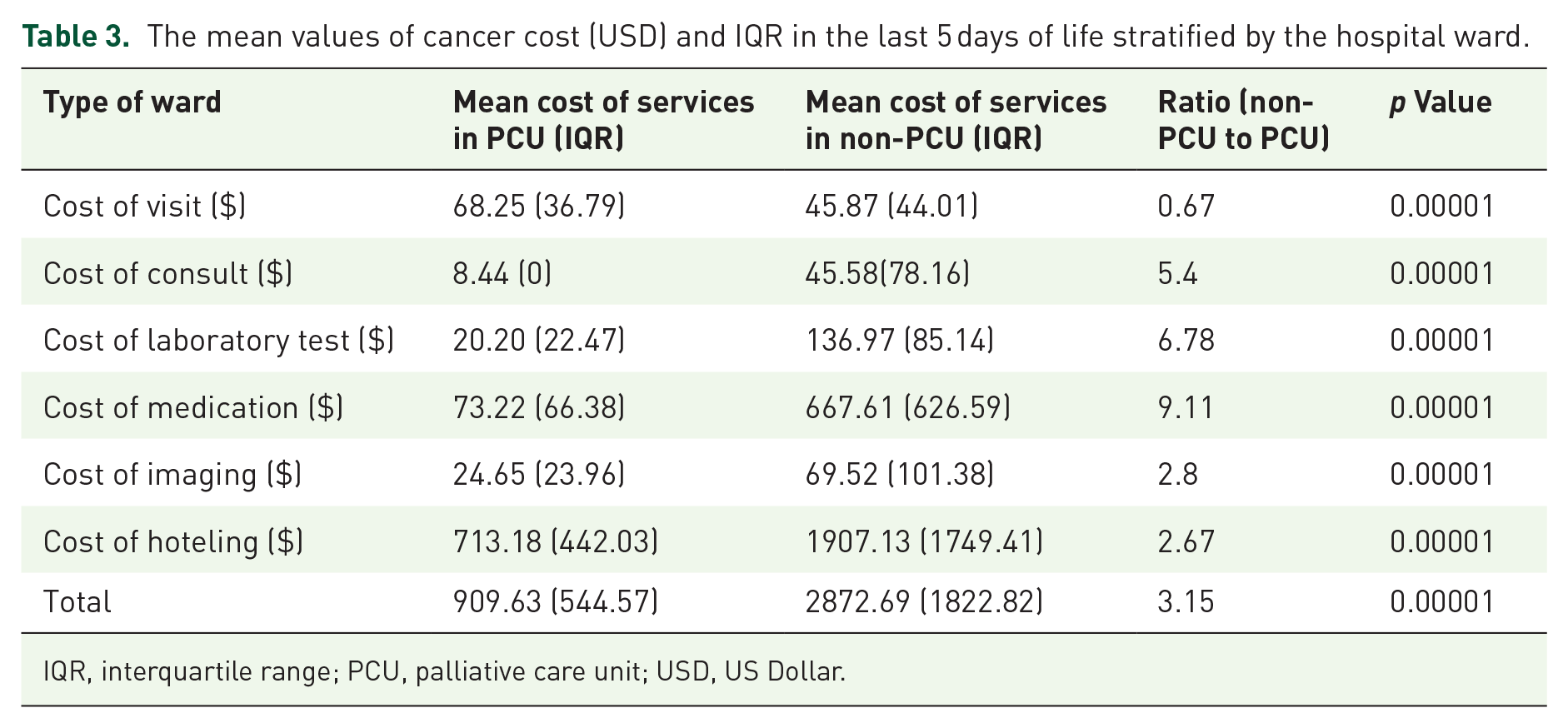
IQR, interquartile range; PCU, palliative care unit; USD, US Dollar.

The mean values of cancer cost (USD) in the last 5 days of life based on the hospital unit.
The most significant difference in cost was related to hoteling expenses, with $1907 in the non-PCU setting and $713 in the PCU; according to this comparison, all costs were significantly different.
Overall, 54 out of 94 patients (57%) in the non-PCU setting were hospitalized in the ICU. The median LOS in the ICU was 37 days in the non-PCU setting, while no patients in the PCU were admitted to the ICU. We used the median for LOS in ICU instead of the mean value because of the wide range of LOS (30–188 days). Evaluation of palliative consultation for patients admitted to the non-PCU setting showed that only three patients had an order of palliative consultation in their records.
Table 4 shows that 36 patients diagnosed with hematopoietic cancer (leukemia and lymphoma) died in non-PCU.
The frequency of patients based on the type of cancer.

PCU, palliative care unit.
Discussion
Our results indicated cost savings in the PCU setting compared to the non-PCU setting for patients with advanced cancers. Overall, hospitalization of patients in the last days of life to the PCU can lead to lower costs for both hospitals and patients. The average cost of care in the last 5 days of life was 3.15 times lower in the PCU compared to the non-PCU setting. The total cost of care for patients admitted to the PCU was $909.63 versus $2872.69 for patients admitted to other hospital wards.
The most significant difference in cancer costs was related to hotel expenses. 2 In our study, 57% of patients in the non-PCU setting were hospitalized in the ICU, and the cost of ICU stay was the highest. The implementation of PCU could be beneficial for the patients in their last month of life. In our study, people who received palliative care services spent less money on care services compared to those who received other services. Similarly, in a systematic review of 46 studies, the results showed that PCUs were less costly than other approaches. 19 Jox et al. in Germany designed a study to show what is the futile treatment and when was applied by care providers. They explained that emotional explanations such as guilt, grief, legal aspects, and family reactions are the reasons for futile treatment. Also, organizational customs, insufficient legal and palliative knowledge, and treatment requests by patients or families are the other reasons. 20 Unfortunately, there is no “Advance Care Planning” in Iran. However, Heng et al., 21 in the United States, showed that encouraging patients to have their Advance Care Planning could avoid admission to the ICU and thus could reduce the cost of hospitalization and futile treatment.
This study was performed in a public hospital, and most patients had public insurance (they were mostly insured). Patients with public insurance tended to use more expensive services and had extended ICU stays for recovery. Tangka et al. 22 declared that private insurance reduced the LOS from 9.5 to 8.5 days compared to public insurance. The costs of medication, laboratory tests, and ICU admission significantly reduced when patients died in PCUs, compared to the non-PCU setting. Overall, a net saving of $4908 in direct costs per admission (p = 0.003), along with a saving of $374 in direct daily costs (p = 0.001), was reported. Significant cost savings can be achieved by setting clear care goals, which can lead to the selection of an effective treatment by the patient’s family and help achieve these goals and avoid unnecessary interventions. 23 Based on international guidelines, most advanced cancer patients did not need to be admitted to ICU. Unfortunately, due to a lack of recognition of palliative care, patients transfer to the ICU without receiving any effective services till they die. 24
Medication order costs in non-PCU settings were nine times higher than in PCU settings, indicating that the medications used were expensive and their benefits questionable. As noted in our results, six patients received chemotherapy, which could explain the increased medication costs in non-PCU settings.
In a study by West et al. 25 in Italy, 75% of hospital patients received three or more potentially ineffective medications during their last 3 days of life, compared to 42.6% in hospice care. Another study by Vallard et al. in France observed 1091 cancer patients in PCUs and evaluated the use of non-anticancer medications. The findings revealed that patients were administered strong opioids (74%), corticosteroids (51%), and antidepressants (21.8%) until death. In addition, prescriptions included antiulcer agents, antibiotics, thrombosis prevention, antidiabetics, and transfusions. 26 Since imaging for advanced patients has no diagnostic value, it can be only justified by the management of acute symptoms, assessment of disease progression, and evaluation of the effects of treatment; the latter can help assess whether treatment should be discontinued or changed. Although there are currently available guidelines, diagnostic imaging remains controversial. Massa et al. 27 in Italy concluded that in the last month of life, most patients had received at least one imaging procedure without improving their survival.
In the current study, PCUs had a higher frequency and cost of daily visits compared to non-PCU settings. We recorded the cost of daily visits in the patient’s file only when the attending physician visited, not the resident. Powel et al. and Balaban in their studies showed the role and importance of PCUs. During daily visits to the PCU, the attending physician managed the patient, met with the patient’s family, and communicated with the patient; these visits were crucial in the last days of a patient’s life.28,29
Generally, palliative care consultations improve the quality of life for patients. The results revealed that few patients benefited from palliative care consultations during their hospital stay. Salama et al. 30 demonstrated that staff education and documenting the consults could enhance the goals of care from 59% to 83% in patients with palliative intent.
The greatest share of costs in the non-PCU setting was ICU admission. There are no differences between the hotel expenses of PCU and non-PCU wards for the last days of life unless patients are admitted to the ICU. In palliative care, the general concept is not to refer patients to ICU but in non-PCU wards, some patients are referred to ICU. If there is no PCU, palliative consultation can reduce the cost of patient management. 31 It is known that the improvement of the patient’s quality of life and their dignity and comfort is the main goal of palliative care. Besides reducing hospital costs, palliative care protects patients and their families against financial difficulties due to disease and disability. 32
According to Table 4, most people admitted to non-PCU had hematological cancers. However, based on the definition of palliative care and the National Comprehensive Cancer Network guidelines, there is no difference in managing the palliative symptoms between cancers. 33 In a study conducted by Ulrich Wedding in 2021, the author explained that the low number of research in palliative care in hematologic malignancies comparing solid cancers. However, the author concluded that these patients could benefit from end-of-life care. 34
To the best of our knowledge, this is the first study evaluating the economic benefits of PCU implementation in Iran. This study, however, had some limitations. First, based on the inclusion criteria and the lack of PCUs in Iran, the sample size was small. We had an obligation to design our study as case series and we could not design a randomized study for this purpose. Second, only the cost of care for advanced cancer patients who died in the hospital was estimated, while the cost of care in the last 5 days of life in patients who died in their homes could not be calculated.
Conclusion
Palliative care is not dependent on prognosis, though end-of-life care is a crucial component. It offers an alternative to disease-modifying and life-sustaining treatments of questionable value by supporting decision-making based on the patient’s care goals. Implementing PCUs can reduce costs in the final days of life for cancer patients, making it a cost-effective option for referral hospitals. In the absence of resources to establish PCUs, palliative consultations or adherence to palliative care guidelines, along with symptom management, can help manage the financial burden of cancer care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241299819 – Supplemental material for Financial cost of end-of-life cancer care in palliative care units (PCUs) and non-PCUs in Iran: insights from low- and middle-income countries
Supplemental material, sj-docx-1-pcr-10.1177_26323524241299819 for Financial cost of end-of-life cancer care in palliative care units (PCUs) and non-PCUs in Iran: insights from low- and middle-income countries by Ali Darrudi, Amir Hossein Poupak, Rajabali Darroudi, Nasrin Sargazi, Kazem Zendehdel, Libby Sallnow, Ali Ghanbari Motlagh, Mamak Tahmasebi and Azin Nahvijou in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.